
Abstract
Abstract
Objective:
The goal of this research was to evaluate fertility outcomes after laparoscopic tubal anastomosis for reversal of tubal sterilization, and assess this procedure's place as an alternative to assisted reproductive technology (ART).
Materials and Methods:
This retrospective cohort study was conducted between January 1, 2011 and mid-May 2017. Data were collected retrospectively from patients with tubal clips, who underwent laparoscopic tubal anastomosis performed by a specific surgeon during the study period, in a secondary Belgian medical unit.
Results:
Twenty-three patients underwent reversal surgery with a follow-up time ranging from 4 months to 6 years. The patients' ages were between 29 to 42 (average: 35.6 years; standard deviation [SD]: 3.2) at the time of the surgery. Average surgery duration was 104.2 minutes (SD: 26.4; range: 64–157 minutes). No intraoperative or postoperative complications were reported. A 61% spontaneous pregnancy rate was achieved (100% <30 years; 42.8% 30–34 years; 66.6% 35–39 years; and 66.6% ≥ 40 years). Average time to conceive was 171 days (SD: 194.5; range: 10–743 days). Of the patients who became pregnant after the surgery, 42.8% reported 2 or more pregnancies. Also reported were: 11/25 live births (44%); 7/25 early miscarriages (28%); 1/25 ectopic pregnancies (4%); 3/25 abortions (12%); and 3 ongoing pregnancies (12%).
Conclusions:
Bilateral tubotubal anastomosis is effective for women wanting to restore their fertility after tubal sterilization and should be proposed as an alternative to ART. Randomized controlled trials comparing in vitro fertilization with tubotubal anastomosis are needed in order to lead to a conclusion. (J GYNECOL SURG 34:115)
Introduction
A
After tubal sterilization, two options are available for a renewed wish for children: (1) assisted reproductive technology (ART) or (2) reversal surgery by tubotubal anastomosis. The choice must be customized and made in consultation with the couple based on a benefit–risk approach. The generous Belgian national health system provides access to both options for Belgian citizens.
Reversal of tubal sterilization has been performed since the 1970s. 4 It was initially done by laparotomy and has been replaced by the minilaparotomy approach. Today—thanks to equipment improvement, technique evolution, and improved surgical skills—laparoscopic reanastomosis has emerged. This technique results in comparable pregnancy rates, less postoperative pain and complications, and as faster recovery. However, it requires longer surgery, and there is a slower learning curve for the surgeon. 5 More recently, robotic techniques have proven to be effective, with a nevertheless higher cost as well as prolonged surgical and anesthesia times.6,7
Materials and Methods
This clinical study was conducted to analyze data retrospectively on all patients requesting sterilization reversal who benefited from a laparoscopic tubal anastomosis performed by 1 specific surgeon at the Centre Hospitalier de Wallonie Picarde in Tournai, Hainaut, Belgium, between January 1, 2011, and mid-May 2017. The Centre Hospitalier de Wallonie Picarde is a secondary teaching hospital in southwestern Belgium.
Patient enrollment
Twenty-five patients who underwent tubal anastomosis in order to conceive after tubal sterilization with clips were enrolled in the study. The installation of tubal clips had been performed in either this center or another center. All of the patients were asked to undergo a fertility work-up before surgery including day 3 follicle-stimulating hormone–Luteinizing hormone–estradiol levels and an endovaginal ultrasound scan to ensure the absence of uterine pathology. Preoperative hysterosalpingography (HSG) was performed in all but 3 patients to rule out intrauterine disease and to confirm tubal patency up to the tubal clips. Semen analysis was requested from each patient's partner when no child was conceived with the patient or if latest pregnancy was more than 2 years prior to the study in order to exclude azoospermia.
Surgical technique
The surgical technique has been the same since 2011. The intervention is performed through a laparoscopic approach under general anesthesia. The patient is set in a lithotomy position. After surgical disinfection and implementation of surgical fields, the bladder is emptied using a urine probe.
First, a uterine manipulator is placed. Then, the standard gynecologic laparoscopy is implanted. After a 10-mm subumbilical incision and adequate pneumoperitoneum is achieved with CO2 gas, a 10-mm trocar is introduced. A 0° laparoscope is inserted and diagnostic laparoscopy is performed to evaluate the patient's internal gynecologic status and rule out any hydrosalpinx or frozen pelvis. Indeed, this drastically improves the risk of extrauterine pregnancy and the in vitro fertilization (IVF) option should then be considered. 8
If the internal status is favorable, three 5-mm trocars are inserted: two lateral to the deep inferior epigastric vessels and one 2 cm above the pubis, on the median line. Standard 5-mm instruments are used to perform the entire surgery.
