
Abstract
Abstract
Objectives:
The goals of this study were to: (1) scrutinize cases of Müllerian anomalies (MuAs) diagnosed intraoperatively, for the first time, during emergency operations: (2) categorize the various MuAs; and (3) compare the presentations of the different subclasses.
Materials and Methods:
For this retrospective cohort study, the records of all the obstetric surgeries performed in the emergency operation theater of the Pt. B. D Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India, were examined from January 2012 to May 2017. All the cases for which MuAs were identified intraoperatively were noted and classified according to the latest ESHRE/ESGE Classification. The MuA classes and subclasses were analyzed in terms of reproductive characteristics, perinatal complications, and association with past adverse outcomes.
Results:
A total of 12,935 emergency obstetric surgeries were performed, and the prevalence of MuAs was 1.3%. The most frequent MuA subtype encountered was hemiuterus at 57.4% (class U4). There was a significant difference in the rate of preterm deliveries and preterm premature rupture of membranes in the index pregnancies between these classes (p = 0.002 and p < 0.0001, respectively). Furthermore, the various classes differed significantly in associated malpresentations; Classes U1 and U2 were least associated with breech (p = 0.001) presentations but were most associated with transverse lie (p < 0.0001). Life-threatening conditions were significantly higher in patients with class U4a undergoing laparotomy than cesarean sections (p < 0.0001).
Conclusions:
MuAs, although often associated with benign conditions, can present as catastrophic obstetric events. Timely diagnosis and rectification of certain malformations, especially class U4a, is essential and lifesaving. (J GYNECOL SURG 34:138)
Introduction
F
Various classification systems exist for female reproductive-tract anomalies, but a new updated classification system based on anatomy has been proposed by the European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy (ESHRE/ESGE). 1 Most MuAs are found incidentally during work-ups for various obstetric and gynecologic problems. Sometimes, the associated conditions are ignored and the diagnosis is made only intraoperatively during surgery. Moreover, different types of MuAs are associated with different reproductive events. The present study was conducted to categorize the various MuAs diagnosed during emergency obstetric surgery and to compare the presentations and perinatal outcomes of the different uterine anomalies.
Materials and Methods
Design
This was a retrospective cohort study in the setting of a tertiary-care teaching hospital. The study was carried out at the Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana, India, from January 2012 to May 2017. The case records of women who underwent emergency obstetric surgeries in the emergency operation theater of this institute, during the study period, were examined. Women who were found to have any type of MuA at the time of surgery were included in the study. From the records, the demographic details of the women, and their presenting complaints, periods of gestation, obstetric histories, antenatal histories, intrapartum courses, intraoperative findings, postoperative courses, and neonatal outcomes were noted.
The uterine anomalies were classified according to the recent ESHRE/ESGE classification system in which the main class is based on the deviation of uterine anatomy, subclassses are designated according to the degree of uterine deformity, and cervical and vaginal anomalies are classified separately in a coexistent class. 1 Table 1 illustrates the ESHRE/ESGE classification system of female genital tract anomalies.
Class U1c or others, which is added to include all minor deformities of the uterine cavity, including those with an inner indentation at the fundal midline level of <50% of the uterine wall thickness, such as arcuate uterus.
ESHRE/ESGE, European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy.
The cases in which MuAs were diagnosed at the time of cesarean section were grouped further (for ease of comparison) according to the types of defects and ESHRE/ESGE Classes as follows:
Group I—Formation defects: hemiuterus (Class U4) Group II—Fusion defects: bicorporeal uterus (Class U3) Group III—Normal fusion but abnormal absorption of septum: dysmorphic and septate uterus (Classes U1 and U2)
Statistical analysis
The results were analyzed in terms of reproductive characteristics, perinatal complications, and associations with past adverse outcomes among these groups.
All of the statistical analyses were carried out using the Statistical package for the Social Sciences, IBM version 19.0. Data were expressed as mean, standard deviation (SD), or frequencies and percentages. p-Values were calculated using two types of tests for two types of data, continuous and categorical. The Kruskal–Wallis test was used for independent samples' median, which has been used for continuous data, and Fisher's exact test was used for categorical data. A p < 0.05 was considered to be statistically significant.
