
Abstract
Abstract
Background:
High-grade endometrial stromal sarcomas (HGESS) are very rare uterine tumors, and HGESS during pregnancy is exceedingly rare. This is the first-ever published case of a uterine sarcoma with a concurrent pregnancy that was treated successfully with surgery and adjuvant chemotherapy.
Case:
A 24-year-old, gravida 1, female at 12 weeks of gestational age presented with vaginal bleeding and was found to have a cervical polyp with spindle-cell malignancy on biopsy. The patient underwent a hysterectomy, bilateral salpingectomy, and lymph node dissection with ovarian preservation.
Results:
Pathology was diagnostic of HGESS. The patient received adjuvant chemotherapy and remained in remission 15 months postoperatively.
Conclusions:
Surgery and adjuvant chemotherapy should be strongly considered for the treatment of HGESS during pregnancy. Ovarian preservation should be considered for patients desiring future fertility. (J GYNECOL SURG 34:105)
Introduction
E
Given the rarity of HGESS, most of the literature is based on small series or case reports. Only 1 case report has ever been published on HGESS during pregnancy. In that case, a 28-year-old female at 15 weeks of gestation presented with pelvic pain. Ultrasonography was suggestive of an ovarian mass. Laparoscopy revealed diffuse peritoneal tumor growth that was evident without clear visualization of the uterus and ovaries. Pathology was significant for ESS. Cytoreductive surgery was attempted; however, dense tumoral involvement of the omentum and small and large bowel prevented significant cytoreduction. Chemotherapy was considered futile, so the patient was given supportive care and died within 6 weeks of diagnosis. 5
The current authors report the second-ever published case report of HGESS complicating a pregnancy and the first-ever published case of a uterine sarcoma with a concurrent pregnancy that was treated successfully with surgery and chemotherapy. This case is significant because it highlights the unusual presentation of endometrial sarcoma and the wide variation in treatment options. A literature review on treatment of endometrial sarcoma is also presented in this article.
Case