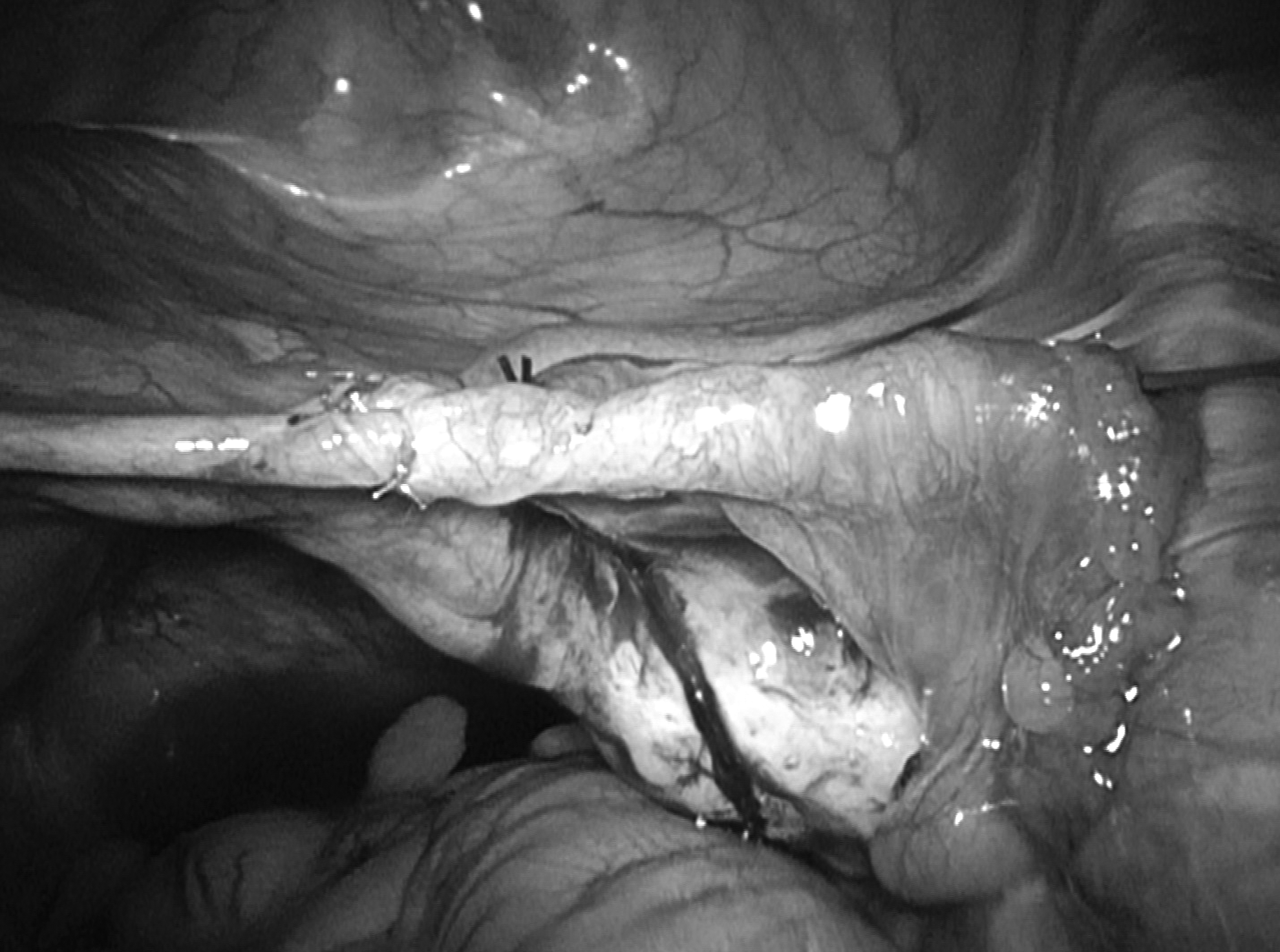
The tubotubal anastomosis consists of the following steps (Fig. 1–8):
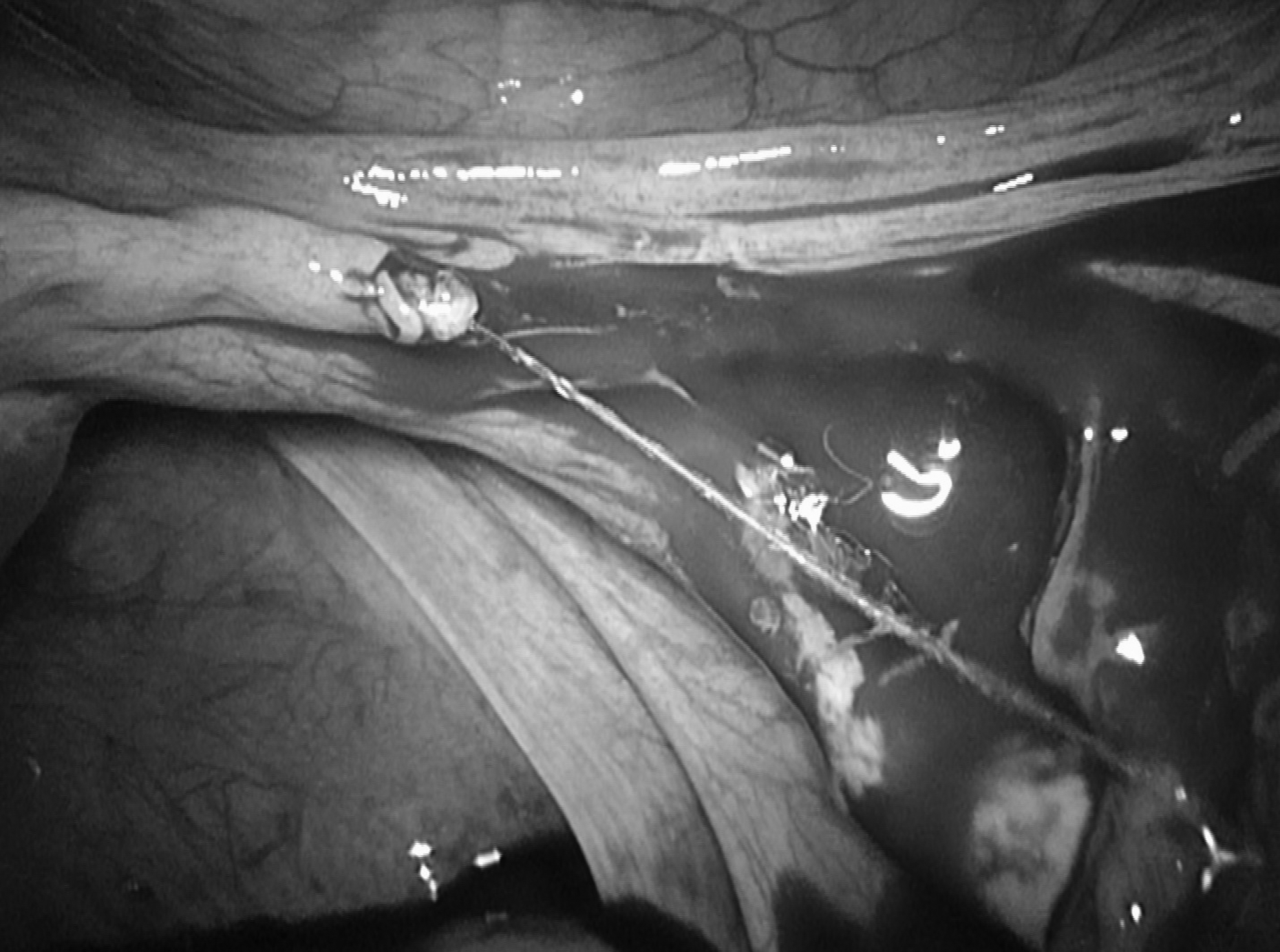
(1) The occluded tubal segment, including the clips, is excised. (2) The proximal tubal patency is verified through intrauterine injection of physiologic methylene blue–tinted serum, excluding an isthmic obstruction of the tube. (3) Then, a retention suture (Vicryl® 2/0) is placed in the mesosalpinx to align the tubal lumen and to avoid an excessive tension on the future tubal stitches. (4) During the third step, a hysteroscopy is performed with a Bettocchi hysteroscope. (5) Through the hysteroscope, a tubal splint (TERUMO® Guide Wire 0.035") is inserted through the cervical canal to the tubal ostium. (6) The splint is taken laparoscopically and inserted into the distal portion of the tube. (7) Then, atraumatic progression of the splint is performed until it is exteriorized beyond the tubal pavilion in the abdominal cavity. The main advantages of this step are to establish good positions of both tubal lumens, to stabilize the tubes during the anastomosis, and to ensure complete tubal patency. (8) A single layer end-to-end tubotubal anastomosis is performed; 4 interrupted sutures of PROLENE* 5/0 are made at the 4 cardinal points incorporating the serosa and muscularis, taking care not to penetrate the endothelial layer.
