
Abstract
Abstract
Objective:
The aim of the present study was to examine feasibility, safety, and efficacy, in the first postmarket case series in gynecologic surgery, using an integrated table motion (ITM) device, which is a new surgical device including a unique operating table that connects wirelessly with the da Vinci® Xi surgical platform. This new feature is expected to advance robotic surgery and the field of minimally invasive gynecologic surgery.
Materials and Methods:
This was a prospective postmarket study, performed with ITM in 11 women who underwent gynecologic surgery. Primary endpoints were ITM feasibility, safety, and efficacy.
Results:
During the 11 gynecologic surgeries, there were 35 instances of table moves. The ITM length was <1 minute per movement in 25 of 35 moves (71%). During total robotic hysterectomy (TRH), the mean number of ITM movements was 3.1, resulting in 28 instances of table movements. During pelvic organ prolapse (POP) surgery, the mean number of ITM moves was 3.5, resulting in 7 instances of table moves. The mean duration of each table motion was 30 seconds during TRH, compared with 94 seconds during POP surgery. Of 35 ITM moves, 32 were performed to achieve internal exposure in the pelvis. The endoscope as well as the instruments remained inserted during 88% of table movements. No adverse events and no ITM safety-related remarks were noted in the medical records.
Conclusions:
Preliminary analysis of the early experience with using an ITM device as a new operating table, which communicates with da Vinci Xi platform, indicated the feasibility, safety, and efficacy of the ITM for different gynecologic surgeries. The small number of subjects in the first worldwide series of gynecologic surgeries as well the diversity of surgical procedures are not yet enough to provide definitive scientific evidence about the use of this device. However, the present study on humans concerning the use of ITM, highlighted the development of this new tool for robotic surgery performed for both benign and malignant gynecologic diseases. (J GYNECOL SURG 34:144)
Introduction
T
The integrated table motion (ITM) device for the da Vinci Xi robotic platform (Intuitive Surgical Inc., Sunnyvale, CA; Figs. 1–3) is a novel surgical tool comprised of a unique operating table (TRUMPF Medizin Systeme GmbH & Co., Saalfeld, Germany) that connects wirelessly with the da Vinci Xi platform allowing reposition of a patient without undocking robotic arms and without removing robotic tools from inside the patient's abdomen.
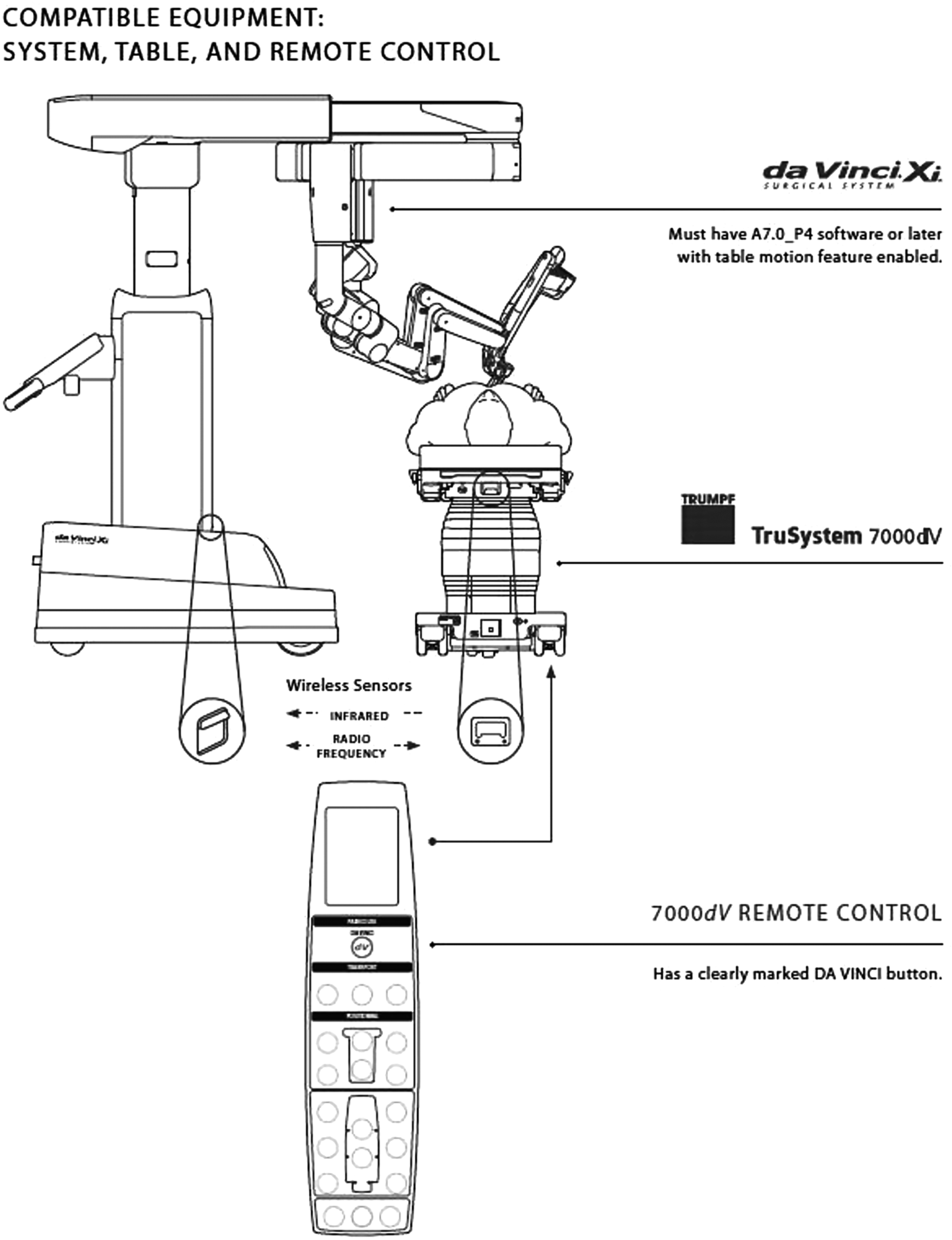
