
Abstract
Abstract
Background:
An advanced abdominal pregnancy with a live fetus is a very rare event with only a few cases reported in the literature. This kind of pregnancy is associated with significantly high maternal and perinatal mortality.
Case:
A 40-year-old woman, para 4, with an intra-abdominal pregnancy was managed conservatively up to 34 weeks of gestation, when she was delivered via laparotomy.
Results:
Subsequently, both the mother and her infant had favorable maternal and fetal outcomes.
Conclusions:
This case is reported to highlight its successful outcome despite the difficulties in diagnosis and management in a low-resource setting such as the current authors'. (J GYNECOL SURG 34:102)
Introduction
E
Case
A 40-year-old woman, gravida 8, para 4+3 (4 alive), presented at the Accident and Emergency Department of the Lagos University Teaching Hospital in Lagos, Nigeria, at 29 weeks of gestation with a 3-day history of progressively worsening abdominal pain. The pain was described as sharp; it was initially localized to the right side of the abdomen but later became generalized. The pain severity was described on a scale as 7 (out of 10) and was said to be aggravated by fetal movement, which this patient still perceived adequately at the time of presentation. She had no bleeding per vaginum, no drainage of liquid, and no gastrointestinal or urinary symptoms. There was no history of early pregnancy uterine instrumentation.
During a physical examination, this patient was anxious-looking but not in obvious painful distress. Her vital signs were within normal limits and her cardiovascular and respiratory systems did not reveal any abnormalities. There was mild generalized tenderness noted on her abdominal examination, with a fundal height of 26 cm and easily palpable fetal parts. An abdominal ultrasound (US) scan performed prior to presentation had shown a live fetus at 29 weeks gestational age, in a transverse lie, within the upper abdominal quadrants, with the fetal head lodged in between the spleen and left kidney and the lower limbs floating freely in the right lumbar region. The uterus was empty with an endometrial lining of 2 mm, and the placenta appeared to be attached to the fundus.
The patient was counseled on the findings, stabilized, and managed conservatively over the next 5 weeks. She had weekly US scans and biophysical profiles performed to monitor the fetal growth and well-being. She was subsequently scheduled for an exploratory laparotomy at 34 weeks of gestation. Preoperative magnetic resonance imaging (MRI) showed a fetus lying freely in the peritoneal cavity. The placenta was located superior to the uterine fundus (Fig. 1). She had 6 units of blood crossmatched in anticipation of hemorrhage. General surgeons were also invited to observe the surgery.
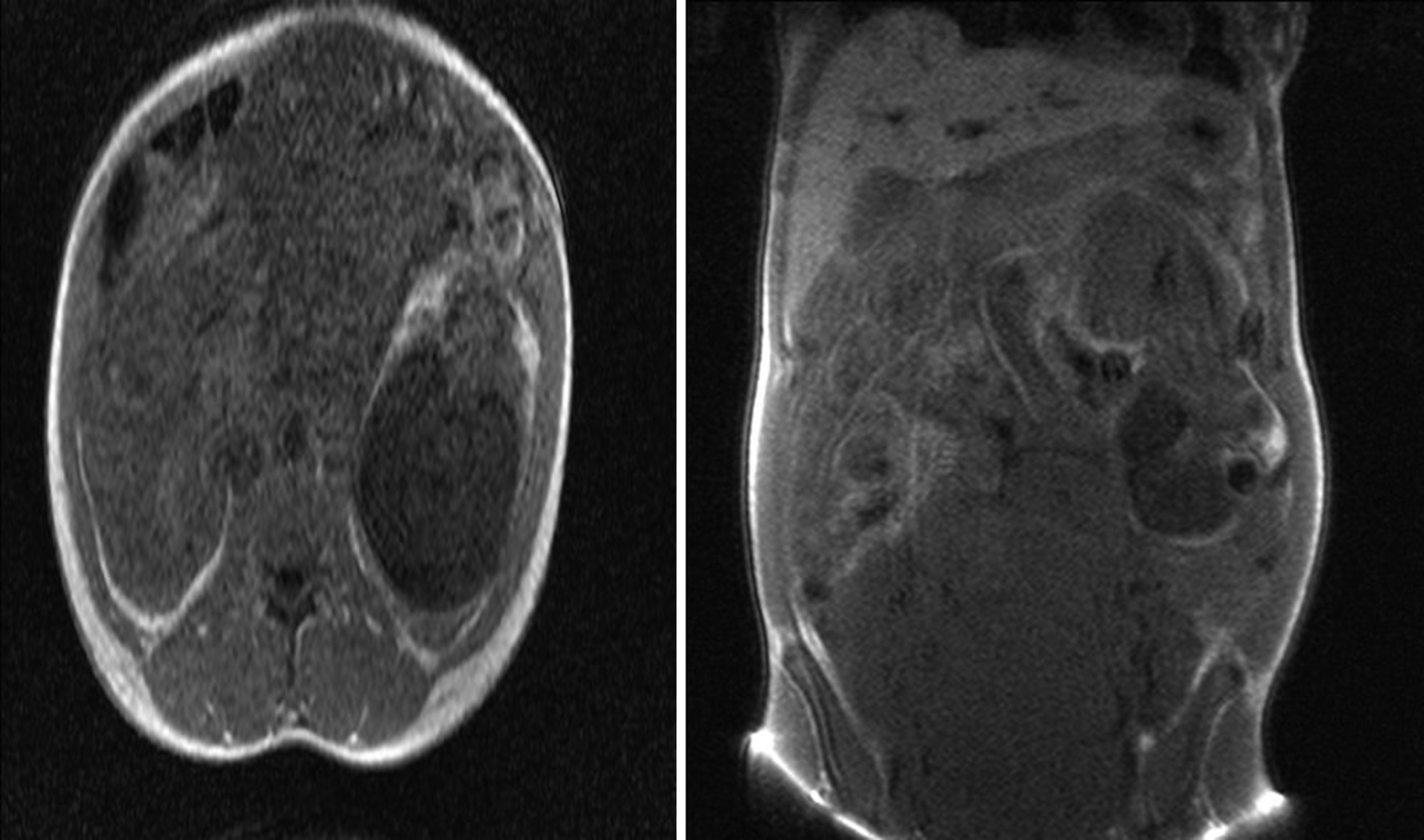
Preoperative magnetic resonance imaging showed a fetus lying freely in the peritoneal cavity.