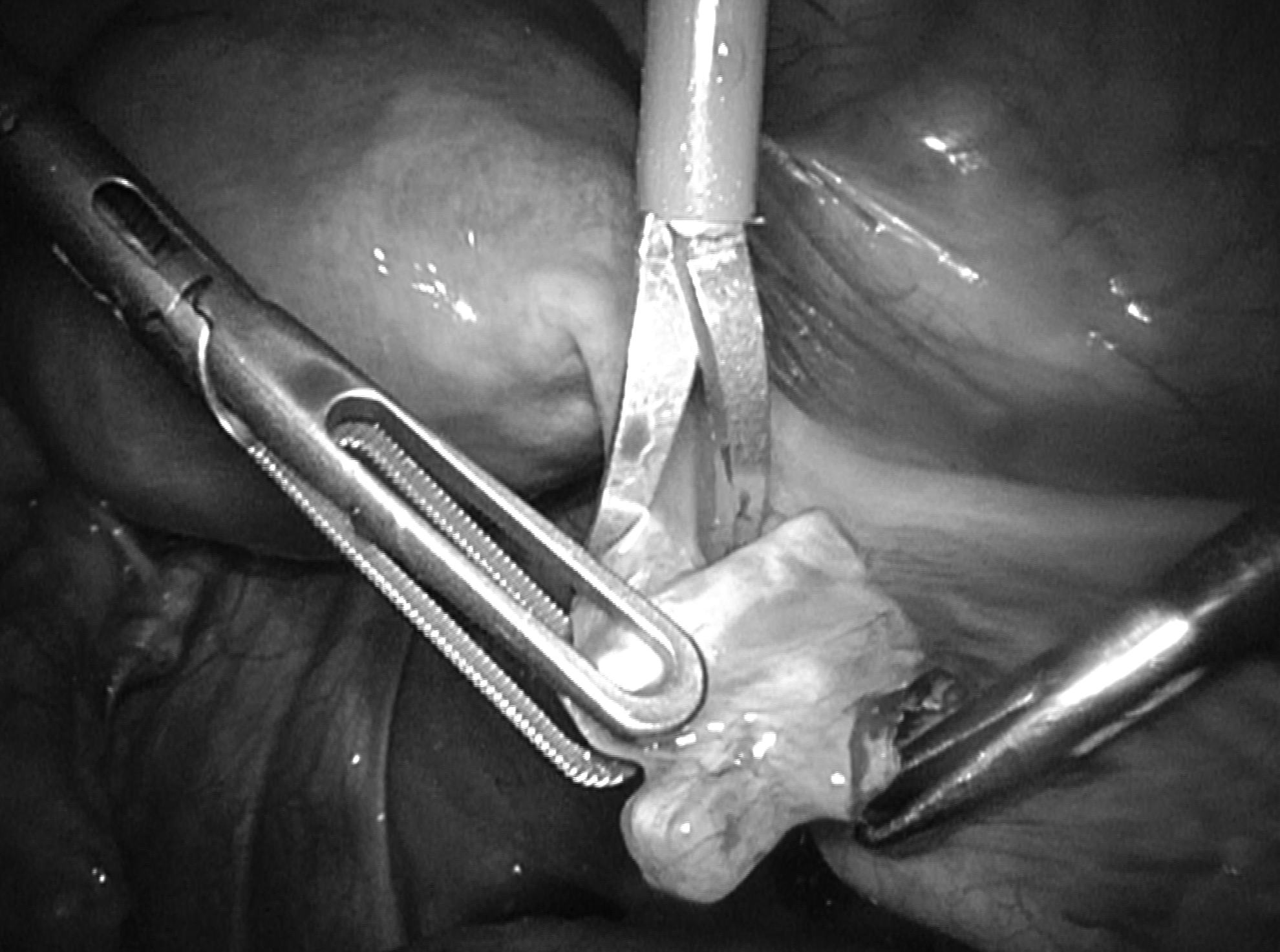
Excision of the tubal segment, including the clips.
Methylene blue test confirms the proximal tubal patency.

Reconciliation point of Vicryl® 2/0 on the mesosalpinx.
