
Abstract
Abstract
Background:
Signet-ring cell tumor of the ovary is a rare condition in gynecology. All of the English literature was checked for the terms
Case:
A 33-year-old woman, who had been diagnosed with Hodgkin's lymphoma, appeared to have a solid-cystic mass of 59 × 49 × 37 mm in the right adnexial region after receiving treatment for her Hodgkin's lymphoma. She was operated on, and her condition was diagnosed as a signet-ring cell stromal tumor of the ovary. This diagnosis was histologically confirmed.
Results:
There was no recurrence of the patient's disease ∼14 months later at follow-up.
Conclusions:
Signet-ring cell stromal tumor of the ovary is an extremely rare kind of ovarian tumor. In the English literature, fewer than 20 cases have been reported. In addition, the current patient is the first case of signet-ring cell tumor of the ovary diagnosed after treatment of Hodgkin's lymphoma. There have been 17 established cases of this type of tumor in the English literature as of this writing. (J GYNECOL SURG 34:154)
Introduction
R
Hodgkin's lymphoma is a rare B-cell malignant neoplasm affecting ∼9000 new patients yearly. Staging of this disease is essential in order to choose optimal therapy. Prognostic models to identify patients at high or low risks for recurrence have been developed, and these models, along with positron emission tomography, are used to provide optimal therapy. 7 At the beginning, treatment for patients with this disease is based on the histologic characteristics of the disease, the stage at presentation, and the presence or absence of prognostic factors associated with a poor outcome. Radiotherapy and chemotherapy are used alone or combined. Patients with early stage Hodgkin's lymphoma generally received combined-modality therapies that include chemotherapy followed by involved-field radiation treatment. 8 In contrast, patients with advanced-stage Hodgkin's lymphoma commonly receive a more-prolonged course of combination chemotherapy, with radiation therapy used only in selected cases. 7
The association of Hodgkin's lymphoma with signet-ring cell stromal tumor of the ovary has not been reported before in the English literature. The current authors checked all the English literature, using the terms
Informed consent was obtained from the patient to publish this case report.
Case
A 33-year-old gravida 1, para 1, woman had received chemotherapy and radiotherapy 11 years prior and autologous bone-marrow stem-cells transplanted 10 years prior as treatments for Hodgkin's lymphoma. She was now diagnosed with a solid-cystic mass of 59 × 49 × 37 mm in the right adnexial region. The mass was noticed during a routine follow-up.
Her menarche had begun at age 11 and her menses had been normal until she reached age 23. Her menses had stopped for 2 years after she had the autologous bone marrow transplantation. Yet, after the treatment, she had a healthy baby spontaneously. After her pregnancy she had regular menses with a 29-day cycle and a flow lasting for 4 days. Then, her menses stopped again in January of 2017. Her ß-human chorionic gonadotropin was negative, her follicle stimulating hormone value was 111 mIu/mL, and her luteinizing hormone was 54 mIu/mL.
Her past medical history included no diseases, except for Hodgkin's lymphoma. She received radiotherapy, 6 cycles of adriablastine+bleomycin+vinblastine+dacarbazine combination chemotherapy, 2 cycles carmustine+etoposide+cytarabine+melphalan combination chemotherapy, and then autologous bone marrow was transplanted. Her family history was unremarkable.
Her physical examination was unremarkable. She had an essentially healthy appearance and normal vital signs. Vaginal speculum examination revealed a normal vagina and cervix. Bimanual pelvic examination revealed an anteflexed normal-sized uterus and a mobile right adnexal mass. The left adnexa could not be palpated.
A Doppler ultrasound was performed. An ∼60-mm mass was noticed on the lateral side of the right ovary. MRI showed a solid-cystic lesion that was hypointense on T-1–weighted images and heterogeneous hyperintense on T-2–weighted images (Fig. 1).

Signet-ring cell stromal tumor of the ovary appearance on magnetic resonance imaging.
Her laboratory tests showed that her CA-125 was 52 international units(IU)/mL; her CA-1-5-3 was 21 IU/mL, and her CA-19-9 was 1 IU/mL. The results of hematocrit, hemoglobin, liver function, and renal function tests were normal.
An abdominal CT had shown no pathology in the adnexial regions 6 years prior.
A laparoscopic unilateral salpingo-oophorectomy was performed. During the surgery, the mass, which originated from the right ovary, was noted. The left ovary and left fallopian tube were normal. The right fallopian tube and right ovary were excised and sent for pathologic examination for histologic confirmation.
Results
There was no recurrence of the disease ∼14 months later at a follow-up.
Macroscopically, the right ovary and the right fallopian tube measured 8 × 6 cm; the tumor was a well-demarcated mass, 6 × 5 × 4.5 cm, with a wall that measured between 0.6 and 0.8 cm. Sectioning disclosed that the tumor was irregular and contained cystic materials.
