
Abstract
Abstract
Objective:
The goal of this research was to evaluate no concomitant hysterectomy versus concomitant hysterectomy at the time of pelvic organ prolapse (POP) repair.
Materials and Methods:
This was an observational cohort study involving inpatient and ambulatory surgery settings in New York State. Women younger than 55 without prior hysterectomies who underwent POP repair between 2009 and 2014 were included. POP repairs included apical support in efforts to equate grade of prolapse. Determinations were made regarding 90-day safety events and reintervention, urinary retention, and pelvic pain within 1 year and 3 years following the initial procedure.
Results:
There were 1564 (71.3%) patients who underwent concurrent hysterectomy at the time of POP surgery, while 629 (28.7%) did not undergo hysterectomy. No differences were found in reinterventions and pelvic pain within 1 year or 3 years after POP repair. Over the study period, we observed increased utilization of concurrent hysterectomy of 46.4% in the most recent study year (p = 0.02). After propensity score matching, patients in the concurrent hysterectomy group had more surgical complications and had more expensive charges.
Conclusions:
Concurrent hysterectomy was more expensive and had more surgical complications within 90 days of the initial procedure, compared to not undergoing hysterectomy. Long-term outcomes were not compromised and did not lead to earlier reintervention when a patient did not undergo hysterectomy. (J GYNECOL SURG 34:122)
Introduction
H
Concomitant hysterectomy is performed at the time of POP surgery because it is thought that, by preserving the uterus, this might increase the risk of POP recurrence. This procedure could help decrease the ability to suspend the vaginal apex adequately. 3 However, uterine-preserving surgery is less invasive, and techniques for preservation have been improving in the past decade.4,5 A number of small studies have reported reduced blood loss, shorter operating time, faster postoperative recovery, and overall fewer complications associated with uterine preservation.6–8 The evidence is inconclusive regarding the benefits and harms of both approaches,4,6,8–11 and there is an equipoise for a randomized clinical trial.6,10
This research was conducted to determine if hysterectomy led to better short- and intermediate-term outcomes, fewer complications, and longer freedom from reintervention at the time of POP surgery. Mesh-based repairs were intentionally excluded due to their unique set of complications and higher reintervention rates due to pelvic pain that are not experienced with native tissue repairs.10,12 This study used 20-year population data from the state of New York, including all women undergoing POP repair, to address this question.
Materials and Methods
Data source
This study utilized the New York Statewide Planning and Research Cooperation System (SPARCS), which is a database that collects patient-level details from every hospital discharge; ambulatory surgery; outpatient service visits to hospital extension clinics; and diagnostic and treatment centers, and emergency departments in New York State. 13
Study population
Patients undergoing surgeries for POP (International Classification of Diseases [ICD]–9-CM 618.0–618.9) conducted between 2009 and 2014 were identified. All procedures were identified using ICD-9-CM procedure codes 14 and Current Procedural Terminology–4th Edition codes 15 (Appendix Table 1 and Appendix Table 2). Each patient's past surgical history was available from the date of inception of the database through the use of these procedure codes. Patients undergoing prolapse repair through an abdominal approach were excluded as well as those who underwent mesh-based repair due to its higher complication and reintervention rates. 16 Only women under age 55 at the time of the procedure were included, and any women with prior hysterectomies were removed for a comparative study.
The younger study population (< 55 years) was chosen to ensure that patients were less likely to have had hysterectomy before 1995 (before age 40 for the cutoff age of 55 years). 17 The literature reports the proportion of women ≤35 years of age having hysterectomy is <5%. 18 This strategy was adopted to eliminate the possible bias of including patients with unrecorded prior hysterectomies in the comparative study. The year 1995 is the first year when SPARCS data were available to the current authors and was the start year for identifying patients' medical histories.
Patients with histories of prolapse repair surgeries or sling procedures before their identified surgery dates were also excluded. Patients with diagnoses of fibroids, abnormal bleeding, cancer, or cervical dysplasias were also excluded as well as patients receiving concurrent sling procedures at admission for POP. Those receiving concurrent slings were excluded due to possible confounders associated with this procedure and to isolate the effect of hysterectomy on POP outcomes.