Findings at surgery included a live male fetus, lying transverse within the peritoneal cavity and surrounded by omentum. The infant's birth weight was 2.5 kg, and his Apgar score was 6 and 8 at 1 and 5 minutes, respectively. No anomaly was seen on this infant. The placenta was extensively attached to the omentum, large bowel, and uterine fundus. The umbilical cord was doubly ligated close to the placenta and then left in situ. The uterus, fallopian tubes, and ovaries appeared to be normal. The patient's intraoperative blood loss was 600 mL, and she did not require transfusion.
Results
This patient's postoperative period was uneventful, and she was discharged to go home with her infant 10 days after her surgery. She was seen 2 and 6 weeks postpartum with serial abdominopelvic US scans showing progressive reductions in the placental size and no demonstrable flow on color Doppler. Her qualitative beta–human chorionic gonadotropin (ß-hCG) at the sixth week of follow-up was negative and the ultrasound scan at 6 months did not show the placenta.
Discussion
Due to the widely uncommon nature of abdominal pregnancy, a high index of suspicion is necessary for prompt diagnosis and appropriate management. 3 The incidence of abdominal pregnancy varies among geographic regions but is found more in developing countries.7–9 The reported incidences were 1 in 10,000 deliveries in the United States 8 ; 1 in 654 in Ibadan, Nigeria 9 ; and 1 in 1320 in Kumasi, Ghana. 7 The incidence is also said to be higher in multiparous women and women of low socioeconomic status. 9
Abdominal pregnancy is classified as primary or secondary. Primary abdominal pregnancy is said to occur when implantation of the fertilized ovum is directly within the peritoneal cavity. 3 In such cases, according to the Studderford criteria, the ovaries and fallopian tubes appear to be normal, there is no uteroperitoneal fistula, and the pregnancy is exclusively on the peritoneal surface.3,10 Secondary abdominal pregnancy is the more common of the two classifications, when there is a secondary implantation of a primary tubal pregnancy in the peritoneal cavity. 7 Primary abdominal pregnancy is rarely seen. 4 The patient in this report was a multiparous woman of low socioeconomic status who had features that were in line with a secondary abdominal pregnancy, as the attached placenta on the uterine fundus suggested the possibility of an early extrusion of pregnancy through the uterine fundus although this patient did not give any history of uterine instrumentation in early pregnancy.
A clinical feature of abdominal pregnancy is most commonly abdominal pain 11 ; however features range from being asymptomatic to acute abdomen, fetal malpresentation, easily palpable fetal parts, and/or fetal demise.3,8,10 Ultrasonography is a very important tool in the diagnosis of an extrauterine pregnancy, while other radiologic tools, such as MRI and computed tomography scans, are also very helpful but, unfortunately, are not readily available or affordable in most third-world countries. Thus, a high index of suspicion is needed for prompt diagnosis and timely intervention to prevent life-threatening complications. 7
Potential treatments of abdominal pregnancy consist of surgery with termination of the pregnancy (removal of the fetus) via laparoscopy or laparotomy, use of methotrexate, embolization, and combinations of these. Sapuri and Klufio 12 indicated that conservative treatment is also possible if the following criteria are met: there are no major congenital malformations; the fetus is alive; there is continuous hospitalization in a well-equipped and well-staffed maternity unit that has immediate blood-transfusion facilities; there is careful monitoring of maternal and fetal well-being; and placental implantation is in the lower abdomen away from the liver and spleen. The choice is largely dictated by the clinical situation but, generally, treatment is indicated when the diagnosis is made. The current patient met all the criteria for conservative management and was subsequently delivered by laparotomy at 34 weeks of gestation.
Major hemorrhage from the placental implantation site is often the most common cause of maternal mortality and, as such, the decision to remove or leave the placenta in situ depends on the extent of placentation and skills of the surgeon.4,7 It is usually recommended to leave the placenta in situ and monitor the patient's ß-hCG levels. 12 MRI has been used with success to plan for surgery,11,13—just like what occurred with the current patient, who had a preoperative MRI to ascertain the location of her fetus and placenta—and thus provide a necessary guide for the surgeons by ensuring the availability of certain additional interventions to forestall complications.
Conclusions
An abdominal pregnancy with a healthy newborn is a rare occurrence. For abdominal pregnancies diagnosed before 20 weeks of gestation, termination is usually advised; however, an advanced abdominal pregnancy is managed expectantly with the aim of delivery at 34 weeks of gestation when fetal lung maturity is certain. Removal of the placenta is for well-selected cases and is usually dependent on findings during surgery as well as the skills of surgeon; otherwise, it is advised to leave the placenta in situ. However, standardization of treatment principles for advanced abdominal pregnancy, perioperative treatment options, and postoperative management measures would improve newborn survival, and reduce complications and mortality.
Footnotes
Acknowledgments
The authors appreciate the assistance given to us by all the medical record staff of the Lagos University Teaching Hospital and the resident doctors of the hospital's Department of Obstetrics and Gynecology.
Author Disclosure Statement
The authors declare that no competing interests exist in connection with the publication of this article.