Results
A total 12,935 emergency obstetric surgeries were performed during the study period from January 2012 to May 2017 (11,765 cesarean sections and 1170 laparotomies). Of all the obstetric surgeries, MuAs were found intraoperatively in a total 169 cases, making the prevalence of this condition in the present study 1.3%. Of these MuAs, 159 cases were diagnosed during cesarean sections, while the rest were diagnosed during laparotomies (Fig. 1).
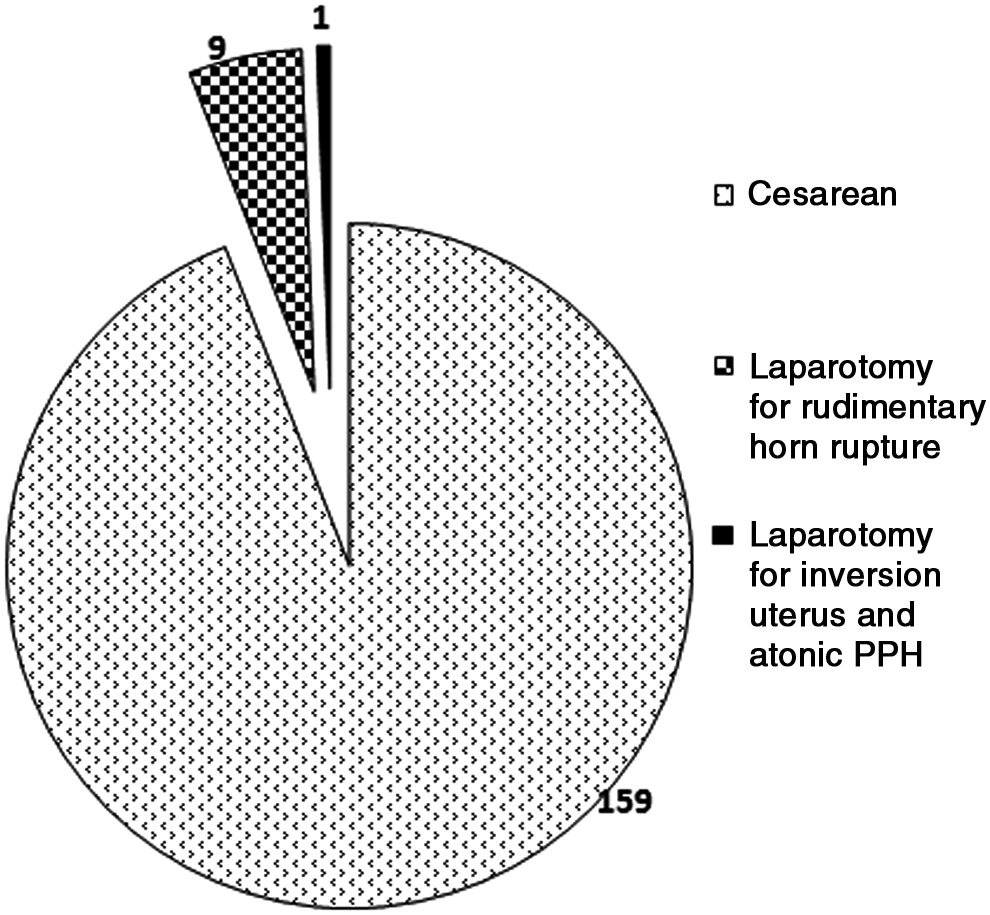
Type of surgery during which Müllerian anomalies were diagnosed (n = 169).
The uterine malformations during cesarean sections were diagnosed for the first time intraoperatively. Although these women had undergone previous antenatal ultrasound (US) scanning for fetal anomalies, there were no comments in regard to any uterine anomalies.
The mean age of women with MuAs was 25.0 ± 3.3 (19–35) years. The demographic and obstetric characteristics are as shown in Table 2. Among these women, there were histories of miscarriages and preterm deliveries in 22.5% and 17.7% of the patients, respectively.
MuAs, Müllerian anomalies.