Variable definition and study endpoint
Patient characteristics included age (< 35, 35–44, and 45–54), race (white, nonwhite, and unknown), insurance status (Medicare, Medicaid, commercial, and other), and comorbidities and surgery types, which were defined using procedure codes. Comorbidities were identified using algorithms validated by Elixhauser and colleagues. 19 Facility-related characteristics included service type (inpatient and outpatient services), facility ownership (state, nonstate/nonprofit, and private), facility academic status (teaching and nonteaching), and facility volume by tertiles (low, medium, and high) calculated based on average annual volume of POP procedures.
Outcomes included length of stay and charges at baseline hospitalization, safety events within 90 days, and reintervention, pelvic pain, and urinary retention within 1 year and 3 years following the initial procedure. Urinary retention was defined through CPT codes and Foley catheter placement. Pelvic pain was defined using diagnosis codes. Safety events within 90 days included medical complications (acute myocardial infarction [MI], stroke, pulmonary embolism [PE], perioperative shock, deep venous thrombosis, and respiratory complications), surgical complications (stricture or kinking of ureter, persistent postoperative fistula, postoperative infection, vesical fistula, urinary–genital tract fistula, digestive–genital-tract fistula, and bladder injury), bleeding, postoperative urinary-tract infections (UTIs), and urinary retention. Readmission within 90 days into an inpatient setting was also examined. Patients who underwent repeated prolapse, revision procedures, or sling procedures were determined as having reinterventions. Patients were considered censored if death was recorded in the SPARCS database during the follow-up period.
Statistical analysis
Baseline characteristics were compared between 2 patient groups. One group included patients undergoing concurrent hysterectomy at the time of POP surgery. The other group included only patients undergoing uterine-preserving POP surgery. Differences in baseline characteristics between the patient groups were examined, using percentage difference of event counts. Temporal trend of hysterectomy versus uterine-preserving was assessed using a Cochran–Armitage trend test. Propensity score matching was used to adjust for differences between the hysterectomy and uterine-preserving groups. Propensity scores for each individual were obtained from a multivariable logistics regression based on patient characteristics (age, race, and insurance status), procedure year, comorbidities, service type, facility academic status, facility ownership, procedure volume, and surgery type. Nearest-neighbor matching was performed at a 1:1 fixed ratio, using a caliper width of 0.2 of the standard deviation of the logit of the propensity score. The differences in baseline characteristics of the 2 groups before and after propensity score matching were then examined to assess reduction of heterogeneity. A difference of <10% was considered an adequate balance. Patients with missing information regarding facility characteristics were excluded from propensity score matching.
Similarly, outcome measures between patient groups were compared before and after propensity score matching. The difference was assessed using χ2 tests in the entire cohort and Mantel–Haenszel tests in the matched cohort. Relative risks were calculated accordingly. Length of stay was compared using a Wilcoxon rank-sum test in the original cohort and using a signed-rank test in the matched cohort. Nonparametric time-to-event analyses were conducted in both cohorts to compare differences in having reintervention, pelvic pain, and urinary retention at 1 year and at 3 years following initial procedures. A log-rank test was utilized in the entire cohort, while a Prentice–Wilcoxon test 20 was utilized in the matched cohort to assess the difference between the 2 patient groups. Kaplan–Meier curves were constructed to visualize freedom from reintervention within 1 year and 3 years. All analyses were performed using SAS v9.4 (SAS Institute Inc., Cary, NC).
Results
Utilization of hysterectomy and uterine-preserving surgeries
There were 5680 women under age 55 undergoing POP repair between 2009 and 2014 in New York State. Of these women, 2708 had hysterectomies at the time of POP repair, while 2972 did not undergo hysterectomies. An overall increase in the proportion of patients undergoing concurrent hysterectomies was observed from 44.2% to 46.4% in 2014 (p = 0.02; Fig. 1).
