
Abstract
Abstract
Objective:
The primary objective of this research was to assess the efficacy of intrathecally administered low-dose morphine and bupivacaine as analgesic modalities for patients undergoing total laparoscopic hysterectomy (TLH) under general anesthesia and the effects of these agents on perioperative humoral stress markers.
Design:
Prospective, randomized, double-blind controlled study.
Materials and Methods:
Forty-seven American Society of Anesthesiologists I–II female patients scheduled for elective TLH under general anesthesia were randomized into 3 groups. Patients in Group B (n = 15, bupivacaine-only) received a subarachnoid block (SAB) with 5 mg of bupivacaine; patients in Group M (n = 16, morphine) received a SAB with 5 mg of bupivacaine and 200 μg of morphine. Patients in Group C (n = 16, control) received skin infiltration with a local anesthetic alone. Blood samples for testing levels of plasma cortisol, growth hormone (GH), insulin, and adrenocorticotropic hormone (ACTH) were taken at 8
Results:
Patients in Groups C and B had significantly greater pain at rest and on movement in the postoperative period, compared to patients in Group M. Patients in Group M required significantly lower doses of fentanyl (175 μg) than patients in Group B (350 μg) and Group C (425 μg) during 24 hours of observation (p = 0.0001). There was a significantly lower rise in ACTH, cortisol, and GH, and maintenance of insulin levels in the intraoperative and postoperative samples in group M, compared to Group C. The incidence of PONV and pruritus was high in Group M, compared to Groups B and C, but this was not statistically significant (Fisher's exact test: 0.45 and 0.33, respectively). No patients in Group M had respiratory depression.
Conclusions:
Preinduction administration of low-dose intrathecal morphine resulted in better postoperative analgesia up to 24 hours, leading to a significant reduction of parenteral opioid consumption during the perioperative period without a significant increase in side-effects. Intrathecal morphine also resulted in a significant decrease in surgical stress, compared to what occurred in the control group. (J GYNECOL SURG 34:77)
Introduction
H
Surgery and pneumoperitoneum during laparoscopy1,2 induces an endocrine stress response that might lead to complex neurohumoral, immunologic, and metabolic changes. Although the stress response is a defense mechanism, it can produce undesirable effects, if the response is prolonged and amplified. If the response is overwhelming, it results in a systemic inflammatory response that could lead to multiorgan failure and even death. Prolonged activation of the immunologic system leads to depletion of cytokines and other inflammatory mediators, producing an immunosuppressed state.3.The severity of this stress response depends on a variety of factors, such as severity and duration of surgical trauma, postoperative pain, anesthetic method, and surgical technique. Abolition of the stress response could reduce perioperative morbidity and mortality, improve outcomes, and decrease the length of hospital stays, thus reducing the total cost of patient care. 4
Intrathecal morphine has emerged as an effective form of perioperative analgesia for many major laparoscopic procedures, notably the colorectal procedure.5–7 To date, there is no study that has analyzed pain after laparoscopic hysterectomy. The current study was designed to assess the efficacy of intrathecally administered low-dose morphine and bupivacaine as analgesic modalities in patients undergoing laparoscopic hysterectomy under general anesthesia and their effects on perioperative humoral stress markers.
Study design
This was a prospective, randomized, double-blind controlled pilot study performed after getting Institutional Ethical Committee approval.
Materials and Methods
The institutional review board of the All India Institute of Medical Sciences, New Delhi, India, approved this study. This trial was registered in Clinical Trials Registry—India (CTRI) as CTRI/2015/11/006370. All patients provided informed written consent. Forty-five American Society of Anesthesiologists (ASA) classes I–II patients ages 25–65, who were scheduled to undergo elective total laparoscopic hysterectomy (TLH) under general anesthesia, were included in this prospective, randomized, double-blinded controlled study. Patients who refused to provide informed consent or refused spinal anesthesia, as well as patients with coagulation disorders (or undergoing treatment with anticoagulants), severe spinal deformities, infection at the injection site, symptomatic cardiac and/or respiratory disease were excluded from the study. In addition, patients who were not capable of understanding how to use a patient-controlled analgesia (PCA) device use were also excluded.