In the pathology report, the right tube was seen as normal. The right ovary contained a sex-cord stromal ovary tumor. Immunohistochemically, clear vacuoles of the signet-ring-like cells were negative for cytokeratin. The signet-ring cells showed diffusely positive immunoreactivity for calretinin and inhibine. Her Ki-67 proliferation index was under 1%. The diagnosis of a signet-ring stromal ovary tumor was made after histomorphologic and immunohistochemical examinations were completed (Fig. 2).
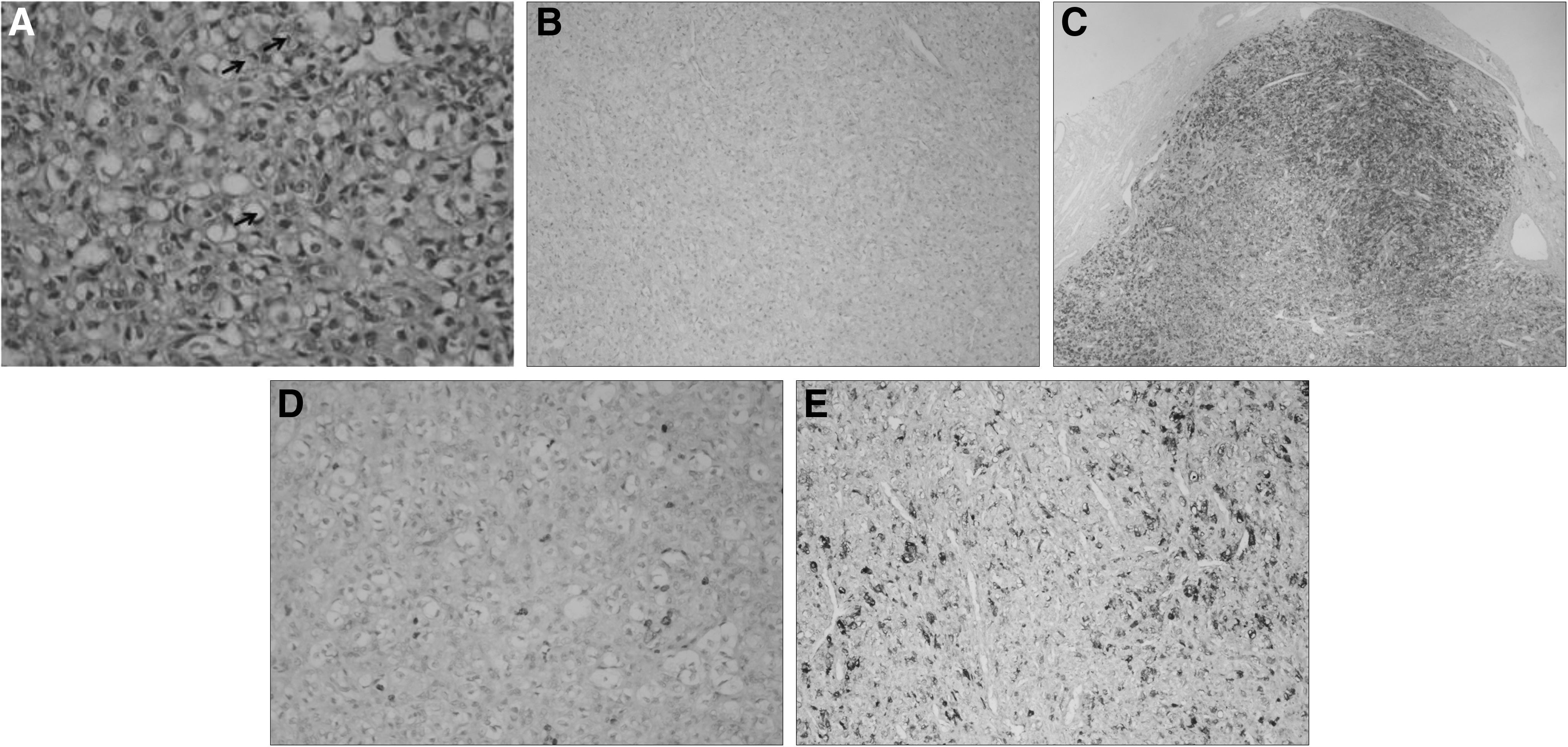
Signet-ring cell stromal tumor of the ovary.
Discussion
The original case was reported by Ramzy in 1976 as a signet-ring stromal tumor, 1 and the term is still used currently. However, in the text, the tumor was referred to as a signet-ring cell stromal tumor just as Roth and Ramzy had reported in 2014. 9 This report described a case of a signet-ring cell stromal tumor of the ovary that was associated with Hodgkin's lymphoma.