Illustration of integrated table motion (ITM) for the da Vinci® Xi surgical system (Intuitive Surgical Inc., Sunnyvale, CA). ITM is a new feature comprising a unique operating table (TRUMPF Medizin Systeme GmbH & Co., Saalfeld, Germany) that communicates wirelessly with the da Vinci Xi. The da Vinci Xi surgical system and the TruSystem 7000dV operating table (TS7000dV; TRUMPF Medizin Systeme) have been specifically developed to address some technical limitations of the da Vinci Si surgical system, and to improve robotic surgery. Illustration used with permission from © 2018 Intuitive Surgical, Inc.

Parts of different components of ITM in the operating room.

The TruSystem 7000dv (TRUMPF Medizin Systeme GmbH & Co. Saalfeld, Germany) operating table simulating how they would move together while docked. Illustration used with permission from © 2018 Intuitive Surgical, Inc.
The da Vinci surgical system and the TruSystem 700dV operating table (TS 7000dV, TRUMPF Medizin Systeme) were exclusively planned to overcome some intraoperative restrictions of the previous da Vinci Si platform in order to advance robotic surgery.
A significant technical hitch with the previous da Vinci Si system during robotic surgery was the incapability to change the operating table position simultaneously with the robotic arms and its tools docked. This drawback can be largely increased in pelvic operations in which orientation in a narrow space, identification and characterization of deep anatomical structures, and perception of the instruments' location in relation to the position of anatomical targets are difficult and potentially risky. 4
In the last 15 years, the use of robotic support in gynecologic surgery has grown on a global scale, especially improving more-challenging gynecologic operations or surgical steps that typically need careful and accurate manipulation of tissue, that have narrow working spaces, and deep anatomical landmarks, thus, limiting the surgeon's sense of orientation in the pelvis during surgical procedures. 5
The new da Vinci Xi system enables moving a patient without undocking the robotic arms and with robotic instruments still inside the abdomen, thus reducing hitches associated with timely access tasks, poor exposure, or patient safety.6,7
Thus, gynecologic and pelvic surgery, in which conservative or tailored approaches are often required, has been recognized as a central application for experimenting with the new ITM device. 8 The aim of this postmarket study was to assess the efficacy, feasibility, and safety of the new operating table ITM for the da Vinci Xi robotic system when performing robotic pelvic surgery for different gynecologic procedures.