A 24-year-old, gravida 1, female at 12 weeks of gestational age presented with painless vaginal bleeding. A pelvic examination revealed a cervical polyp that was biopsied and significant for spindle-cell malignancy surrounding benign endocervical-type glands. Abundant mitotic figures were present in addition to prominent thick-walled vessels (Fig. 1.). CD10 immunostaining was positive in a patchy distribution. Cyclin D1 was present in >50% of the tumor nuclei, which raised concern regarding a potential diagnosis of UES. Magnetic resonance imaging of the abdomen and pelvis was significant for a single intrauterine pregnancy and a 2.5 × 2.7 cm polypoid mass extending into the superior aspect of the vagina (Fig. 2). The patient was extensively counseled on the risks and benefits of surgical management, including the loss of her current pregnancy. At 14 weeks and 3 days of gestation, the patient underwent a total abdominal hysterectomy, a bilateral salpingectomy, and staging with lymph node dissection. Both ovaries were preserved, given their grossly normal appearance and the patient's desire for future surrogacy.
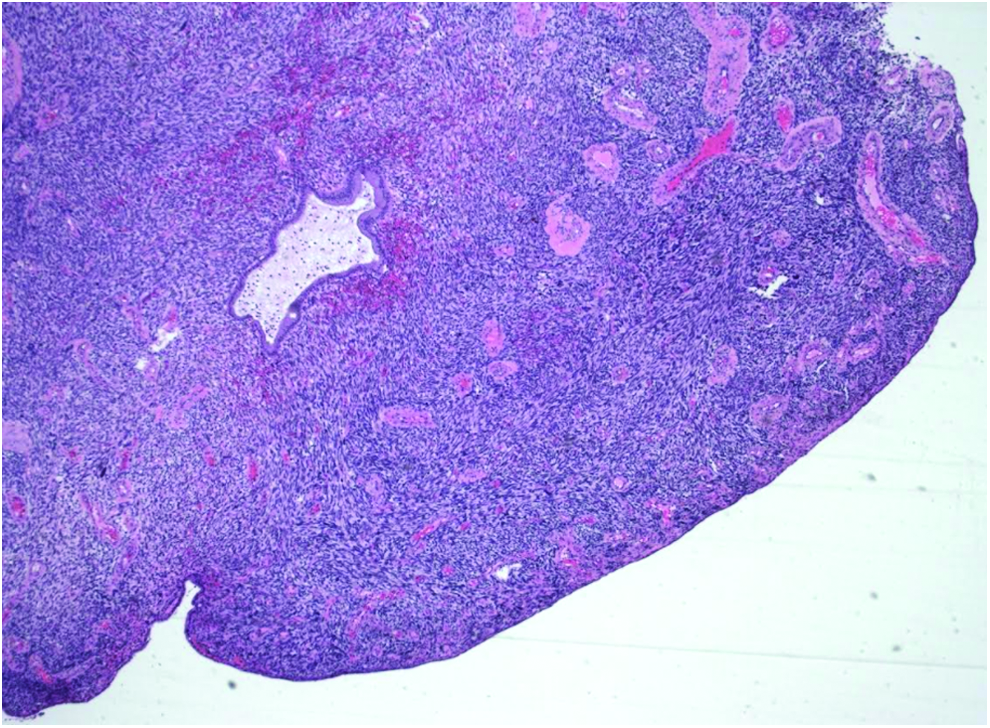
Initial cervical biopsy of polyp showing spindle-cell malignancy with prominent thick-walled vessels. Color images available online at www.liebertpub.com/gyn
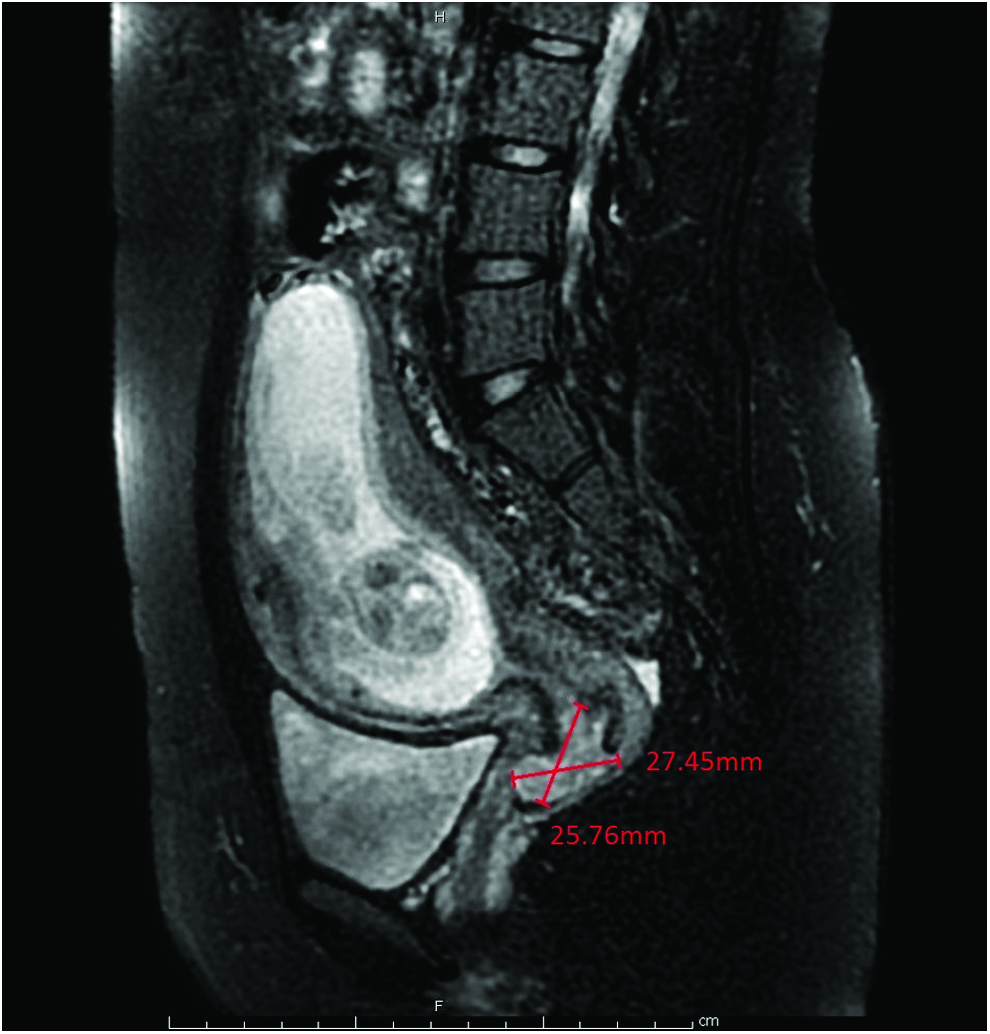
Single intrauterine pregnancy and 2.5 × 2.7–cm polypoid mass extending into the superior aspect of the vagina. Color images available online at www.liebertpub.com/gyn
Pathology revealed a stage I, upper endocervical canal high-grade sarcoma with 0.2-cm myometrial invasion (Figs. 3, 4, and 5). Histology revealed a malignant spindle-cell lesion arising in the upper endocervical canal with moderate nuclear atypia and a mitotic rate of up to 78 per 10 high-power fields (Fig. 6). Immunohistochemistry showed moderate CD10 positive staining, with cyclin D1 staining positive in >70% of the tumor nuclei. Estrogen receptor (ER), progesterone receptor (PR), CD117, smooth-muscle actin (SMA), desmin, caldesmon, and keratin stains were negative. (Figs. 7 and 8). Molecular studies did not reveal any identified rearrangements within the JAZF1, PMF1, or YWHAE gene regions. These findings were most consistent with endometrial stromal differentiation. Additionally, lymph node biopsies were negative for tumor spread.