A computer-generated random-number list was used to prepare serially numbered opaque envelopes and was kept with one of the investigators who was not participating in the postoperative pain assessment. A member of the anesthetic team (who was not the investigator) opened an envelope assigned for the serial number of each patient and the patient was randomly allocated to one of three groups. Patients in Group B (n = 15, bupivacaine-only) received a subarachnoid block (SAB) with 5 mg of bupivacaine. Patients in Group M (n = 16, morphine) received a SAB with 5 mg of bupivacaine and 200 μg of morphine. Patients in Group C (n = 16, control) received skin infiltration with a local anesthetic over L-3–L-4 after cleaning and draping (this was a “sham” block). The injections for the SABs were prepared by an anesthesiologist who was not involved in pain assessment or patient care. The specific interventions given were unknown to the patients and the anesthesiologists in intraoperative care and postoperative pain assessments.
Enrolled patients underwent complete evaluations (histories, physical examinations, and biochemical and hematologic tests). The patients were instructed in the use of a visual analogue scale that was marked from 0 cm to 10 cm (0 = no pain and 10 = worst possible pain) and the use of the PCA device. A blood sample for plasma cortisol, growth hormone (GH), insulin, and adrenocorticotropic hormone (ACTH) was taken at 8
General anesthesia was induced after the regional procedure. All patients received standardized anesthetic induction consisting of 2 mg/kg of propofol and 2 μg/kg of fentanyl for induction. After muscle relaxation was achieved with 0.1 mg/kg of vecuronium, the trachea was intubated with an appropriate size endotracheal tube. Anesthesia was maintained with air, oxygen, and isoflurane to maintain a minimum alveolar concentration of ∼1. Intraoperatively, all patients received 1 μg/kg/hour of a fentanyl infusion from induction of pneumoperitoneum until termination of pneumoperitoneum. Thirty minutes after initiation of pneumoperitoneum, blood samples for testing plasma cortisol, GH, insulin, and ACTH were collected in appropriate tubes.
If a patient's heart rate and/or mean arterial pressure increased by >20% from baseline, 1 μg/kg of fentanyl was given in an IV bolus. Thirty minutes before the end of surgery, all patients received 1 g of IV paracetamol and 100 μg/kg of ondansetron. Any residual neuromuscular blockade was reversed with standard doses of neostigmine (50 μg/kg) and glycopyrrolate (10 μg/kg). The trachea was extubated after the patient had good respiratory effort and airway reflexes. All patients were shifted to the postanesthesia care unit (PACU) for further monitoring, observation, pain measurement, and rescue analgesia.
In the PACU, all patients were connected to a PCA fentanyl infusion capable of delivering a 25-μg bolus with a lock-out time of 10 minutes and a maximum dose of 150 μg/hour without any basal infusion. The first pain assessment was performed as soon as each patient was awake, oriented, and capable of following instructions. VAS scoring was performed every 2 hours for a period of 8 hours and again at 24 hours. Postoperative blood samples for stress markers were taken 1 hour after the end of the surgery. In any patient who had pain (VAS >3), even with use of the PCA, a 25-μg IV bolus of fentanyl was repeated until the patient was pain-free. The number of episodes of postoperative nausea and vomiting (PONV) was recorded and rescue antiemetic treatment was provided. The next morning, the PCA device was removed and number of times the PCA was activated and the total amount of fentanyl consumed were noted.
Statistical analysis was carried with Stata 11.1 software. Data were represented as mean with standard deviation, and qualitative data were compared by applying χ2/Fischer's exact test. The quantitative data was compared by an analysis of variance followed by a posthoc comparison by the Bon-Ferroni method. p-Values <0.05 were considered significant.
Results
A total of 54 patients who fulfilled the inclusion criteria were approached to participate in the current study from January 2013 to June 2014. Seven patients refused to give consent for participation in the study and the participation of 2 patients was withdrawn due to conversion of their operations to laparotomies. Finally, data from 45 patients were analyzed (Fig. 1). There were no significant differences among the groups with respect to demographic characteristics and surgical data (Table 1). In general, the VAS at rest in the postoperative period was less in Group M, compared to Group B and Group C at all timepoints of observation. Patients in Group B had clinically minimal pain at 0 and 2 hours. The median VAS at these times (0 hour (2 [1–4]) and 2 hours (2 [1–3]) in Group B was comparable to the VAS at corresponding times in Group M. However, in the remaining observation period (4, 6, 8, and 24 hours) the VAS in Group B was significantly higher than that in Group M. At 0 hour, VAS in Group C was significantly higher than both Group B and Group M (p = 0.02 and 0.002, respectively).