Materials and Methods
Between May and October of 2015, the first human use of the new ITM was approved in a postmarket study in the European Union. For this study, 40 patients in need of different surgical specialties (gynecology, urology, general surgery) were prospectively enrolled. The gynecologic subgroup of that study included 11 patients. The ethics committee of the University of Pisa in Pisa, Italy, approved this study protocol.
Morelli L. et al. provided an accurate description of the Materials and Methods details and a Technical Device note for that study. 9
Primary endpoints of the current study were ITM feasibility, efficacy, and safety.
Feasibility and efficacy were assessed by evaluating the number of ITM movements performed per case, duration of each table motion, table position attained, causes for moving the operating table, and position of the instruments and camera (inserted or removed) during ITM movement.
The safety of ITM was analyzed by assessing patients' estimated blood loss (EBL); urine volume; total administered fluid; pre-and postoperative mean blood pressure (BP) and heart rate (HR); port-site condition; intra- and postoperative complications; adverse events related to the use of the new operating table ITM in terms of injuries to tissue, nerves or organs; and hospital stays (Table 1).
ITM, integrated table motion; ASA, American Society of Anesthesiologists; TRH, total robotic hysterectomy; POP, pelvic organ prolapse.
Technical features of ITM
The TruSystem 7000dV operating table can interact with the da Vinci Xi surgical system to support ITM, enabling table motion with the robotic side-cart while it is docked (attached) to cannulas inside the patient. The operating table is an optional third-party auxiliary product for use with the da Vinci Xi system; it is not required for normal use of the da Vinci Xi system. Two types of wireless interfaces (infrared and radiofrequency) enable communication between the table interface module (TIM) in the da Vinci Xi system and the operating table. A remote connected to the table via cable is used by surgical staff to command table motion (Fig. 1). The da Vinci ITM allows the surgical staff to reposition a patient by adjusting the table while still docked to the da Vinci Xi surgical system. When users turn on the ITM, brakes release the joints of the da Vinci Xi system's patient cart, allowing the instrument arms to move with the patient passively and safely. If instruments remain on the arms during the motion, the surgeon must have them in view and under active control for the table motion to be allowed. When users turn off da Vinci ITM, these joint brakes reapply, and the arms return to typical surgical use. If the joints reach a range of motion limit during ITM, the boom compensates by moving in a direction that gives the arms additional range of motion. 9
Statistical analysis
Studied variables were analyzed retrospectively after institutional review board approval. Sample characteristics were assessed using descriptive statistics. Continuous variables were expressed as the mean, median, and range, whereas categorical variables were expressed as counts and percentages.
Statistical analysis was performed using the statistical package SPSS®, version 17 (SPSS Inc., Chicago, IL).
Results
Technical intraoperative features
Throughout the study duration, 9 women underwent total robotic hysterectomy (TRH) with ITM, and 2 patients underwent surgery for pelvic organ prolapse (POP). Of these 11 patients, 1 underwent lateral suspension for an hystero-cystocele,1 patient underwent sacral rectopexy for repair of a posterior pelvic prolapse, 5 patients underwent TRH for benign uterine pathology, and 4 patients underwent TRH for malignant indications; the patients with oncologic conditions underwent associated bilateral lymphadenectomy. In consideration of menopausal presurgical conditions, 8 of the 9 TRH women underwent concomitant bilateral salpingo-oophorectomy. The mean operating room enter/exit time was 144 minutes (range: 117–240 minutes) and the mean robotic time was 110 minutes (range: 83–192 minutes). Targeting success was obtained in all cases. The mean number of ITM movements was 3.3 (range: 1–6 movements), resulting in 35 instances of total table moves in the 11 different surgical procedures. The mean duration of each table motion was 43 seconds (range: 6–73 seconds). The required table position was realized in all cases.