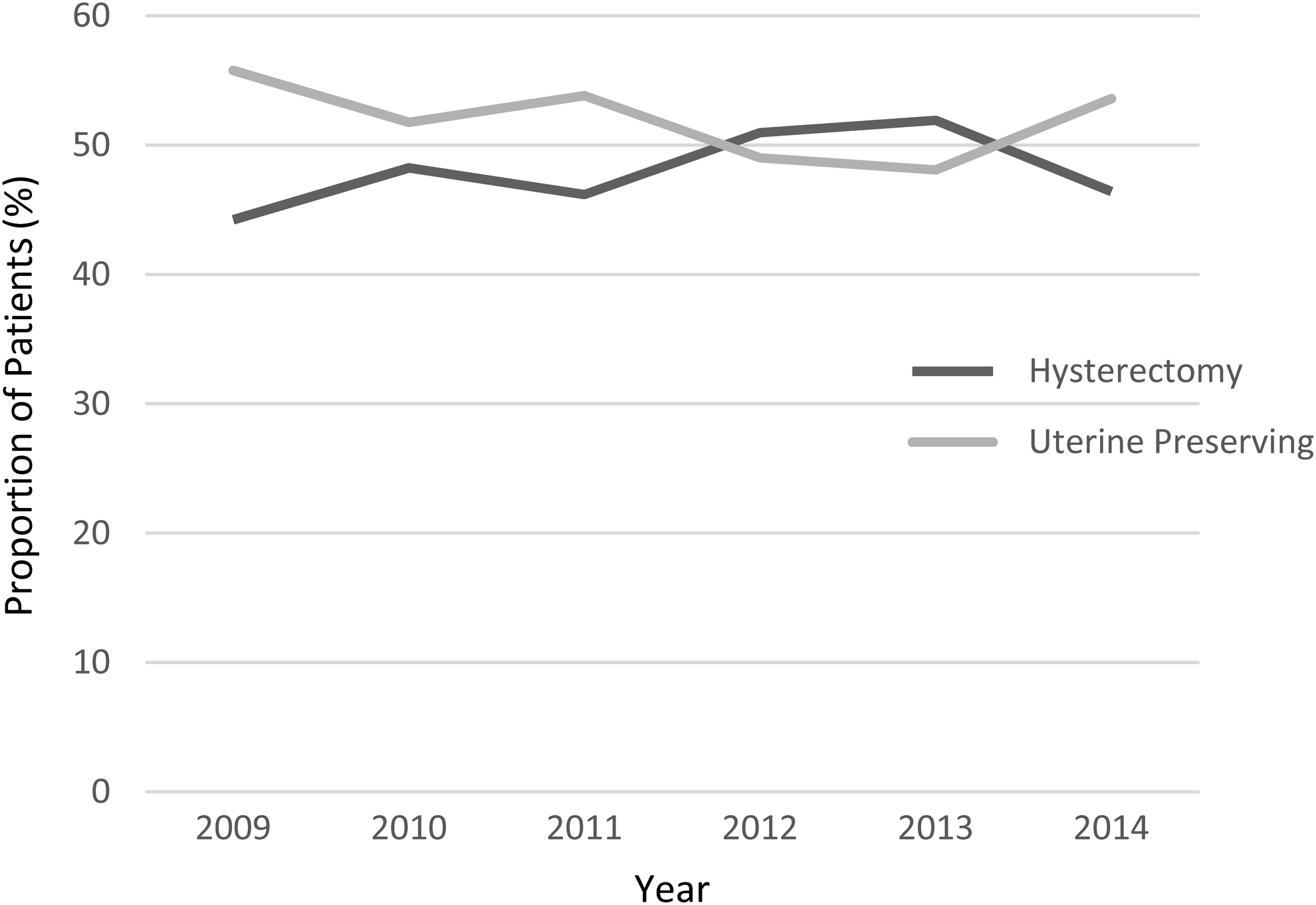
Trends of prolapse repair surgery with hysterectomy and uterine sparing surgery, between 2009–2014 in New York State (p = 0.02).
Patient characteristics
There were 2193 patients undergoing apical POP repair. Of these women, 1564 (73.1%) had hysterectomies, while 629 (28.7%) did not undergo hysterectomies. The majority were between 45- and 54-years-old (57.1%; n = 1253); Table 1). Fewer patients were younger than age 35 in the hysterectomy group than in the uterine-preserving group (hysterectomy versus no concomitant hysterectomy; 6.6% versus 13.2%). There was a slightly higher prevalence of hypertension (17.4% versus 12.1%), obesity (7.8% versus 5.1%), anemia (4.8% versus 2.4%), and depression (9.1% versus 7.2%) among patients who underwent hysterectomies than patients without concomitant hysterectomies.
POP, pelvic organ prolapse; NR, not reported.