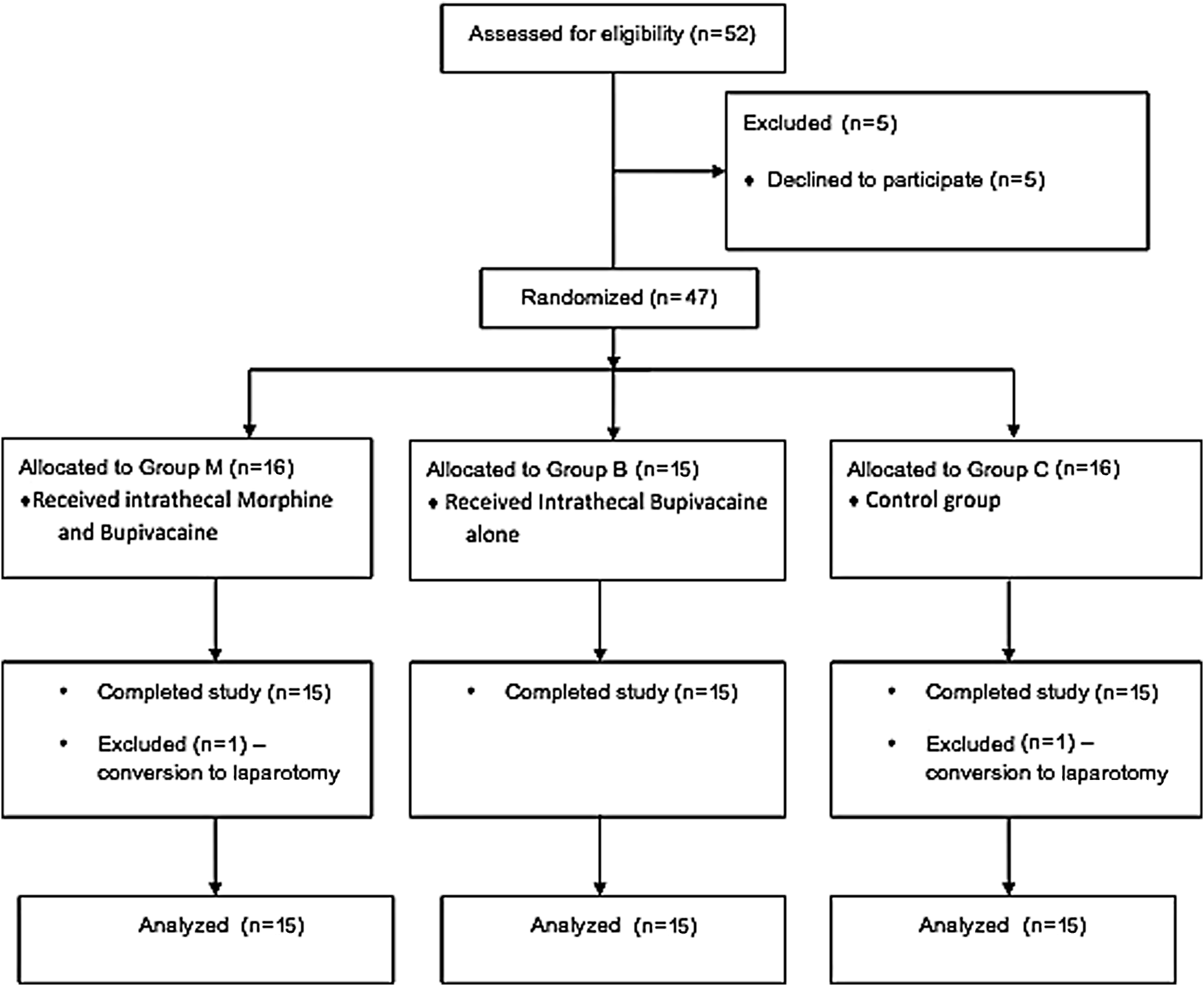
Consolidated Standards of Reporting Trials (CONSORT) flow diagram. Patient flow (according to CONSORT chart).