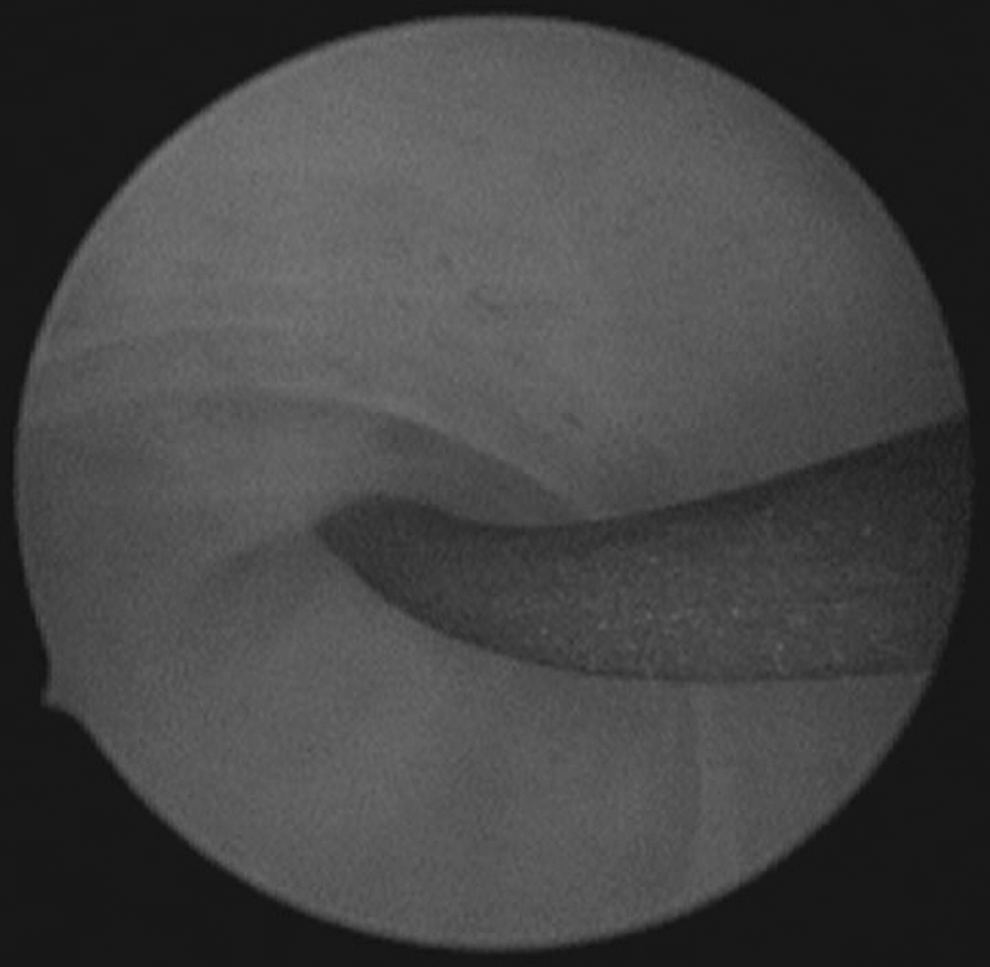
Diagnostic hysteroscopy and insertion of tubal splint through tubal ostium.

Intra-abdominal recuperation of the splint.
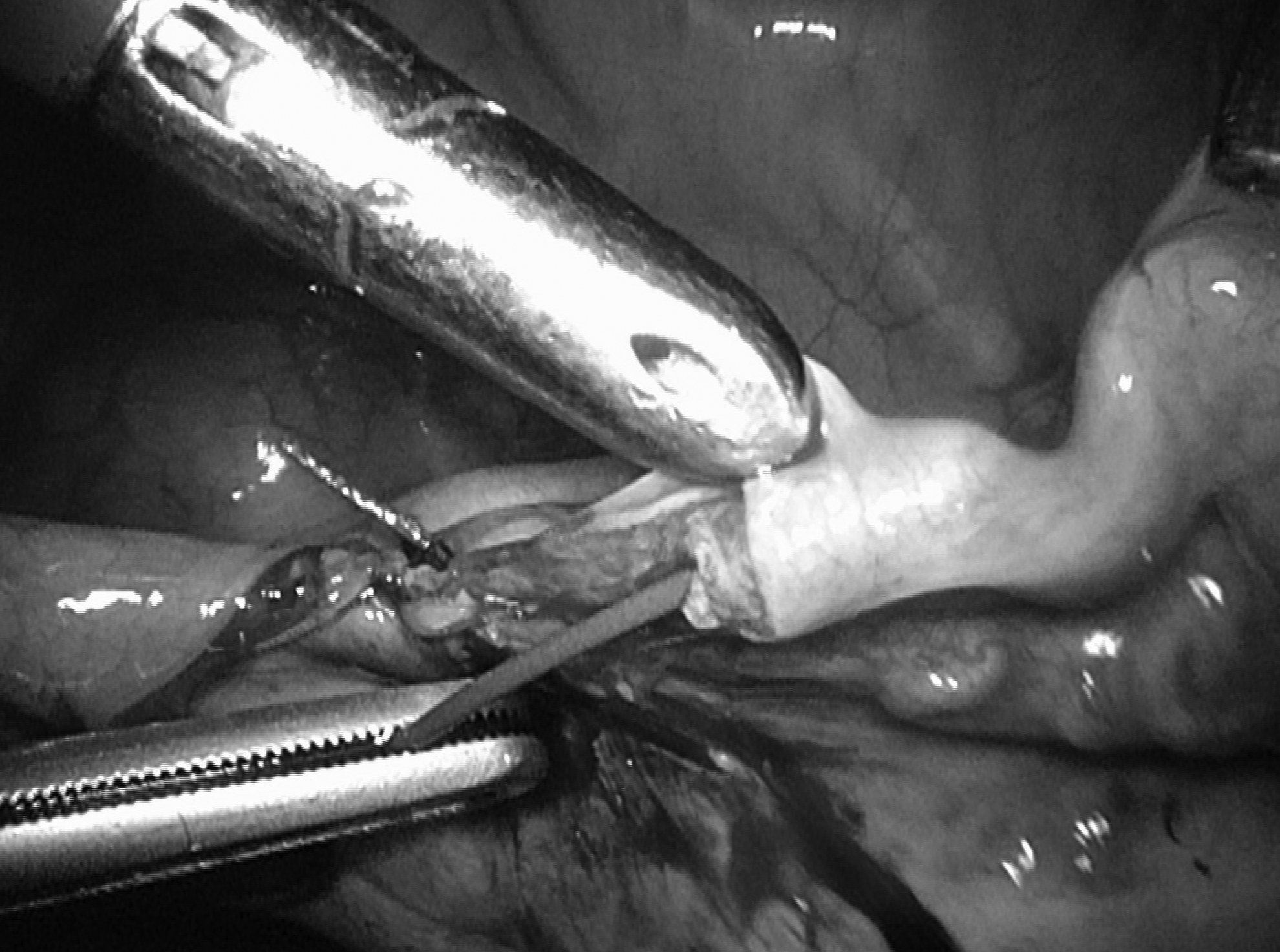
Passage of the splint in the distal tubal portion.

Atraumatic progression of the guide until its exteriorization beyond the tubal pavilion.
Tubal suture with 4 cardinal stitches of PROLENE* 5/0.
Both splints are left in place and fixed with tape on the thighs of the patient until 2 days after surgery to enable the early healing phases with a proper alignment of the tubal segments. The splints are then removed by smooth traction. Antibiotic therapy, consisting of Zinacef® (1.5 g 3/day) and Flagyl® (1.5 g/day), is given until the removal of the splints to avoid any infection that could be caused by the vaginal insertion of a foreign body into the abdominal cavity.
Data collection
For every patient, data were collected concerning age at the time of sterilization and reversal surgery, obstetric history, fertility workup, and semen analysis of the partner. Surgery and hospitalization duration, previous reanastomosis on one or both sides (with or without use of splints), and intra- and postoperative complications were compiled.