Baseline outcomes and 90-days' safety
In unadjusted analyses, patients who received concurrent hysterectomies at the time of POP surgery had longer lengths of stay (RR 95% confidence interval [CI] of staying longer than 2 days: 1.60 [1.17–2.19]) and were relatively more likely to have medical complications (risk ratio [RR] 95% CI: 4.07 [0.96–17.31]; Table 2). The charges were also higher ($16,597 versus $12,444), compared to patients who did not undergo concomitant hysterectomies. After propensity score matching, concurrent hysterectomy with POP repair was consistently associated with higher charges (median charges were $15,013 versus $13,251 following POP repair surgery. No significant difference was found for length of hospitalization, medical and surgical complications, and inpatient readmissions within 90 days between the 2 cohorts, and there was a trend toward higher surgical complications in the hysterectomy group (Fig. 2).
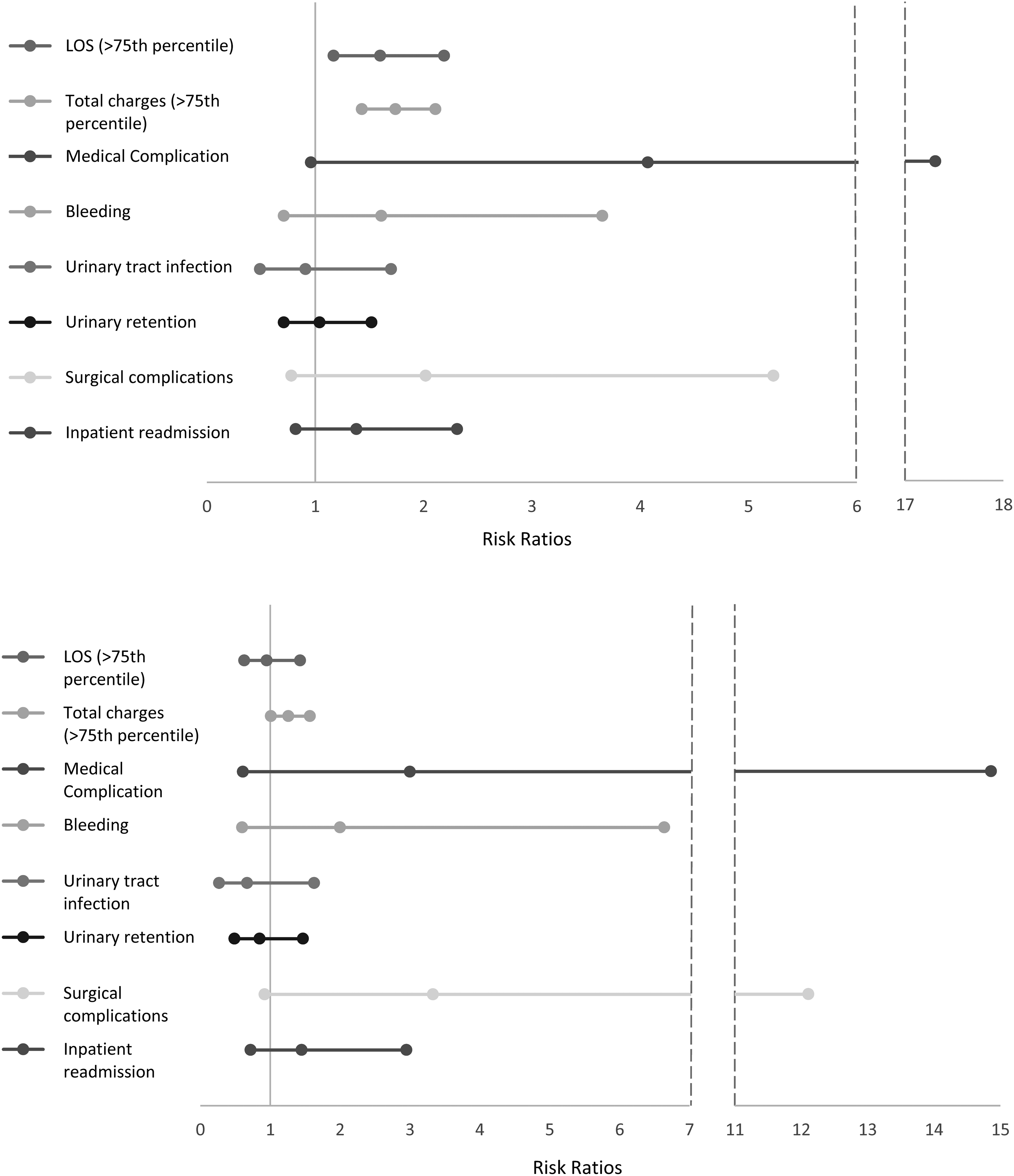
Risk ratios of index outcomes and 90-day safety events comparing patients undergoing pelvic organ prolapse surgery with hysterectomy to patients undergoing POP with uterine-preserving surgery. Top: Before propensity score matching (unadjusted risk ratio). Bottom: After propensity score matching (adjusted risk ratio).