Fisher's exact test.
Group allocations: M, group who received bupivacaine, morphine, and a subarachnoid block; B, group who received bupivacaine and a subarachnoid block; C, control group who received skin infiltration with a local anesthetic alone.
SD, standard deviation; ASA, American Society of Anesthesiologists.
However, the VAS at rest from 2 hours onward was comparable between Group B and Group C. The VAS on deep breathing and turning (movement) followed the same pattern as those at rest. VAS on movement was significantly higher at all points of observation in Group C, compared to Group M. In contrast, VAS on movement was comparable at all observation points between Groups B and C except at 0 hour. VAS on movement was comparable between Groups B and M (3 [0–6] and 4 [3–6]), respectively; p = 0.12. VAS at rest and on movement are shown in Figures 2 and 3. The median (min–max) amount of total fentanyl (in μg) consumed in the postoperative period at 24 hours in Group M, Group B, Group C were 175 (50–250), 350 (275–450), and 425 (200–600), respectively, which was statistically significant (p-value: 0.0001; Fig. 4)
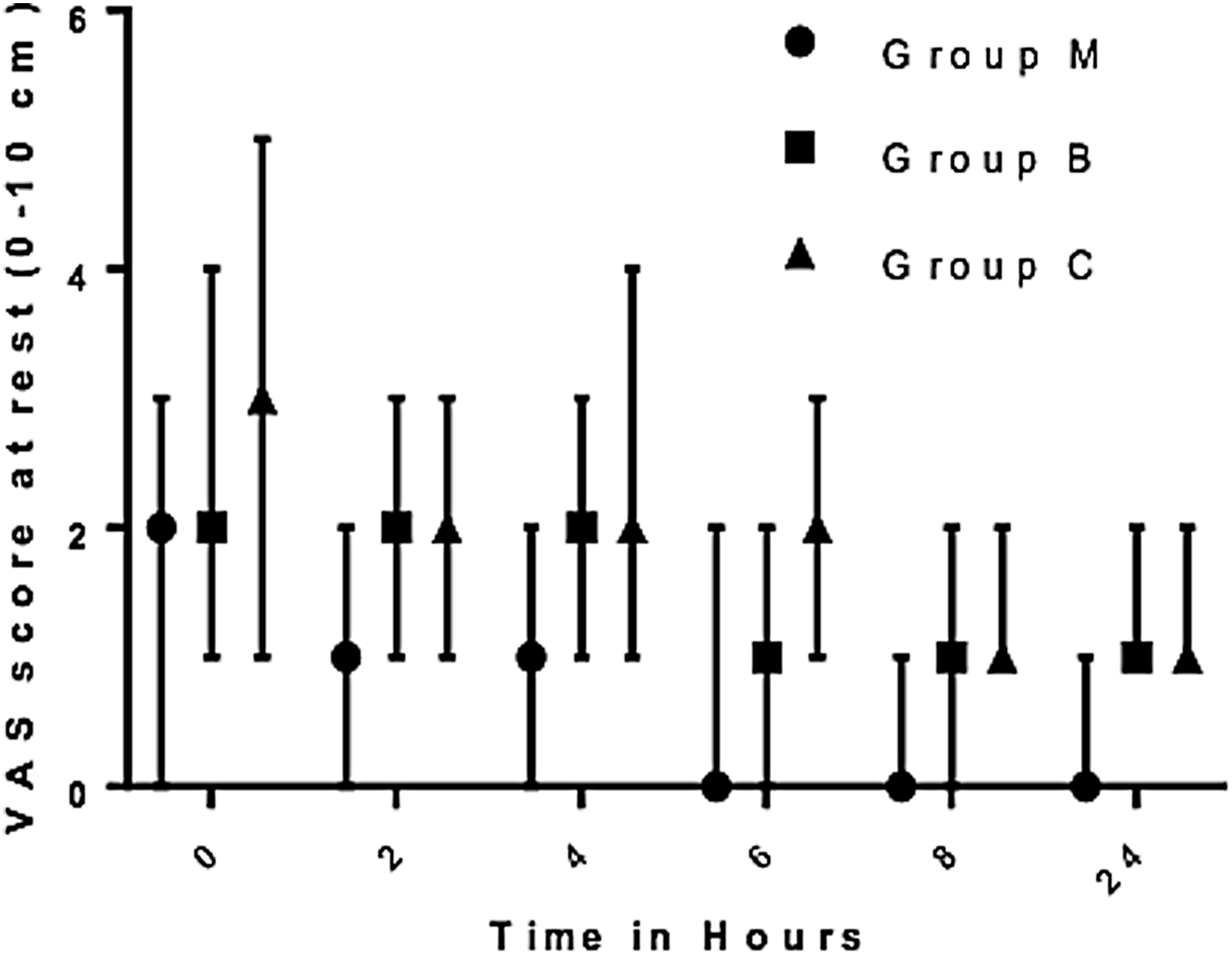
Visual analogue scale scored at rest for the 3 groups. Group M—intrathecal morphine; Group B—intrathecal morphine + bupivacaine; Group C—control. Values are expressed as median with interquartile range.
