
Abstract
Abstract
Background:
Ovarian torsion is a rare gynecologic emergency in adolescents and, upon diagnosis, immediate surgical intervention is mandatory to salvage the affected ovary. Oophorectomy is conventionally performed when the affected ovary is clinically deemed nonviable. However, a recent conservative method of detorsion and conservation of an apparently gangrenous twisted ovarian cyst has emerged, and it has been proven that seemingly gangrenous ovarian tissue is still capable of remaining viable even after prolonged ischemia.
Cases:
This article reports 2 cases of young adolescents, each of whom presented with an acute abdomen secondary to ovarian cyst torsion. Both patients were managed with two-stage conservative laparoscopic surgery (laparoscopic detorsion followed by interval laparoscopic cystectomy) performed by a general gynecologist in a district hospital. Although the twisted ovary appeared gangrenous during the emergency diagnostic laparoscopy in both cases, detorsion rather than conventional oophorectomy was performed.
Results:
In each case, subsequent second-look laparoscopy revealed viable ovarian tissue, enabling conservation of the ovary by only cystectomy, thus salvaging a previously apparent gangrenous ovary. Histopathologic testing confirmed benign ovarian cysts in both cases.
Conclusions:
Laparoscopic detorsion is currently the preferred choice of treatment for a twisted ovary in an adolescent, despite its gangrenous appearance. This is a simple but crucial procedure that can be performed easily by a general gynecologist with level 2 operative laparoscopic skills. Detorsion would be a superior option to maximize female ovarian reserve and future reproductive potential. (J GYNECOL SURG 34:150)
Introduction
O
This article reports on 2 cases of young adolescents with ovarian cyst torsion. Both cases were managed successfully in a district hospital with 2-stage conservative laparoscopic surgery (laparoscopic detorsion followed by interval laparoscopic cystectomy).
Cases
Case 1
A 19-year-old nulliparous girl presented with right iliac fossa pain, fever, and vomiting for 1 day. Otherwise, she had no abnormal vaginal discharge and her menstrual history was unremarkable. On examination, she was noted to be hemodynamically stable with a low-grade fever (temperature: 37.5°C). There were tenderness, guarding, and a palpable mass at the right iliac fossa. Urinalysis for infection and pregnancy were both negative. Transabdominal ultrasound (US) revealed a right multiloculated adnexal cyst measuring 11 × 7 cm (Fig. 1). A complete blood count test revealed a normal white-cell count of 13.8 × 103/μL. A provisional diagnosis of a twisted right ovarian cyst was made.
Transabdominal ultrasound finding of right adnexal cyst in Case 1.
Emergency diagnostic laparoscopy was performed. Intraoperatively, a right ovarian cyst measuring 10 × 8 cm was seen; it was twisted once at the right infundibulopelvic ligament. The cyst was blue–black in color and gangrenous in appearance. The right fallopian tube was edematous and engorged. Laparoscopic detorsion of this right ovarian cyst was undertaken without any further interventions. Postoperatively, she remained afebrile with resolution of her right iliac fossa pain.
She was discharged well on postoperative day 1 with a plan for an interval cystectomy 3 weeks later. Counseling on risk of retorsion was done prior to discharge. However, she developed an upper respiratory-tract infection when she arrived for this second surgery and the anesthetic team had to postpone the surgery. As she did not have any symptoms of retorsion, she was scheduled for the second-look surgery 3 weeks later. Upon readmission, repeated US showed persistence of the right ovarian cyst. Her tumor markers were normal. During the second-look laparoscopy, the previously gangrenous-appearing right ovary was now white and viable. Laparoscopic right cystectomy was performed and the right ovary was repaired. Histopathologic examination confirmed that she had a benign serous cystadenoma.