Uterus with grossly normal 15 week fetus, placenta, and 2-cm polypoid mass at the endocervical canal. Color images available online at www.liebertpub.com/gyn

A 2-cm polypoid mass at the endocervical canal. Color images available online at www.liebertpub.com/gyn

Tumor cells with 0.2 cm of myometrial invasion. Color images available online at www.liebertpub.com/gyn
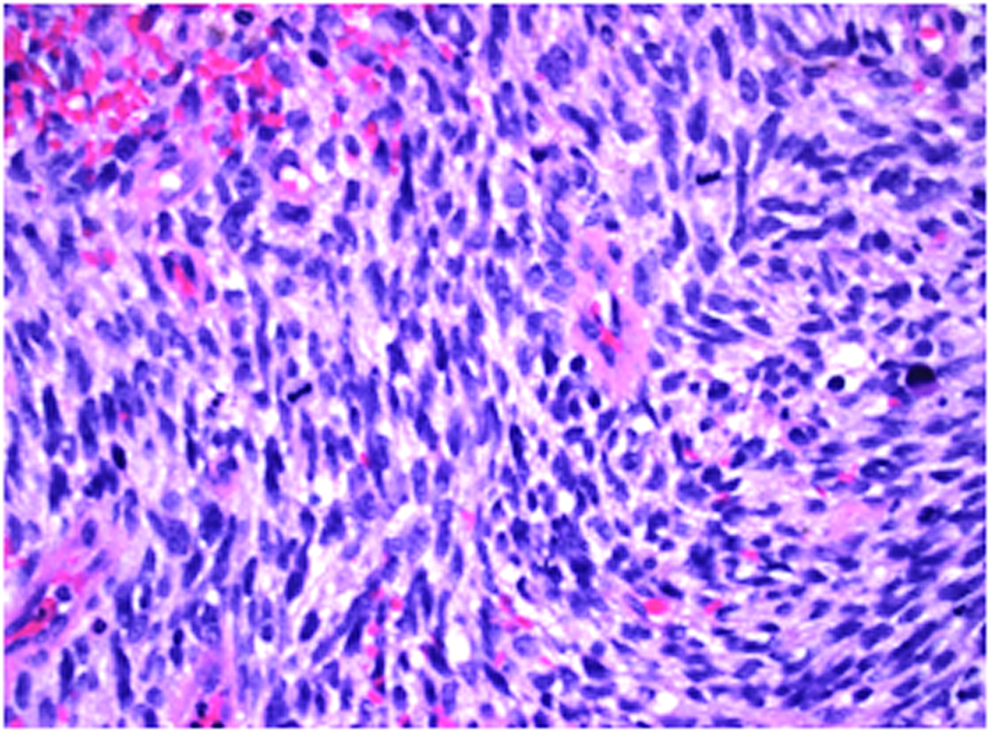
Spindle-shaped tumor cells showing nuclear atypia with prominent mitoses. Color images available online at www.liebertpub.com/gyn

Tumor cells showing >70% cyclin D1 nuclear staining. Color images available online at www.liebertpub.com/gyn
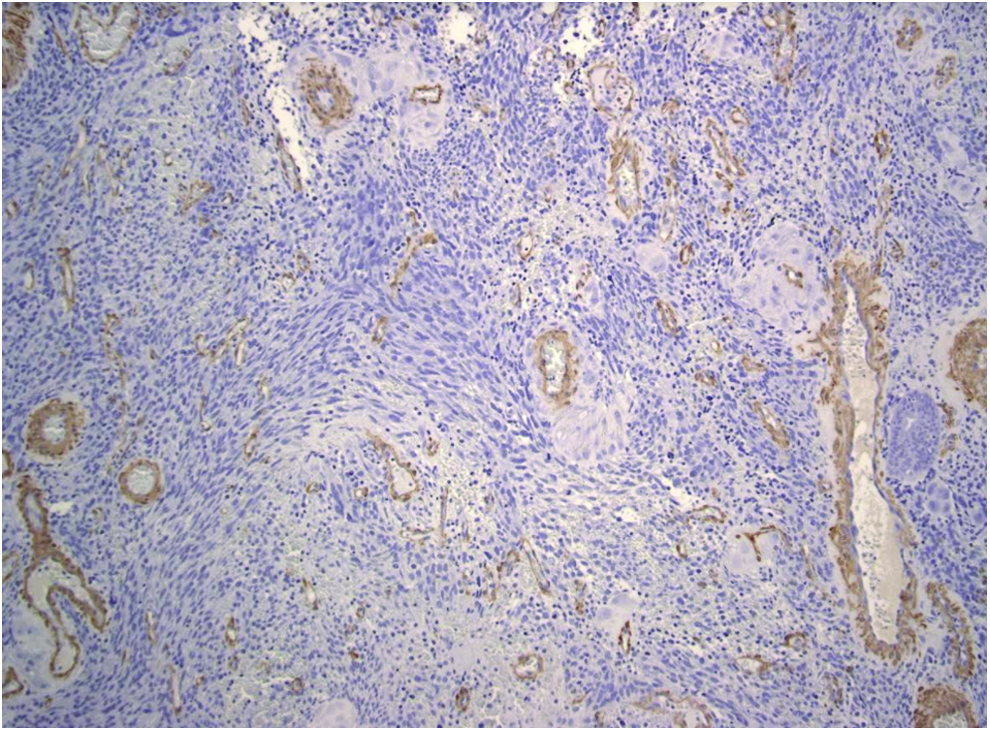
Tumor cells negative for smooth-muscle actin. Color images available online at www.liebertpub.com/gyn
Results
There were no surgical complications, and the patient was discharged on postoperative day 3. She was treated with 6 cycles of gemcitabine and taxotere and remained recurrence-free 15 months postoperatively.
Discussion
To the best of the current authors' knowledge, this case is the second-ever published case report of HGESS complicating a pregnancy and the first-ever published case to have been successfully treated with surgery and chemotherapy.
In this case, pathology testing revealed malignant invasion of the myometrium and histology testing showed spindle-cell tumors with moderate nuclear atypia and a high mitotic rate. Immunohistochemistry testing revealed diffuse cyclin D1 nuclear staining, which is diagnostic for HGESS, based on the 2014 WHO guidelines. ER, PR, CD117, SMA, desmin, caldesmon, and keratin stains were negative, ruling out the diagnosis of endometrial carcinoma or leiomyosarcoma. Molecular studies were performed looking for mutations in the JAZF1, PMF1, or YWHAE gene regions but were negative for such mutations. However, based on the constellation of available pathologic evidence, the current authors believe the tumor is best characterized as an HGESS.
Specific treatment regimens remain controversial, and additional research is needed. Treatment is primarily surgical, and typically includes total abdominal hysterectomy with bilateral salpingo-oophorectomy. Lymph node dissection is not thought to be beneficial for patients with low tumor volume and no other clinical or imaging findings of nodal disease. 