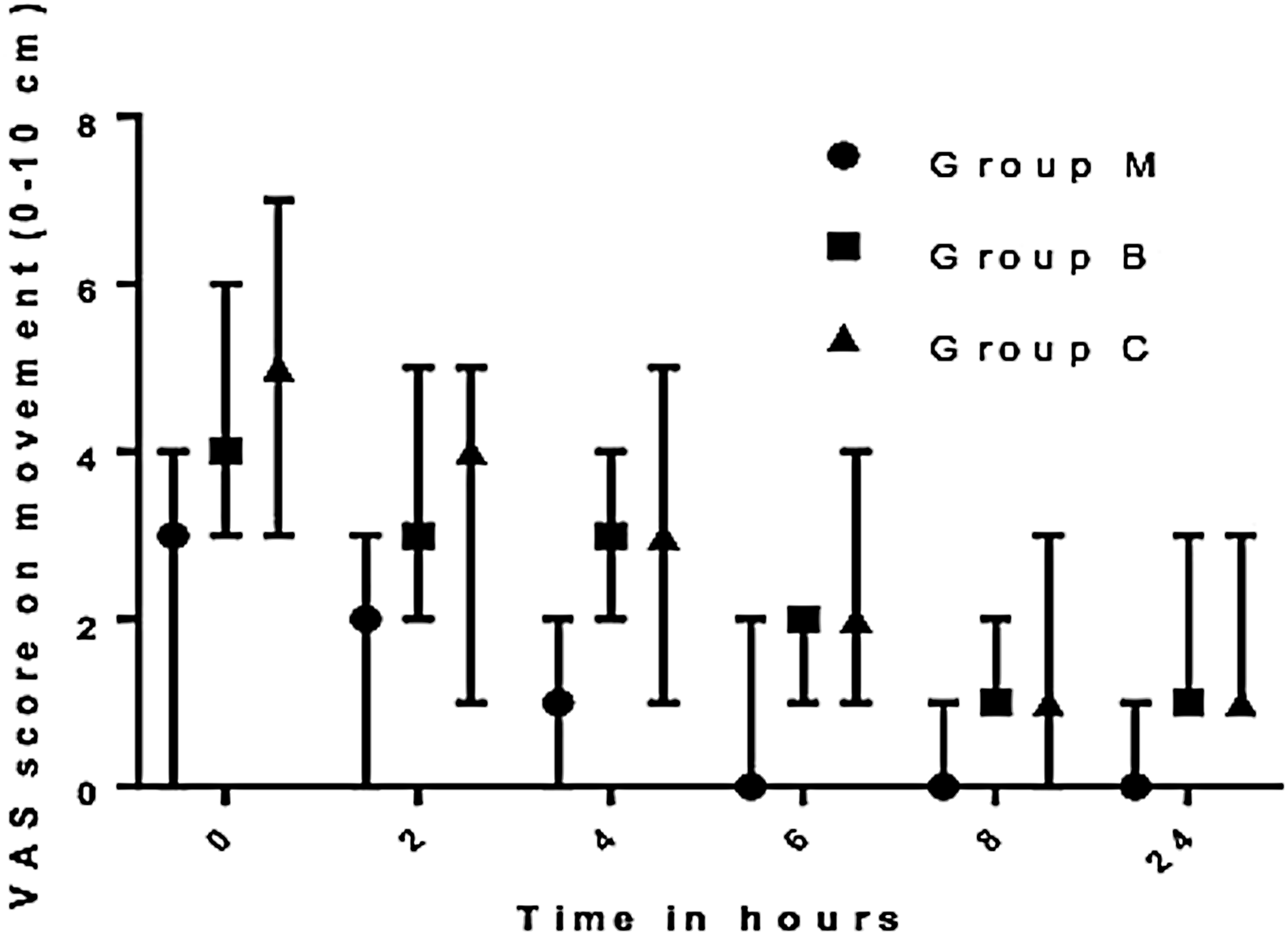
Visual analogue scale scores on movement for the 3 groups. Values are expressed as median with interquartile range.