Case 2
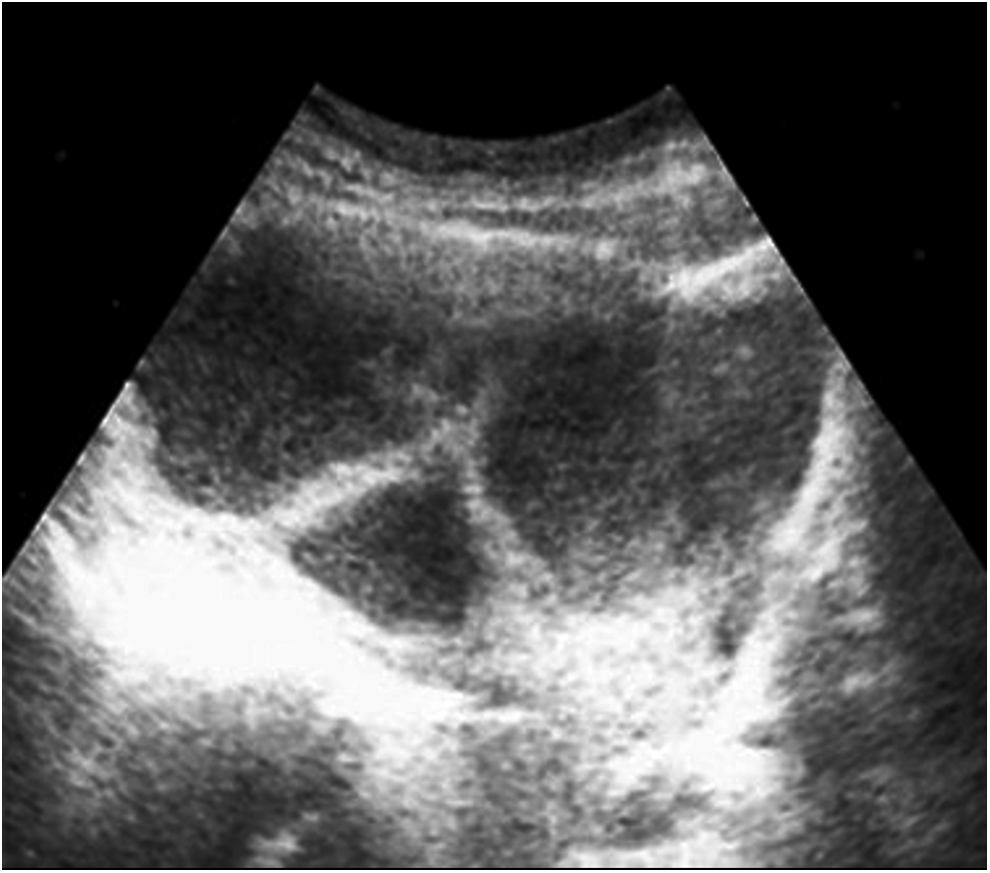
An 11-year-old girl presented with worsening left iliac fossa pain and vomiting for 2 days. She had attained menarche at age 10 and had irregular menstrual cycles. On examination, it was noted that she was afebrile and hemodynamically stable. She had tenderness and guarding at the left iliac fossa. No abdominal mass was palpable. Urinalysis for infection and pregnancy testing were both negative. Transabdominal US revealed a left uniloculated adnexal cyst measuring 7.36 × 5.92 cm with coiling of the left ovarian vascular pedicle and an absence of intraovarian blood flow (Fig. 2). Complete blood count testing revealed leucocytosis of 17.5 × 103/μL. The provisional diagnosis was left ovarian cyst torsion.

Transabdominal ultrasound showed a left adnexal cyst, and a Doppler study showed coiling of the left ovarian vascular pedicle (arrow) and absence of intraovarian blood flow in Case 2.
Following discussion with the patient and her parents, options for surgery, including detorsion, were agreed upon. A diagnostic laparoscopy was performed immediately. Intraoperatively, there was a left ovarian cyst measuring 8 × 7 cm. The cyst and left fallopian tube were found to be twisted three times around the base and both were gangrenous in appearance (Fig. 3). Detorsion was undertaken.

Diagnostic laparoscopic finding of apparent gangrenous twisted left ovarian cyst in Case 2.
The patient's postoperative period was uneventful and she was discharged well on postoperative day 2. She was advised to undergo a second-look laparoscopy 3 weeks after detorsion. However, the parents requested to postpone the surgery for another 5 weeks, as that would have coincided with her school holidays. The parents were also informed about the risk of retorsion.
Subsequent US surveillance showed persistence of the patient's left ovarian cyst. Her tumor markers were normal. The second-look laparoscopy was then undertaken. Intraoperatively, the previously gangrenous-appearing left ovary was now viable (Fig. 4). Laparoscopic cystectomy was performed and the left ovary was repaired. Histopathologic examination of the cyst confirmed a benign serous cystadenoma.