The medical charts were screened for information regarding the follow-up. Previous pregnancies or their absence were registered as well as time to conception; whether pregnancy had resulted in live birth, miscarriage (positive pregnancy test but ending <12 weeks gestational age), or ectopic pregnancy; and delivery date. If there were ongoing pregnancies, they were noted as well as events that possibly interfered with the pregnancy success rate, such as contraception, change of mind regarding desire for a child, hysterectomy, or ending relationship with the partner.
Furthermore, if HSG was performed postoperatively, it was reported with its result.
Results
The study population
A total of 25 patients were included. Unfortunately, 2 patients could not be contacted for follow-up. This left 23 patients with a follow-up time ranging between 4 months and 6 years. Average patient age at the implementation of tubal clips was 30.13 years (standard deviation [SD]: 4.2; range: 18–37 years). All of the patients had undergone tubal sterilization by laparoscopic placement of either Hulka or Filshie clips. At the time of the reconstructive surgery, the patients' ages ranged between 29 and 42 with an average of 35.6 (SD: 3.2). The distribution by age was: less than 30 (4.3%); between 30 and 34 (30.4%); between 35 and 39 (52.2%); and 40 and older (13.1%). The average number of offspring at the time of the surgery was 2.48 (SD: 1; range: 1–4).
Surgical implications
Internal laparoscopic and hysteroscopic status was normal in all patients. The tubotubal anastomosis was bilateral in all patients.