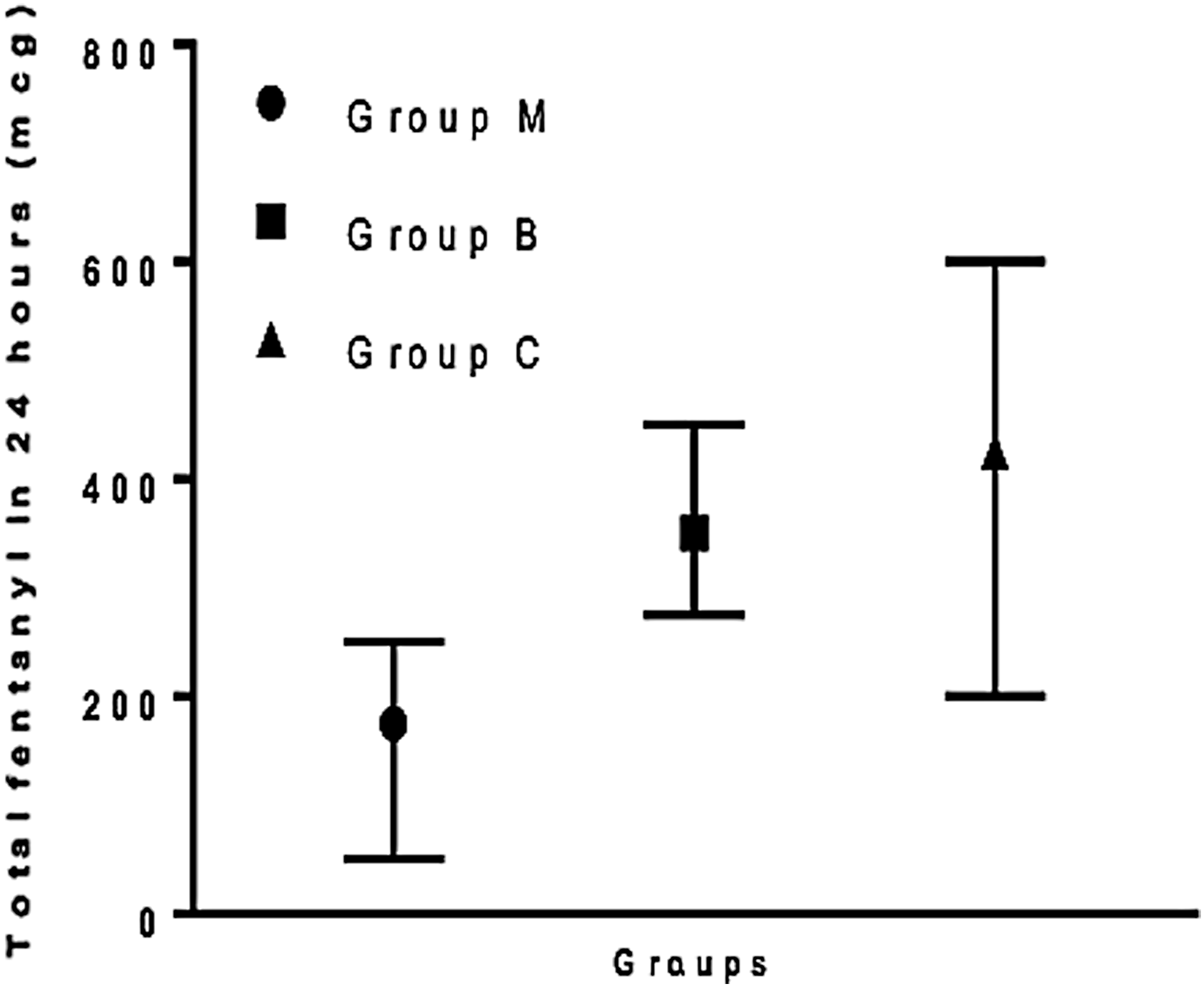
Postoperative fentanyl consumption for the 3 groups. Values are expressed as median with interquartile range.