p-Values calculated from χ2 test.
Risk ratios and p-values calculated using a stratified Mantel–Haenszel test.
p-Value was obtained from Wilcoxon rank-sum test in the original cohort and signed rank-test from the matched cohort.
90-day safety only included patients with complete follow-up time.
Medical complications included acute myocardial infarction, stroke, pulmonary embolism, postoperative shock, deep venous thrombosis and respiratory complications.
Surgical complications included stricture or kinking of ureter, persistent postoperative fistula, postoperative infection, vesical fistula, urinary–genital tract fistula, digestive–genital tract fistula, and bladder injury.
RR, risk ratio; IQR, interquartile range.
Longer term follow-up
Among patients who underwent POP repair surgery with and without hysterectomies, 69 and 29 of them had reinterventions within 3 years following initial surgeries, respectively. After propensity score matching, risks of reintervention 1 year (1.4% versus 2.3%) and 3 years (3.1% versus 5.2%) following surgery were slightly higher for patients who did not undergo concomitant hysterectomy than for patients in the hysterectomy group, but the differences were not significant (Fig. 3; Table 3). There were 118 and 46 patients in the hysterectomy group and uterine-preserving group, respectively, experiencing urinary retention within the 3-year follow-up period, without a significant difference between groups after propensity score matching (7.2% versus 7.2%; p = 0.97). Risk of having a pelvic pain diagnosis within 3 years was not different after propensity score matching between the 2 groups (3.9% versus 4.5%; p = 0.63).
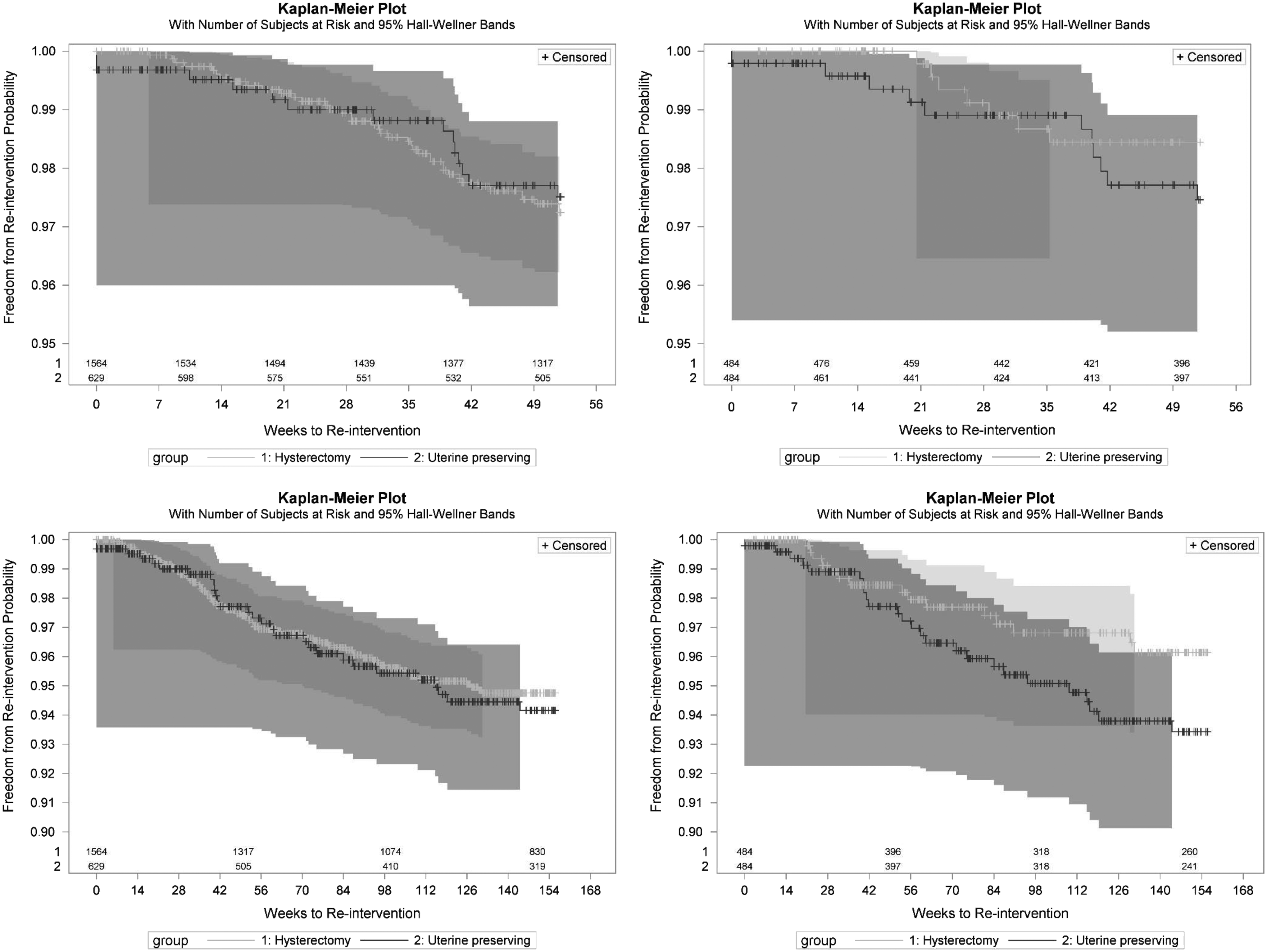
Time to reintervention following pelvic organ prolapse surgery between 2009 and 2014 in New York State. Kaplan–Meier plots show numbers of patients at risk and 95% Hall–Weller bands. Top left: One-year follow-up before propensity score matching. Top right: One-year follow-up after propensity score matching. Bottom left: Three-year follow-up before propensity score matching. Bottom right: Three-year follow-up after propensity score matching.