Average surgery duration was 104.2 minutes (SD: 26.4; range: 64–157 minutes). No intraoperative or postoperative complications were noticed. The duration of hospitalization lasted an average of 1.8 days (SD: 0.4).
For 18 of the 23 patients, it was possible to insert the tubal splint bilaterally through the tubal ostium up to the abdominal cavity. Unilateral complete tubal splint passage with a contralateral atraumatic progression through the anastomosis site but blockage in the distal part of the tube was noted in 3 of the 23 patients. In the 2 remaining patients, bilateral splint progression up to the abdominal cavity failed, but at least a unilateral tubal suture around the splint was achieved.
Pregnancy incidence
Pregnancy was defined as a positive blood test indicating pregnancy.
In total, of the 23 patients, 14 patients became spontaneously pregnant during the follow-up period. The current authors were able to conclude that their success rate of spontaneous pregnancy was 61%. The age distribution of the success rate is as follows: less than 30 (100%); 30–34 (42.8%); 35–39 (66.6%); and 40 and older (66.6%).
The average time to conceive was 171 days (SD: 194.5; range: 10–743 days). Therefore, the delay between the surgery and the conception was ∼5.5 months.
Among the 9 patients who did not get pregnant spontaneously, 5 patients agreed to have an HSG. A tubal obstruction was found unilaterally in 1 of 5 patients and bilaterally in 4 of 5 patients. IVF was proposed to those who showed no tubal patency on the postoperative HSG. The other 4 patients did not follow the HSG as prescribed.
Regarding the factors that interfered with the pregnancy rate, 1 patient changed her mind about her wish to have a child and started a contraceptive pill after her surgery. A second patient gave up her desire to conceive for 2 years after her surgery and then wished to conceive but had reached the age of 44. A third patient took a contraceptive pill during the 1 year following her reversal surgery and was pregnant as of this writing.
Excluding both patients that used contraceptive methods following surgery, the spontaneous pregnancy rate can be estimated at 66.6% (14/21).
Pregnancy outcomes
The 14 patients who became pregnant during the follow-up period reported a total of 25 pregnancies. Among the patients who became pregnant after the surgery, 42.8% reported 2 or more pregnancies.
In total, 11/25 live births (44%), 7/25 early miscarriages (28%), 1/25 ectopic pregnancies (4%), 3/25 abortions (12%), and 3 ongoing pregnancies (12%) were reported.
No obstetrical complications were noted during the pregnancies.
Birth rates
Of the patients who became pregnant, 57% had at least 1 live birth during the follow-up period. The first pregnancy of 3 of the patients was still ongoing as of this writing.
All of the patients had prior vaginal deliveries and delivered vaginally after their tubotubal anastomosis surgeries.
Discussion
Sedbon's team performed the first laparoscopic tubal reanastomosis in 1989. 9 Since then, various suture techniques have been developed,10,11 using microclips 12 ; an intraluminal guide 13 ; the one, two-, or three-stitch technique14,15; tissue adhesive or glue 9 ; etc. No laparoscopic technique has been described for reversal of tubal sterilization.
A systematic review (37 studies, 10689 women) published by Van Seeters et al. in 2017 concluded that surgical approach (minilaparotomy, laparoscopy, or robotic) had no influence on pregnancy rates and outcomes. 16 There is currently no sufficient evidence showing superiority of one specific approach for reversal surgery.12,17
Laparoscopy offers a shorter hospitalization time (1.8 days in the current study). 11 The operating time ranges from 95 to 284 minutes.11,13,18 The average of 104.2 minutes in the current study was shorter because the surgeons were more experienced in performing laparoscopy.
The review of Deffieux et al. in 201111 reported a time to conception after laparoscopy or laparotomy between 2 and 9.6 months, which was comparable to the current study (∼ 5.7 months).
As in the current analysis, most studies reported no intra- or postoperative complications.15,18 Deffieux et al. 11 noted a 5% conversion rate to laparotomy and 1 case of thromboembolism 10 as well as 1 case of epigastric artery injury.