Increase in intraoperative and postoperative values of plasma ACTH, cortisol and GH in Group C were significantly higher, compared to corresponding values in Group M; Fall in intraoperative and postoperative insulin levels was more in Group C, compared to Group M, although this was not statistically significant. Although the median levels of cortisol, ACTH, and GH in Group B in the intraoperative and postoperative samples remained higher than those in group M, the values did not attain statistical significance. This also demonstrated that spinal analgesia with bupivacaine alone also ameliorated the endocrine stress response to laparoscopy, albeit to a lesser extent than the intrathecal morphine (ITM)–bupivacaine combination. The values are given in Table 2. Although the incidence of PONV and pruritus was more in Group M, compared to Group B and Group C, the difference did not reach statistical or clinical significance (Tables 3 and 4). There was no incidence of respiratory depression noted in any of the patients included in the study.
p < 0.05 was considered significant; see bolded p-values.
Group allocations: M, group who received bupivacaine, morphine, and a subarachnoid block; B, group who received bupivacaine and a subarachnoid block; C, control group who received skin infiltration with a local anesthetic alone.
min, minimum; max, maximum; ACTH, adrenocorticotropic hormone; GH, growth hormone; op, operation.
p < 0.05 was considered significant.
Group allocations: M, group who received bupivacaine, morphine, and a subarachnoid block; B, group who received bupivacaine and a subarachnoid block; C, control group who received skin infiltration with a local anesthetic alone.
p < 0.05 was considered significant.
Group allocations: M, group who received bupivacaine, morphine, and a subarachnoid block; B, group who received bupivacaine and a subarachnoid block; C, control group who received skin infiltration with a local anesthetic alone.
Discussion
Reduced postoperative pain is frequently cited as one of the significant advantages of laparoscopic surgery, compared with open surgery. However, there is evidence in the literature that pain can be significant after most types of laparoscopic surgery. Visceral pain is most intense on the first day and disappears in 24 hours 8 ; shoulder-tip pain is severe and uncomfortable, persisting for 2–3 days postoperatively. Peritoneal inflammation induced by pneumoperitoneum during pelvic laparoscopy may cause upper abdominal pain after the procedure. 9
In the current study, patients who received ITM had consistent and significantly less pain at rest and on movement throughout the period of observation. In contrast, the control group experienced significantly worse pain than both the bupivacaine-only group and the bupivacaine + morphine group. These results also confirm that addition of ITM to bupivacaine confers more superior analgesia for pain management up to 24 hours, compared to intrathecal bupivacaine alone. These findings are also in agreement with the results from Motamed et al.'s study, 10 which compared the analgesic efficacy of low-dose ITM with isobaric bupivacaine in patients undergoing elective laparoscopic cholecystectomy. The reduction in VAS translated directly into a difference in PCA fentanyl consumption. In the current study, opioid consumption was reduced by 50% in the morphine + bupivacaine group, compared to the bupivacaine-only group, and by 62%, compared to the control group. This effectively highlighted the opioid-sparing nature of low-dose intrathecal morphine in patients undergoing TLH. The opioid-sparing effect of ITM in laparoscopic surgery has been demonstrated in other studies also.5,6
Modification of the stress response to surgery results in potential beneficial effects on surgical outcome. Patel et al., 11 in a recent review of patients undergoing laparoscopic surgery for colorectal malignancy, stated that an exaggerated stress response has been associated with postoperative bowel dysfunction; fatigue; delayed wound healing; and infectious complications, such as wound infection, anastomotic leak, and cardiopulmonary complications. Activation of the endocrine response is initiated in afferent stimuli; blocking these impulses may inhibit the stress response. The efficacy of combining neuraxial anesthesia—with or without opioids—in attenuating surgical stress over general anesthesia has been the subject of considerable research. The efficacy of intrathecal morphine for depressing the neuroendocrine stress response following TLH has not been evaluated before. Although only a few studies have involved laparoscopy directly, the role of epidural and intrathecal morphine in attenuating the metabolic and humoral response to surgical stress is evident in the literature.