The reasons for moving the ITM was to gain internal exposure in 32 moves (91%), to perform endoscopic observations in 2 moves (6%), and to improve external access in 1 move (3%). The endoscopic camera remained inserted during 31 of the 35 table movements (88%), and the instruments were left inserted during 31 of the 35 table movements (88%). The ITM length was <1 minute per movement in 25 of 35 moves (71%). During TRH, the mean number of ITM movements was 3.1, resulting in 28 instances of table movements. During POP surgery, the mean number of ITM moves was 3.5, resulting in 7 instances of table moves. The mean duration of each table motion was 30 seconds during TRH, compared with 94 seconds during POP surgery. The most frequent cause for moving the operating table during TRH was to gain internal exposure. The reason for moving operating table during POP surgery was to gain internal exposure in all cases.
Patients' perioperative outcomes
The mean EBL was 52 mL (range: 0–400 mL), mean urine volume was 783 mL (range: 350–1800 mL), and mean total volume of administered fluid was 2550 mL (range: 2000–4000 mL). The mean pre-and postoperative BPs were 132/75 mm Hg (range: 100–155 mm Hg) and 125/70 mm Hg (range: 195–155 mm Hg), respectively. The mean pre-and postoperative HRs were 65.4 beats per minute (bpm; range: 52–84 bpm) and 56.3 bpm (range: 43–81 bpm), respectively. The mean hospital stay was 3.6 days (range: 2–5 days).
Complications and adverse events
The port-site condition was intact and uncomplicated in all analyzed cases. No external instruments collisions or other problems related to the new ITM were noted. There were no ITM-related intra- and postoperative complications or need to convert to traditional laparoscopy or laparotomy. There were no ITM safety-related observations and no adverse events (Table 2).
ITM, integrated table motion; TRH, total robotic hysterectomy; POP, pelvic organ prolapse.
Discussion
This early experience demonstrated that the use of ITM when performing gynecologic surgeries with da Vinci Xi is feasible. The ITM permitted patient relocation without interrupting operative workflow by allowing the surgeon to leave robotic tools in the abdomen of the patient and the endoscope docked to the patient. An ITM makes it possible to move the operating table without removing surgical instruments from inside the patient, thus simplifying the surgery flow, without taking time to undock or redock the robotic platform. In these circumstances, compared to the conventional laparoscopic technique, the da Vinci Xi, together with ITM technology, offers the possibility of maximizing gravity exposure and provides easy and rapid access to narrow and deep spaces of the female pelvis, access that is essential in gynecologic procedures. These dynamic changes can be performed robotically by modulating the Trendelenburg and lateral tilt of the ITM without undocking robotic arms from the patient. Interestingly, in the gynecologic subgroup of patients, most ITM movements during these surgeries took <1 minute, allowing accurate modulation during all operative steps and main surgical phases that were not possible without its use.
With increasing expertise with ITM and, after having assessed its safety, the current authors tried to follow a standardized operative approach regarding movements and reasons for the usage of the new operating table for TRH, but this was not possible for POP surgery because of the small number of patients with POP who were enrolled for ITM surgery. During TRH, the patient was commonly positioned in a shifting 21°–30° Trendelenburg position in relation to different surgical steps or the patient's specific anatomical setting and needs. During lymphadenectomy, the patient was tilted to the right or left for iliac-vessel exposure. In cases of robotic POP surgery, the patient was generally arranged in a shifting 24°–31° Trendelenburg position. In these 2 cases, the maximum Trendelenburg position was required in order to obtain good exposure of the rectovaginal and vesical–vaginal spaces during deep dissection of these anatomical sites. In this view, ITM provided stable patient repositions and powerful gravity traction under the surgeon's control offering ideal exposure of the anatomical landmarks during all surgical steps.
It is plausible to speculate that the TruSystem 7000dV could increase patient safety in extreme Trendelenburg positions also for gynecologic procedures. In this preliminary experience in the first gynecologic series, some anesthesiology parameters were considered as indirect signs of ITM safety.