p-Value was obtained from log-rank test comparing difference in survival function between the 2 patient groups.
p-Value was obtained from Prentice–Wilcoxon test comparing difference in survival function between the 2 patient groups.
POP, pelvic organ prolapse; NR, not reported.
Discussion
It was found that there was no additional benefit in terms of future surgery for prolapse in women who underwent concurrent hysterectomies, compared to women who did not undergo concomitant hysterectomies. Uterine-preserving surgery—which addresses apical prolapse—has been shown to have similar outcomes to the outcomes of patients undergoing concurrent hysterectomies. In a study by Dietz et al., women were randomized to either undergo vaginal hysterectomy or sacropinous hysteropexy (uterine preserving). 10 Women who underwent hysteropexy took less time to return to work (43 days versus 66 days; p = 0.02). 10 Although at a 1-year follow-up, those who underwent hysteropexy had a 17% risk of recurrent prolapse (95% CI: 2–30), there were no statistical differences in functional outcomes or quality of life. 10 A caveat of that study was it did not measure reintervention rates.
It is possible that the improvement in surgical techniques of uterine-preservation in recent years has contributed to the nondifferential long-term risk following both surgeries. To date, there are solitary randomized controlled trials7,10,21–23 addressing the effectiveness of concurrent hysterectomy at the time of POP surgery. In a multicenter, randomized nonblinded trial, Detollenaere et al. evaluated whether uterine-preserving vaginal sacrospinous hysteropexy was noninferior to vaginal hysterectomy with suspension of the uterosacral ligament among 208 women undergoing treatment for POP. 22 The intraoperative period showed that mean operating time (in minutes) and estimated blood loss (mL) were higher in patients receiving vaginal hysterectomies. In the postoperative period, mean length of stay was similar in both groups (n = 3 days).