A signet ring–like appearance can be found associated with nonneoplastic processes and in a variety of nonadenocarcinomatous neoplasms, such as several varieties of malignant lymphomas, 10 malignant melanomas, 11 meningiomas, 12 and gastrointestinal stromal tumors. 13 However, the relationship between Hodgkin's lymphoma and a signet-ring cell stromal tumor of the ovary is unclear. Perhaps this tumor is related to the Hodgkin's lymphoma's therapy.
The main differential diagnostic disease is a Krukenberg tumor, which is commonly bilateral and nearly always has epithelial components other than signet-ring cells, being positive for different cytokeratins and epithelial membrane antigen, and containing mucin within the vacuoles. 3 If periodic acid Schiff, mucin, and cytokeratins are negative in the signet-ring cell stromal tumor cells, that is strong evidence against a mass being a Krukenberg tumor. 2 The primary characteristic separating a signet-ring cell stromal tumor from the other ovarian sex-cord stromal tumors is the presence of nonmucin/nonlipid signet-ring cells. In addition, Su et al. showed in 2003 that the ultrastructure of the vacuole in the signet-ring–like cells consists of cytoplasmic pseudoinclusions of extracellular edematous matrix. 14 General edema of the cytoplasmic matrix, dilatation of the mitochondria, and invagination of the cell membrane by the extracellular matrix are three possible mechanisms of vacuole formation that were described previously in signet-ring cell stromal tumors by Dickersin et al. in 1995. 15
The difference between a Krukenberg tumor and a signet-ring cell stromal tumor is critical, as a Krukenberg tumor is malignant with an extremely bad prognosis and a signet-ring cell stromal tumor is benign. 16 Krukenberg tumors are bilateral nearly 63% of the time and are often multinodular. On the contrary, all of the previously reported signet-ring cell stromal tumors have been unilateral and uninodular. These two findings have been the only significant distinguishing characteristics for differentiating these tumors, but Forde et al. reported a case multinodular and bilateral signet ring cell stromal tumor of the ovary in 2010. 5 A microcystic stromal tumor of the ovary can include both a signet-ring cell stromal tumor and a Krukenberg tumor. The distinguishing microscopic features are small round–to–oval cystic spaces or a reticular pattern. 17 Some neoplastic cells have intracytoplasmic eosinophilic globules positive with alpha-1-antitrypsin 18 (Table 1).
Modified from Forde et al. 5
PAS, periodic acid–Schiff; CK, cytokeratin.
A signet-ring cell stromal tumor of the ovary may be associated with a Brenner tumor 19 and must be differentiated from other stromal tumors of the ovary, especially a techoma-fibroma. Stromal tumors of the ovary have shown positivity for vimentin, actin, inhibin, and calretinin immunohistochemically. 20 A sclerosing stromal tumor, a luteinized thecoma associated with sclerosing peritonitis, and a microcystic stromal tumor must be considered in the differential diagnosis of a signet-ring cell stromal tumor. All of these tumors are benign conditions of the ovarian stroma. Macroscopically distinguishing a signet-ring cell stromal tumor from the other tumors is very difficult due to their solid or solid and cystic nature and yellow–gray surfaces. Luteinized thecomas have scattered lutein cells and brisk mitotic activity associated with sclerosing peritonitis, both of which are not seen in Signet-ring cell stromal tumors. Signet-ring cell stromal tumors of the ovary have no documented association with sclerosing peritonitis, hormone production, or other syndromes. Signet-ring cell stromal tumors occur especially in adult women, but other sclerosing stromal tumors are identified in young women. 5
There have been 17 cases in the English literature as of this writing until when these studies were examined, the following were found: The mean age was 46.94 ± 23.17 (minimum: 4; maximum: 83) The mean size of the tumors was 6.84 ± 3.03 cm (minimum: 2.5; maximum: 13.0). In studies with available data, the mean follow-up time was 40.2 months (minimum 1; maximum: 208). The majority of these patients presented with abdominal pain and their tumors were localized in the left adnexial region. Unilateral oophorectomy was the most-performed procedure but optimal treatment is not yet established (Table 2).
This case was previously reported by Dickersin et al. 15
Size of ovary.
NI, no information; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; SO, salpingo-oophorectomy; WRLO, wedge resection of left ovary; NED, no evidence of disease.
Conclusions
The association of Hodgkin's lymphoma with signet-ring cell stromal tumor of the ovary was not established prior to the current case. This is the first case after Hodgkin's lymphoma was treated with chemotheraphy, radiotherapy and transplanted autologous bone-marrow stem cell. The current authors believe that signet-ring cell stromal tumor of the ovary might be associated with Hodgkin's lymphoma or chemotherapy, radiotherapy, or transplanted autologous bone-marrow stem cells.
Footnotes
Author Disclosure Statement
All authors declare that there are no conflicts of interest in connection with this article.