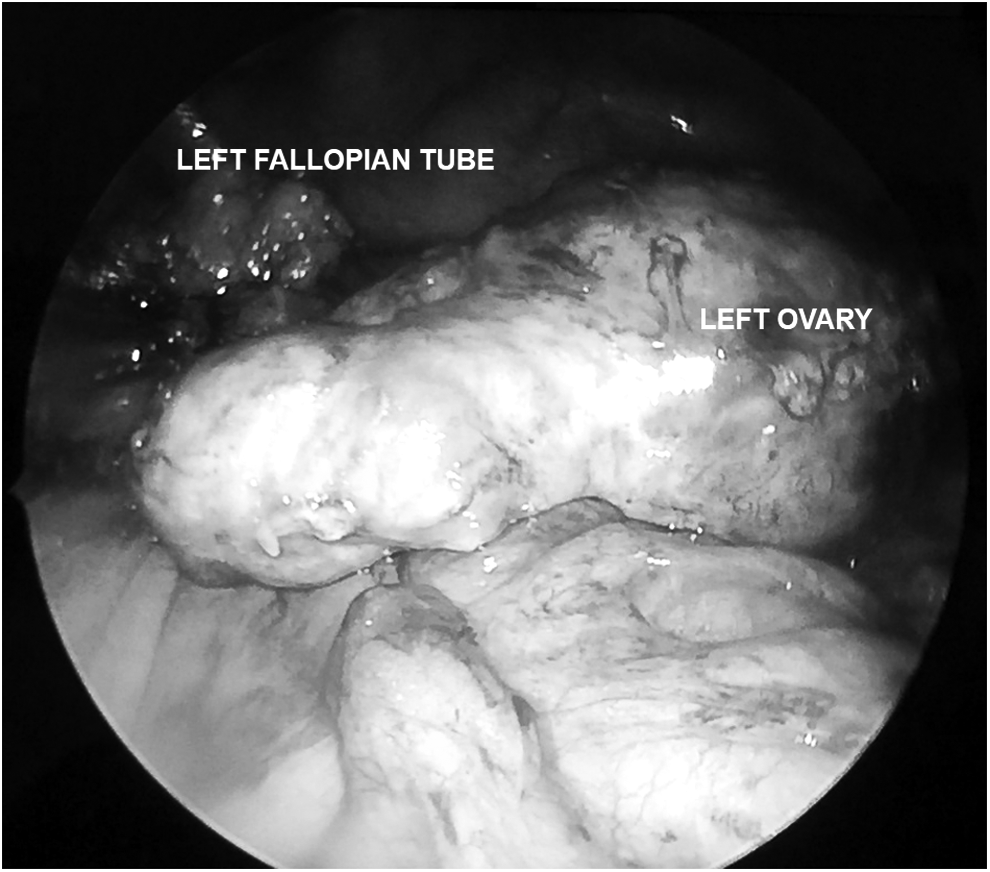
Second-look laparoscopy showed a viable left ovary and left fallopian tube in Case 2.
Results
As mentioned in each case, second-look laparoscopy was performed to remove the cysts, the ovaries were now viable, and the patient's symptoms were resolved.
Discussion
Both cases showed successful adnexa-sparing conservative laparoscopic surgery performed for apparently gangrenous twisted ovarian cysts in adolescents. Conventionally, oophorectomy without untwisting has been the standard treatment for twisted gangrenous ovarian cysts. Many reasons have been cited, such as risk of infection and sepsis if the nonviable gangrenous ovary is not removed, 4 risk of thromboembolism following detorsion, release of an ovarian vein thrombus into the systemic circulation,3–5 and fear of possible malignancy. 4
Current management of ovarian cyst torsion has moved away from surgical resection. Detorsion with adnexal sparing has been advocated as a new approach in the management of twisted ovarian cysts, particularly in young females.2–5 Detorsion can be achieved via a laparoscopy or laparotomy approach, wherein the outcome of ovarian function recovery is similar. 6 Laparoscopic detorsion with blunt laparoscopic instruments was used in both of these 2 cases, considering the advantages of laparoscopy, such as faster recovery, reduced hospital stay, decreased postoperative analgesic requirements, lesser febrile morbidity, and lower risk of postoperative adhesion formation.2,6,7
Ideally, surgery for ovarian cyst accidents in adolescents is performed preferably in a tertiary center with a pediatric and adolescent gynecology service. However, this service is not widely available in the current authors' local setting. Furthermore, the chance of salvaging the affected ovary by detorsion decreases over time, notably when the duration of torsion persists longer than 48 hours. 8 In order to prevent diagnostic and interventional delay, given the presence of a general gynecologist in the district hospital, emergency diagnostic laparoscopy upon admission was performed for both cases. Detorsion was also undertaken laparoscopically, once the twisted ovarian cysts were confirmed. The current authors believe that laparoscopic detorsion is a simple—yet crucial—procedure that is performed easily by a general gynecologist who has level-2 operative laparoscopic skills.