Patients who did not undergo concomitant hysterectomies at the time of POP surgery had similar risks for complications, including major medical events (MI, PE, stroke, shock), postoperative bleeding, UTIs, and bladder injuries. It was found that patients undergoing concomitant hysterectomies at the time of POP surgery had a trend toward more surgical complications. There was also no significant difference in long-term outcomes following POP repair, including urinary retention and pelvic pain. In a previous study evaluating hysterectomy at the time of POP surgery, this group had significantly higher complication rates (31.2% versus 11.5%) with concurrent hysterectomy. 8 Furthermore, women having concurrent hysterectomies experienced significantly higher blood loss, with 4.2% of the patients undergoing blood transfusions. 8 However, these results are not directly relatable to the current study given the difference in ages of the patients studied.
In the current study, there were higher costs with concurrent hysterectomies. This was also confirmed by Costantini et al. who found higher mean hospital stay associated with hysterectomy, compared to uterine-preserving surgery. 24 The evidence of increased readmission into an inpatient service within 90 days following hysterectomy also suggests that overall use of resources is higher after hysterectomy. Based on this information, when uterine-sparing surgery was noninferior to concomitant hysterectomy, the estimated cost savings per surgery was $1,203, without taking into account readmission costs.
Another finding in the current study was an increase in the use of hysterectomy for POP. This is surprising, given that several studies have shown that women prefer a uterine-preservation approach. In a cross-sectional study of 213 women with POP, 25 when treatment was similar in outcome, 36% preferred uterine-preservation, 20% preferred hysterectomy, and 44% had no preference. When uterine-preservation was superior, 46% preferred this method, compared to 11% for hysterectomy. Uterine-preservation still remained high at 21%, even when hysterectomy was seen as a superior option. 25
There were some limitations in the current study. The SPARC data do not capture the severity of POP, although only patients who had apical prolapse were included to help reduce bias in the groups. Statistical methods were also applied to minimize residual confounding and to reduce imbalance between groups. Potential unmeasured confounders, such as physicians' and patients' preferences, could have been limitations of the observational study design. Although menopause would be a risk factor for POP, these data were not available, although the 2 cohorts were matched for age and comorbidities. In addition, miscoding and undercoding might have occurred, and follow-up of patients might also have been incomplete in the state database.
Furthermore, women might have had hysterectomy previously, biasing the current study. Also, the younger group of patients evaluated might have had better general conditions and were less likely to be subject to adverse postoperative outcomes. Despite this, the current study fills a major gap in evidence by using New York State all-inclusive data (population 27 million) from recent years.
To ensure that the data were robust, only patients who underwent POP surgery for the first time between 2009 and 2014 were identified, and patients who had prior hysterectomies or previous POP surgeries were excluded to 1995. Although patients who underwent hysterectomies before the study period (1995) could not be eliminated, the oldest person in this study would have been younger than age 40; and, thus, hysterectomies were less likely to be missed. 17 The cohort was matched to controls to adjust for confounding variables, which additionally strengthened the comparisons made between the groups. Reintervention was used as a main endpoint of the analyses, and this was in line with a patient-centered approach. The current authors believe that what is important is the incidence of undergoing surgery again. The inclusion of data from the entirety of New York State from recent years makes this study unique, robust, and also very applicable nationally.
Conclusions
This is the first major population cohort study addressing the comparative effectiveness of hysterectomy versus no concomitant hysterectomy at the time of POP surgery. Longer-term outcomes—specifically freedom from reintervention—were not compromised when preserving the uterus. Prospective randomized trials are needed to evaluate the role of hysterectomy at the time of POP repair.