6 However, given the concern regarding the pathology on the initial biopsy of the cervical lesion, and the accessibility of the lymph nodes at the time of surgery, lymph node dissection was performed. The National Comprehensive Cancer Network® treatment guidelines for stage I HGESS include observation or systemic therapy (Category 2B) with combination regimens or single-agent chemotherapy. 7 The addition of adjuvant radiotherapy or chemotherapy is controversial. Docetaxel + gemcitabine is a common regimen, largely based on its efficacy for treating leiomyosarcoma. 8 Other studies suggest the addition of doxorubicin could be of benefit. 9 However, the body of evidence remains lacking and further investigation is needed.
While there is little literature regarding ovarian preservation in HGESS, studies of LGESS suggest that ovarian preservation is not a significant prognostic factor for disease recurrence or survival.10,11 Given the lack of metastasis or nodal involvement, and the patient's desire for future surrogacy, ovarian preservation was considered to be reasonable. Oocyte cryopreservation may be another consideration—particularly if chemotherapy is being considered—and should be discussed on a case-by-case basis. Additionally, the benefits of ovarian preservation including cardioprotective effects and osteoporosis risk reduction, were considered given the patient's young age.
After thorough discussion with the patient regarding the high-risk histology of her tumor, she chose to undergo ovarian-sparing surgery with adjunctive chemotherapy, and her cancer remained in remission 15 months after treatment.
Conclusions
Important points to consider are:
1. Endometrial stromal tumors include ESNs (benign), LGESS, HGESS, and UES. 2. ESS are very rare malignant tumors, accounting for ∼0.2% of all uterine cancers. HGESS detected in pregnancy is exceedingly rare. 3. Ovarian preservation can be reasonable in cases of HGESS. The decision should be made on a case-by-case basis after consideration of future surrogacy, cardioprotective effects, and osteoporosis risk reduction.
Footnotes
Acknowledgments
The authors would like to thank the Kapiolani Women's Cancer Center in Honolulu, HI, for their dedication to patient care.
Author Disclosure Statement
The authors have no actual or potential conflicts of interest with respect to this article. No financial support was provided.