Color Doppler US findings of the “whirlpool” sign of a twisted pedicle and coiling of the ovarian vessels increases the diagnostic potential for torsion. 2 The latter was observed in the second case. Total absence of intraovarian blood flow, which was seen in the second case, might have indicated a relatively late torsion and thus warranted an urgent surgical intervention. 2 Intraoperative appearance of gangrenous adnexa is poorly predictive of ovarian recovery.3,5 Regardless of the severity of a gangrenous twisted ovarian cyst, detorsion could promptly restore ovarian blood supply and salvage more than 80%–90% of affected ovaries.7,9 The 2 current cases showed viable-looking ovaries during second-look surgery after detorsion. This implied that complete arterial occlusion following torsion of adnexa does not commonly occur. 3 In addition, both patients presented less than 48 hours from the onset of the torsions, thus allowing timely detorsion to restore ovarian perfusion, so that the likelihood of preserving viable ovaries would increase. 8
Case studies have also revealed that the perceived increased risk of postoperative infectious morbidity is overstated. 3 Transient postoperative fever and ileus—which did not occur in the 2 current cases—are more common following laparotomy rather than laparoscopic detorsion.6,7
The documented risk of risk of pulmonary embolism is 0.2%, although surgical resection without untwisting is undertaken. 4 Nevertheless, recent evidence revealed that detorsion does not increase the risk of pulmonary embolism.6,7
The risk of finding ovarian malignancy in young girls with twisted ovarian cysts is lower than 0.5%. 1 Furthermore, a malignant ovarian tumor is less likely to be twisted due to underlying inflammation and adhesion. 10 In both of the current cases, the twisted ovarian cysts were benign in nature. Furthermore, the tumor markers were normal and diagnostic laparoscopy showed no periovarian adhesions and intra-abdominal metastasis. All of these factors, coupled with the rarity of ovarian malignancy in this age group, makes the possibility of ovarian malignancy highly unlikely.
It is recommended to perform elective cystectomy after an interval of 3 weeks to allow resolution of edema.2,5 Concurrent cystectomy from a gangrenous ovary is avoided, as it poses technical difficulty attributed to absence of a clear plane of cleavage between the cyst wall and ovarian tissue, risk of bleeding, and risk of inadvertent removal of normal ovarian tissue.4,7 For both of the current patients, interval laparoscopic cystectomy was performed later than the recommended 3-week interval after detorsion due to an upper-respiratory tract infection in the first case and the parental request in the second case. The risk of retorsion (4.9%) was emphasized to the patients. 7
Oophoropexy was not performed in either of these patients, each of whom had a first episode of a twisted ovarian cyst. The role of routine oophoropexy in preventing recurrence of torsion adnexa is still controversial in this context. Furthermore, oophoropexy could distort the anatomical tubo-ovarian relationship and impair the fallopian tubal blood supply and function, thus posing a risk of infertility in the future. Nevertheless, oophoropexy could be considered for certain patients with bilateral ovarian torsion, recurrent torsion, or ovarian torsion attributed to excessively long utero-ovarian ligaments.4,5
Conclusions
Laparoscopic detorsion is currently the preferred choice of treatment for twisted ovaries in adolescents, as illustrated in both of these current cases. It is a simple procedure that is easy to perform by a general gynecologist with level-2 operative laparoscopic skills. Despite the dusky and gangrenous appearance of the ovary, there is still a high rate of ovarian revival after detorsion. The perceived risk of infectious morbidity, thromboembolism, and malignancy has been shown to be negligible. Owing to future risk of infertility, oophoropexy should not be performed routinely in first-episode cases of adnexal torsion.
Footnotes
Acknowledgment
The authors would like to thank the Director of Health Malaysia for permission to publish this paper.
Author Disclosure Statement
The authors declare that they have no conflicts of interest and nothing to disclose.