With respect to pregnancy rate, a recent systematic review found a 42%–69% rate after reversal surgery through different approaches. 16 Tubal anastomosis was first performed by laparotomy, then by minilaparotomy, with a pregnancy success rate of 60%–91%.19,20 More recently, in 2016, Berger et al. found a similar 69% pregnancy rate and a 35% birth rate. Their clip sterilization subgroup had the best pregnancy (76%) and birth (50%) rates, compared to ligation and coagulation procedures. 21
Later, laparoscopy was developed with the same microsurgical technique used in laparotomy. Different studies yielded high pregnancy rates of up to 84.9%. 10
The technique was simplified and showed similar results. Placing one stitch on the antimesial edge of the tube led to an intrauterine pregnancy rate of 53.2% (Dubuison and Chapron, in 1998) 14 and 72.7% (Bissonnette et al., in 1999). 15 Wiegerinck et al. (in 2005) 12 and Schepens et al. (in 2011) 18 reported, respectively, 55% and 74% cumulative pregnancy rates with their sutureless laparoscopic reanastomosis technique. Ribeiro et al. (in 2007) found a pregnancy rate of 56.6% with a 4-stitch technique similar to the current authors' technique. 13 In the current patient cohort, the pregnancy rate reached 61%.
The current study population was too small to analyze the factors that influenced the success rate. The only unanimous influencing factor was age.3,11,16,19,22 The length of the available tubal segments, the type of ligature, and the quality of the microsurgical technique are controversial.3,10,11,22,23
Most studies reported a gradual decline of pregnancy and birth rates with age and, definitely, a drop after ages 37–40.10,21,24–26 Some researchers went as far as to assert that after age 37 IVF should be preferred. 27 The current narrowly studied cohort had good results in this age range (66.6%). The pregnancy rate at an age older than 40 should not be neglected nor constitute an exclusion factor for reversal surgery. If ovarian function is preserved, tubotubal anastomosis could be proposed as suggested by Petrucco et al. (2007), who found a 40% live birth rate in patients older than age 40. 28 However, the higher miscarriage occurrence should not be overlooked at this age. 29
The incidence of extrauterine pregnancy is: 2% in the general population 8 ; 3%–8% after reversal surgery3,10,16; and 2%–11% following IVF in tubal infertility. 8 The current study showed similar results (4%) explained by the precision of the surgery and healthy tubal mucosa resulting in anatomically and physiologically normal tubes.
IVF started in the 1980s with poor results that improved quickly to reach a plateau of around 27%–30% live births per initiated cycle in the United States and 21% in Europe due to embryo-transfer legislation. 30
In a study published by Boeckxstaens et al., the cumulative pregnancy rate reached a nonstatistical significant difference of 52% in an IVF group and 59.5% in a surgical tubotubal anastomosis group by laparotomy. 27 As with tubal anastomosis, pregnancy and live birth rates with IVF decline with age. 25
Tubotubal anastomosis can be considered as a curative surgery, offering a monthly natural chance of conception and the possibility to conceive more than once. Frequent injections and monitoring as well as ovarian hyperstimulation risk are avoided. Some researchers have cited poorer obstetrical outcomes (perinatal mortality, preterm births, low birth weights, congenital malformations, and cesarean deliveries) for IVF singletons compared to spontaneous conception.31–33 IVF also increases the risk of multiple pregnancies.
However, IVF offers the advantage of avoiding surgery, a high success rate per cycle, and a short time to conception.29,34
Despite the generous Belgian national health system, the cost issue is important. The total cost calculated by De Sutter et al. (2002) 35 reached 2,426€ ($2,875) per IVF cycle, compared to the one-time cost of 2,360€ ($2,800) for reversal surgery. In total, the cost per delivery for IVF (11,707€) [$13,890] is twice that of reversal surgery (6,015€) [$7130] 27 not even including the additional costs. 25
In 2012, an American Society of Reproductive Medicine Committee Opinion concluded that, for all age ranges, reversal surgery was more cost-effective than IVF. This is partially due to the higher cumulative pregnancy rate of tubotubal anastomosis, even if the pregnancy rate per cycle is higher with IVF.34,36
A Cochrane systematic review failed to assess whether IVF or tubal anastomosis was superior due to a lack of randomized controlled trials (RCTs). 4
Limitations
The current study was retrospective research, implying inherent limitations. The narrow sample size made statistical analysis less powerful. Finally, the surgeries were spread over 6 years with 9/23 patients who had surgery in the last year. The follow-up period was short, and further pregnancies might be reported later. Indeed, literature shows that the cumulative pregnancy rate increases with time, mostly during the 2 years following surgery.10,23,37
Conclusions
Bilateral tubotubal anastomosis is effective for women wanting to restore their fertility after tubal sterilization. Even if performed on a small cohort and in a secondary-care center, this surgery produced good results. This proves that it should be considered as an alternative to ART, given that the pregnancy and birth rates are encouraging and that the cost and burden of ART can be avoided. From the current authors' perspective, besides severe andrologic factors, tubal reversal should be encouraged prior to IVF for woman desiring pregnancy following tubal sterilization. RCTs comparing IVF with tubotubal anastomosis are needed to lead to a conclusion.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.