Remarkably, there were no significant hemodynamic modifications during different surgeries. Furthermore, pre-and postoperative BPs and HRs were comparable. ITM seems to offer the anesthesiologist team to control patient positioning exactly and display the table position to the entire surgical team, considering that the degree of Trendelenburg positioning and tilt are shown on the remote, Vision System Cart monitor, and surgeon side console monitor.
ITM could provide patient relief during Trendelenburg-position surgery, not only from a hemodynamic point of view but also by counteracting increased intraocular pressure, and neurologic or soft-tissue injuries. Furthermore, ITM seems able to minimize the use of extreme positions by starting with a less extreme patient Trendelenburg position and shifting to more extreme positions only when required.
In gynecology, robotic surgery advances the valuable role played by minimally invasive surgery further because of robotic surgery's innate advantages over conventional laparoscopic surgery, including improved instrument dexterity, higher degrees of freedom for instrument movement, and a three-dimensional view with a more-magnified view and filtered tremor. A short learning curve seems to be another possible advantage. In the TRH procedure, management of ureters and uterine vessels are the main, risky, and complex surgical steps, while, in POP procedures, robotic technique could enhance surgeries more than the canonical laparoscopic technique, leading to safer dissection and more accurate suturing and mesh placement.10–12
Future advances in robotic platforms and tools will probably ensure that robotic surgery becomes a better surgical approach for patients benign and malignant gynecologic diseases than conventional robotic instruments. However, no well-designed prospective trials have yet compared different robotic platforms or devices. Moreover, long-term surgical outcomes after robotic operations, using different platforms and tools, have not been evaluated because of the short time passed since the adoption of robotic surgery for the management of gynecologic patients. 3
In this view, the new surgical configuration of the da Vinci Xi platform associates the functionality of a boom-mounted system with the flexibility of a mobile platform.
The newest creation of Intuitive Surgical systems seems more capable of being steered than its precursor da Vinci Si, thus indicating a significant transformation and improvement in structure and function compared with the preceding robotic platforms. However, it is well-known that the Xi platform is characterized by static patient positioning, which bounds the working area in some restricted spaces such as the pelvis. Thus, sometimes, undocking, robotic tools' removal, and cart repositioning could be essential for improving surgical exposure or patient safety, equally as needed with the earlier da Vinci Si. In some cases, these procedures may disrupt the flow of the surgery.6,7
Limitations of the present study are related to the small number and the heterogeneity of analyzed surgeries encompassing benign, malignant, and POP surgery, and the differences in the learning curves of surgeons, thus preventing absolute conclusions about ITM's technical advantages in reduction of total surgical operative times or other improvements.
For these reasons, the assessment of a standardized approach regarding table changes and motivations for ITM usage for both TRH and POP procedures is still premature. However, additional studies are required and could show whether ITM could improve minimally invasive surgeries or function as parts of procedures to be performed robotically that would otherwise be challenging. Additional studies could also show whether ITM could enhance surgical performance by decreasing operating time. The analysis of costs is also critical in the complete evaluation of these innovative devices.
Gynecologic procedures require a deep operative field in the pelvis and anatomical areas that often are localized in narrow spaces. The introduction of the new robot da Vinci Xi in surgical practice and the novel ITM that is able to connect wirelessly with the robotic platform can overcome the critical drawbacks of robotic surgery, while preserving its particular technical benefits. Even if acquired data derived from a small and miscellaneous subgroup of patients detracts somewhat from the data's scientific value, this limited experience using ITM might be potentially important for uterine surgery (for both benign and malignant cases) and POP surgery to achieve all operating phases, maximizing exposure because of the robotic dexterity.
Conclusions
The data obtained from the gynecologic subgroup of this study showed, in a preliminary analysis, that ITM was safe and no adverse events related to its use occurred in the first 11 gynecologic procedures. An ITM could allow gynecologists to amplify all the pros of the robotic technique while reducing its intrinsic limits, facilitating a faster approach to different anatomical areas during surgeries that involve difficult target parts of human anatomy. Moreover, patient safety is improved, as it is possible to modify extreme positions to reach an optimal compromise between good visceral exposure and anesthesiology risks. The analysis of a larger number of cases will help assess different standardized approaches regarding table movements and reasons for ITM usage specifically for different fields of gynecologic surgery.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.