All of the MuAs found were classified according to the ESHRE/ESGE classification system. 1 The frequency of different classes and subclasses is enumerated in Table 3. The most commonly encountered uterine anomaly among them was Class U4 (hemiuterus), which accounted for almost half of the MuAs (57.4%). Hemiuteri with rudimentary horn (RH) cavities were more common than without such cavities. Figure 2 shows an intraoperative finding of a hemiuterus without an RH (U4b). Class U2 (septate uterus) was the second most-common class of genital-tract anomaly (16.5%). In 1 case it was associated with a cervical septum (C1) and a longitudinal vaginal septum (V1). Figure 3 shows a partial septate uterus (U2a), wherein a septum divides the uterine cavity above the level of the internal cervical os. In 15% of the cases of bicorporeal uteri, there were associated double cervices (C2). In all cases of hemiuterus with RH, excision of the RH and ipsilateral salpingectomy was performed.

Intraoperative picture of hemiuterus without rudimentary cavity (European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy [ESHRE/ESGE] Class U4b).

Intraoperative picture of partial septate uterus (European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy [ESHRE/ESGE] Class U2a).
Arcuate uteri in the present study.
All laparotomy cases had Class U4a anomaly.
MuAs, Müllerian anomalies; ESHRE/ESGE, European Society of Human Reproduction and Embryology/European Society for Gynaecological Endoscopy.
According to the different types of formations and fusion defects, the ESHRE/ESGE classes were grouped and compared with respect to different obstetric characteristics, modes of presentation, complications, and perinatal outcomes (Table 4). The 3 groups were similar with respect to their demographic characteristics and past obstetrical histories. The rate of preterm deliveries (< 37 weeks) was statistically significant (p = 0.002) but not when prematurity <32 weeks was considered. Preterm premature rupture of membranes (PPROMs) in the index pregnancies was significantly more prevalent in group III (p < 0.0001).
Kruskal–Wallis test for independent sample medians was used to study the difference among the groups.
Bold denotes statistical significance (p < 0.05).
MuAs, Müllerian anomalies; PPROMs, preterm premature rupture of membranes: HDU, high-dependency unit.
Of the total cesarean sections performed during the study period, the most-common malpresentations were breech (1405; 11.9%) and transverse lie (153; 1.3%), respectively. MuAs were detected in 7.6% of breech (108) and 9.1% transverse lie (14) cases. Breech cases were significantly higher (p < 0.001) in groups I & II, whereas transverse lie cases were higher in group III MuAs (p < 0.0001).
The obstetric characteristics and perinatal outcomes were also compared among the two subtypes of class U4 (hemiuterus) with or without RH but no statistically significant difference was found.
MuAs were found in 0.85 % cases of the total 1170 emergency laparotomies performed during the study period. Nine of the 10 laparotomies were performed for ruptured RH pregnancies. In all of these cases, except 1, ultrasonography (USG) was performed only at the time of presentation in the emergency department. There was no previous USG record diagnosing the condition. One case of RH was an already admitted patient misdiagnosed as having an “intrauterine” fetal death and who was undergoing induction with misoprostol. Although that patient had US earlier, it failed to reveal the RH pregnancy. There was 1 interesting case of laparotomy that was performed for a uterine inversion coupled with uncontrolled atonic postpartum hemorrhage, wherein the finding of an RH was incidental.
The majority of women with RH pregnancies (70%) presented with life-threatening hypovolemic shock necessitating massive blood transfusions. The difference in life-threatening conditions (requiring blood transfusions) was statistically significant when Class U4a was compared between cesarean sections and laparotomies (p < 0.0001).