Footnotes
Acknowledgment
The authors thank Ms. Wei-Chun Hsu for her contribution in statistical analysis.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
| ICD-9 Diagnosis/Procedure Code | CPT-4 Code | ||
|---|---|---|---|
|
|
|||
|
|
|||
| Acute myocardial infarction | 410.x | ||
| Intermediate coronary syndrome | 411.1 | ||
| Acute coronary occlusion without myocardial infarction | 411.81 | ||
| Other acute & subacute forms of ischemic heart disease, other | 411.89 | ||
| Cardiac complications, not classified elsewhere | 997.1 | ||
|
|
|||
| Iatrogenic cerebrovascular infarction or hemorrhage | 997.02 | ||
| Subarachnoid hemorrhage | 430 | ||
| Intracerebral hemorrhage | 431 | ||
| Nontraumatic extradural hemorrhage | 432.0 | ||
| Subdural hemorrhage | 432.1 | ||
| Unspecified intracranial hemorrhage | 432.9 | ||
|
|
|||
| Pulmonary embolism & infarction | 415.1, 415.11, 415.12, 415.13 415.19 | ||
|
|
|||
| Postoperative shock not classified elsewhere | 998.0, 998.00, 998.01, 998.02, 998.09 | ||
|
|
|||
| Phlebitis & thrombophlebitis of deep veins of lower extremities | 451.1 | ||
| Phlebitis & thrombophlebitis of lower extremities, unspecified | 451.2 | ||
| Phlebitis & thrombophlebitis of iliac vein | 451.81 | ||
| Phlebitis & thrombophlebitis of unspecified site | 451.9 | ||
| Other venous embolism & thrombosis of inferior vena cava | 453.2 | ||
| Acute venous embolism & thrombosis of deep vessels of lower extremity | 453.4, 453.40, 453.41, 453.42 | ||
| Acute venous embolism & thrombosis of other specified veins | 453.8 | ||
| Other venous embolism & thrombosis of unspecified site | 453.9 | ||
|
|
|||
| Empyema with fistula | 510.0 | Positive airway pressure, CPAP | 94660 |
| Empyema without mention of fistula | 510.9 | Insert emergency airway | 31500 |
| Iatrogenic pneumothorax | 512.1 | ||
| Pulmonary collapse | 518.0 | ||
| Acute edema of lung, unspecified | 518.4 | ||
| Pulmonary insufficiency following trauma & surgery | 518.5 | ||
| Acute respiratory failure | 518.81 | ||
| Ventilator-associated pneumonia | 997.31 | ||
| Continuous invasive mechanical ventilation | 96.70, 96.71, 96.72 | ||
| Noninvasive mechanical ventilation | 93.90 | ||
|
|
|||
| Hemoperitoneum (nontraumatic) | 568.81 | ||
| Hemorrhage or hematoma complicating a procedure not classified elsewhere | 998.1 | ||
| Hemorrhage complicating a procedure | 998.11 | ||
| Hematoma complicating a procedure | 998.12 | ||
| Hematoma of vulva | 624.5 | ||
|
|
|||
| Cystitis | 595 | ||
| Acute cystitis | 595.0 | ||
| Trigonitis | 595.3 | ||
| Other specified types of cystitis | 595.89 | ||
| Cystitis, unspecified | 595.9 | ||
| Urinary-tract infection, site not specified | 599.0 | ||
|
|
|||
| Stricture or kinking of ureter | 593.3 | ||
| Persistent postoperative fistula | 998.6 | ||
| Postoperative infection not classified elsewhere | 998.5x | ||
| Vesical fistula, not classified elsewhere | 596.2 | ||
| Urinary–genital tract fistula, female | 619.0 | ||
| Digestive–genital tract fistula, female | 619.1 | ||
|
|
|||
| Bladder-neck obstruction | 596.0 | Urethral/bladder catheterization (simple) | 51701 |
| Postoperative urethral stricture | 598.2 | Cystourethroscopy with dilation of stricture | 52281 |
| Other specified causes of urethral stricture | 598.8 | Dilation of urethra | 53660, 53661, 53665 |
| Urethral stricture, unspecified | 598.9 | Dilation of urethra stricture | 53600, 53601, 53605, 53620, 53621 |
| Urinary obstruction | 599.6x | ||
| Retention of urine | 788.2x | ||
| Splitting of urinary stream | 788.61 | ||
| Slowing of urinary stream | 788.62 | ||
| Straining on urination | 788.65 | ||
| Cystostomy | 57.1 | ||
| Urethral/bladder catheterization (simple) | 57.94 | ||
|
|
|||
| Rupture of bladder, nontraumatic | 596.6 | Repair of bladder wound | 51860, 51865 |
| Hemorrhage into bladder wall | 596.7 | ||
| Injury to bladder and urethra, without mention of open wound into cavity | 867.0 | ||
| Suture of laceration of bladder | 57.81 | ||
|
|
|||
| Interstitial cystitis | 595.1 | ||
| Dyspareunia/pelvic pain | 625.0 | ||
CPAP, continuous positive airway pressure.