In 2006, Karaman et al., 12 in a randomized controlled trial, concluded that ITM was effective for depressing the stress response in patients undergoing TAH under general anesthesia. Similarly, Liu et al., 13 in a meta-analysis, showed that ITM reduced mortality, ischemia, and dysrhythmia, but without statistical significance after coronary bypass surgery. The results of the current study demonstrated that significantly lower rises in ACTH, cortisol and GH; and maintenance of insulin levels in the intraoperative and postoperative samples in the M group, compared to the C group highlights the efficacy of the ITM + bupivacaine combination in attenuating the surgical stress of patients undergoing TLH under general anesthesia. These results also demonstrated that spinal analgesia with bupivacaine alone also ameliorates the endocrine-stress response to laparoscopy, albeit to a lesser extent than the ITM–bupivacaine combination.
Incidence of dose-related side-effects, such as PONV and pruritus, was high in the ITM group but was not statistically significant. An incidence of nausea and vomiting as high as 50%–74% has been reported in other studies. The incidence of PONV is only 33.33% in the current study, because all patients received prophylaxis with metoclopramide on the day of surgery and injections of 4 mg of ondansetron every 8 hours were administered in the postoperative period. Given that all of the patients in the current study were catheterized, per the surgical protocol, it was not possible to assess the incidence of urinary retention. However, following removal of the catheter no patient complained of urinary retention.
PONV is rated as one of the most unpleasant symptoms following general anesthesia. A study was conducted by Yazigi et al. in 200314 to assess the efficacy of 8 mg of ondansetron for preventing ITM- and sufentanil-induced PONV in patients undergoing cesarean section under general anesthesia. That study showed that the incidence of PONV was significantly reduced in an intervention group, compared to a placebo group (18% versus 48%). The dose of ITM use in that study was 100 μg. The higher incidence of PONV in Group M (33.33%) in the current study, compared to that observed by Yazigi et al., 14 even with ondansetron prophylaxis, could be attributed to the higher dose of ITM (200 μg) in the current study versus the 100 μg in Yazigi et al. 14 study.
A study by Imeh (2014) demonstrated a significant reduction in PONV with a dexamethasone–ondansetron combination, 16 which was previously found to be ineffective (Szarvas, 200316). Although there is little evidence that dexamethasone could be effective for preventing PONV in patients undergoing laparoscopic surgery, the current authors did not use dexamethasone prophylaxis in the current study because cortisol levels were used as one of the markers of surgical stress. Negative feedback to the hypothalamic-pituitary-adrenal axis caused by dexamethasone administration decreases serum cortisol levels.
The incidence of pruritus in a meta-analysis performed by Meylan et al. in 2009 17 to assess the risk and benefit of ITM in patients undergoing major abdominal surgery was 21.4% in that study's ITM group, compared to 5.3% in the study's placebo group. The incidence of pruritus in the current study was similar to that described by Meylan et al.
Respiratory depression is a grave complication of perioperative opioid use. No events of respiratory depression were noted in any of the patients included in the current study. Gehling et al. in 2009 18 performed a meta-analysis to find the frequency of side-effects in patients receiving ITM in combination with local anesthesia, compared to placebo. It was observed in the study that, in patients who received <300 μg of ITM, no episodes of respiratory depression were observed.
Given that all of the patients in the current study were catheterized per the surgical protocol and the urinary catheter retained in-situ till the end of the study period, it was not possible to assess the incidence of urinary retention, if any, caused by the use of PCA opioids or ITM. However, following removal of the catheters, no patients complained of urinary retention.
Conclusions
Preinduction administration of low-dose ITM resulted in better postoperative analgesia up to 24 hours, leading to a significant reduction in perioperative parenteral opioid consumption without a significant increase in side-effects. ITM also resulted in a significant decrease in surgical stress, compared to what occurred in the control group.
Footnotes
Acknowledgments
The authors acknowledge the help provided by the statisticians at A.I.I.M.S.: Dr. Kalaivani, Dr. Guresh Kumar, and Mr. Ashish Datt Upadhyay.
Author Disclosure Statement
The authors declare no conflicts of interest in association with this study.