Discussion
Müllerian-duct anomalies are often undiagnosed until an unfavorable reproductive or gynecologic event occurs. Sometimes these malformations may go unnoticed, to be discovered for the first time during a laparotomy or cesarean section. There are studies that have evaluated reproductive outcomes in women with MuAs, but these studies examined cases in which these MuAs were diagnosed during work-up for one or another gynecologic or obstetric condition. The present study is different from earlier studies in a number of ways. It takes into account only those cases of MuAs that were encountered during emergency obstetric surgeries. This involves diagnosis of an MuA by direct inspection wherein even minor malformations would be noticed. Furthermore, the present study takes into account the latest ESHRE/ESGE classification system of different classes and subclasses of malformations. 1 In addition, the current authors attempted to categorize the MuAs that were found into three different groups according to their anatomical defects and etiologies, and then compare the obstetric and perinatal outcomes among these groups. A similar comparison of uterine defects was performed in a systematic review by Chan et al. 3
There has been a great variation in the prevalence rate of MuAs, ranging from 0.06% to 38%. 4 A prevalence of 1.3% was noted in the current study, which involved women who had undergone emergency obstetric surgeries. Although the prevalence during cesarean sections was higher (1.3%) than during laparotomies (0.85%), life-threatening conditions were more common in MuAs diagnosed during laparotomies (70% versus 3.7%). Chan et al. reported the prevalence of uterine anomalies as 5.5% (95% confidence interval [CI]: 3.5–8.5) in an unselected population and 24.5% (95% CI: 18.3–32.8) in patients with miscarriage and infertility. 5
Hemiuterus (Class U4) was the most commonly occurring uterine anomaly (57.3%) detected intraoperatively during cesarean sections and laparotomies, followed by septate uterus (class U2). Some studies have reported arcuate uterus being the most common uterine malformation, while others have found septate uterus most often.6,7 Chan et al. observed arcuate uterus as the most common anomaly in an unselected population and septate uterus in a high-risk population. 5 This may be explained by the fact that the study populations were different in the different analyses.
Obstetric complications, including rate of preterm deliveries and PPROMs, were significantly more prevalent in Classes U1 and U2 (group III). A pooled analysis of 5 studies by Chan et al. showed a significant increase in rate of preterm births and increased rates of first-trimester miscarriages in patients with canalization defects that included subseptate or septate uteri (corresponding to Class U2). 3 There are a number of hypotheses explaining the poor reproductive performance in this group, namely lack of proper implantation due to abnormal endometrium and lack of adequate vascularization over the septum, reduced uterine capacity, and uncoordinated contractions, explaining the risk of preterm labor and malpresentations.3,8–10
Significant differences were found regarding fetal malpresentations at delivery among the classes. Transverse lie was found significantly more in Classes U1 and U2. This might be due to the altered shape of the uterine cavity in septate and dysmorphic uteri (arcuate uteri). Classes U3 (bicorporeal uterus) and U4 (hemiuterus) had significantly higher rates of breech presentations. The narrow, elongated cavity in these classes favors longitudinal lie rather than transverse lie (cf., U1 and U2). A retrospective study by Hua et al. concluded that the odds ratio of the fetus in breech presentation was 8.6 in women with MuAs, compared to women with normal uteri (95% CI: 6.2–12.0; p < 0.01). 11
In the present study, 76.9% cases of life-threatening events were associated with Class U4a (hemiuterus with RH). Three-fourths of the patients with RH pregnancies presented with shock and with catastrophic events. In all of the cases of incidentally discovered RHs, prophylactic excision of the horn along with ipsilateral salpingectomy was performed. One of the cases of a ruptured RH pregnancy with shock had a previous history of cesarean section, emphasizing the need for RH removal whenever first encountered to prevent future catastrophes. A detailed US examination in the first trimester of pregnancy could be useful for its timely diagnosis although its sensitivity is low. Magnetic resonance imaging is especially useful when a doubt arises in the diagnosis of an RH pregnancy. Although this condition is quite rare, given the high maternal morbidity it causes, early and timely diagnosis is of prime importance.
Conclusions
Depending on the type and the degree of anatomical distortion, MuAs are associated with health and reproductive problems. 1 Certain subclasses of MuAs are associated with poorer reproductive outcomes than others. The presence of a MuA might often go unnoticed until a serious complication occurs. This is especially true in cases of Class U4a (hemiuterus with rudimentary cavity). Timely diagnosis and rectification is essential and life-saving. At the time of an antenatal US scan, uterine anomalies should also be noted and documented, as they could have important obstetric implications. Moreover, detection of an MuA may help in counseling the patient regarding the associated adverse reproductive consequences. Practitioners should be vigilant about these potentials, aiming for timely corrections.
Footnotes
Acknowledgement
The authors acknowledge the work of Mr. Niranjan Kulkarni (biostatistician) and thank him for the statistical analysis of this research.
Author Disclosure Statement
There are no conflicts of interest by any of the authors. All authors are working in the Department of Obstetrics and Gynaecology, Pt. B.D. Sharma Post Graduate Institute of Medical Sciences.