
Abstract
Abstract
Background:
Cervical cancer is often a slowly progressing malignancy that presents in women with a mean age of 51. This case is a highly unusual presentation of metastatic squamous cell carcinoma (SCC).
Case:
A 28-year-old healthy, gravida 0, female—who was post a quadrivalent Gardasil® series with normal Papanicolaou smears—presented with abdominal pain, bloating, and postcoital bleeding. A colposcopy was significant for cervical intraepithelial neoplasia III. Cold knife cone was significant for SCC with positive margins. Human papilloma virus (HPV) typing was positive for HPV 31 and 68. Positron emission tomography was negative for metastasis. However, a radical hysterectomy started and then was abandoned due to the discovery of metastases to the sigmoid epiploica.
Results:
Pathology testing revealed that this patient had SCC with metastasis to the sigmoid epiploica and to 2 pelvic lymph nodes. Immunohistochemical staining was positive for p16. She was diagnosed with stage IVA SCC of the cervix and, as of this writing, stated that she intended to undergo radiation therapy followed by chemotherapy.
Conclusions:
When appropriate, a high index of suspicion is necessary to diagnose cervical cancer in low-risk individuals. (J GYNECOL SURG 34:159)
Introduction
W
Squamous cell carcinoma (SCC) comprises 69% of cervical cancers, followed by adenocarcinoma (ADC) at 25% and other at 6%. 14 SCC originates from the ectocervix at the squamocolumar junction. 15 The classic pathologic feature is an eosinophilic keratin pearl located in the center of a nest of malignant cells. These nests can invade the stroma and trigger a lymphocytic response. 15 The 5-year survival rate of SCC is greater than that of ADC at every stage 16 and varies from 85%–90% in stage I disease to 15%–20% in stage IV disease. 17
This article reports a highly unusual presentation of metastatic cervical SCC in a healthy, low-risk female who had a status of post-Gardasil® vaccination series and normal Papanicolaou smears.
Case
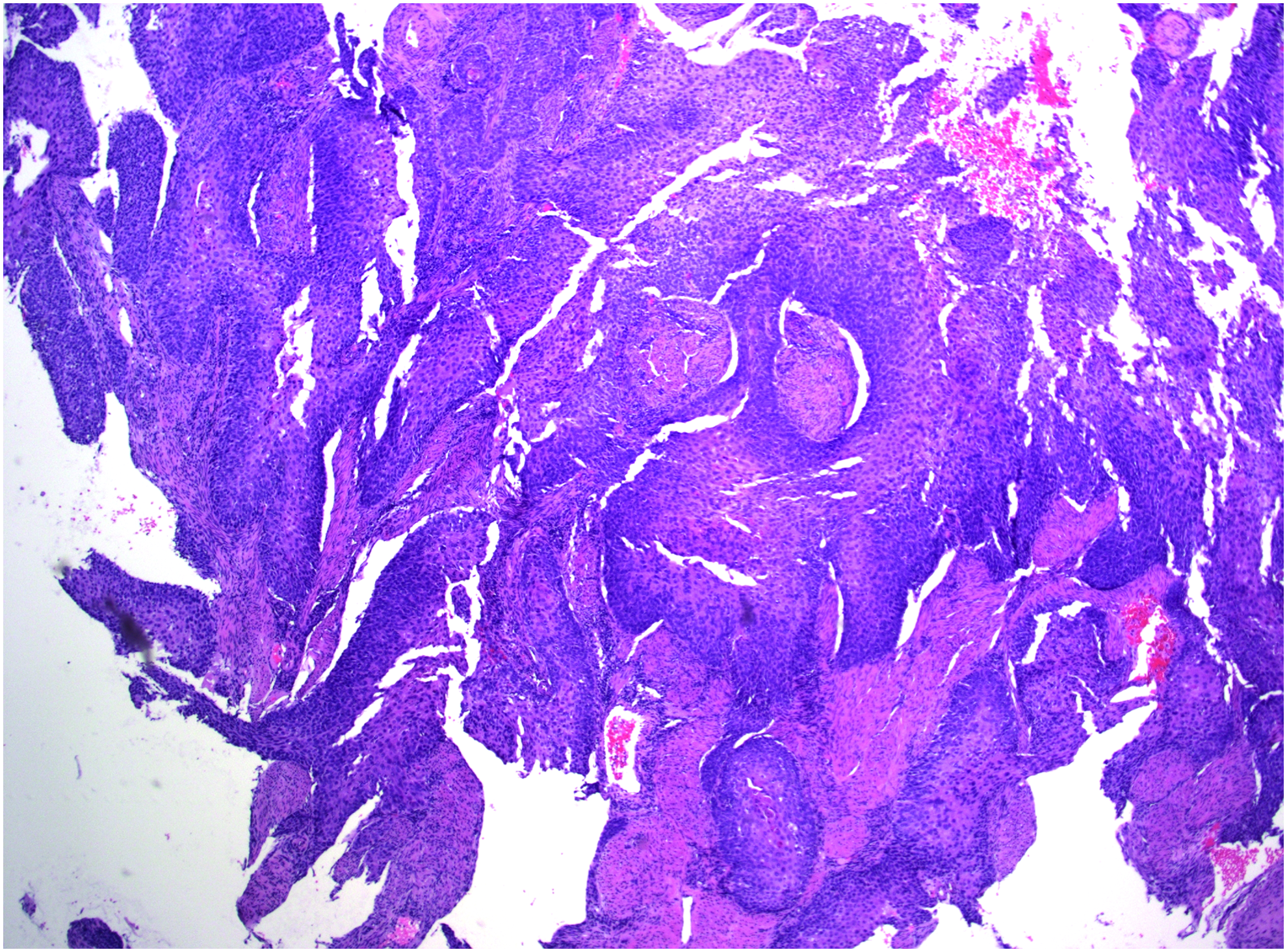
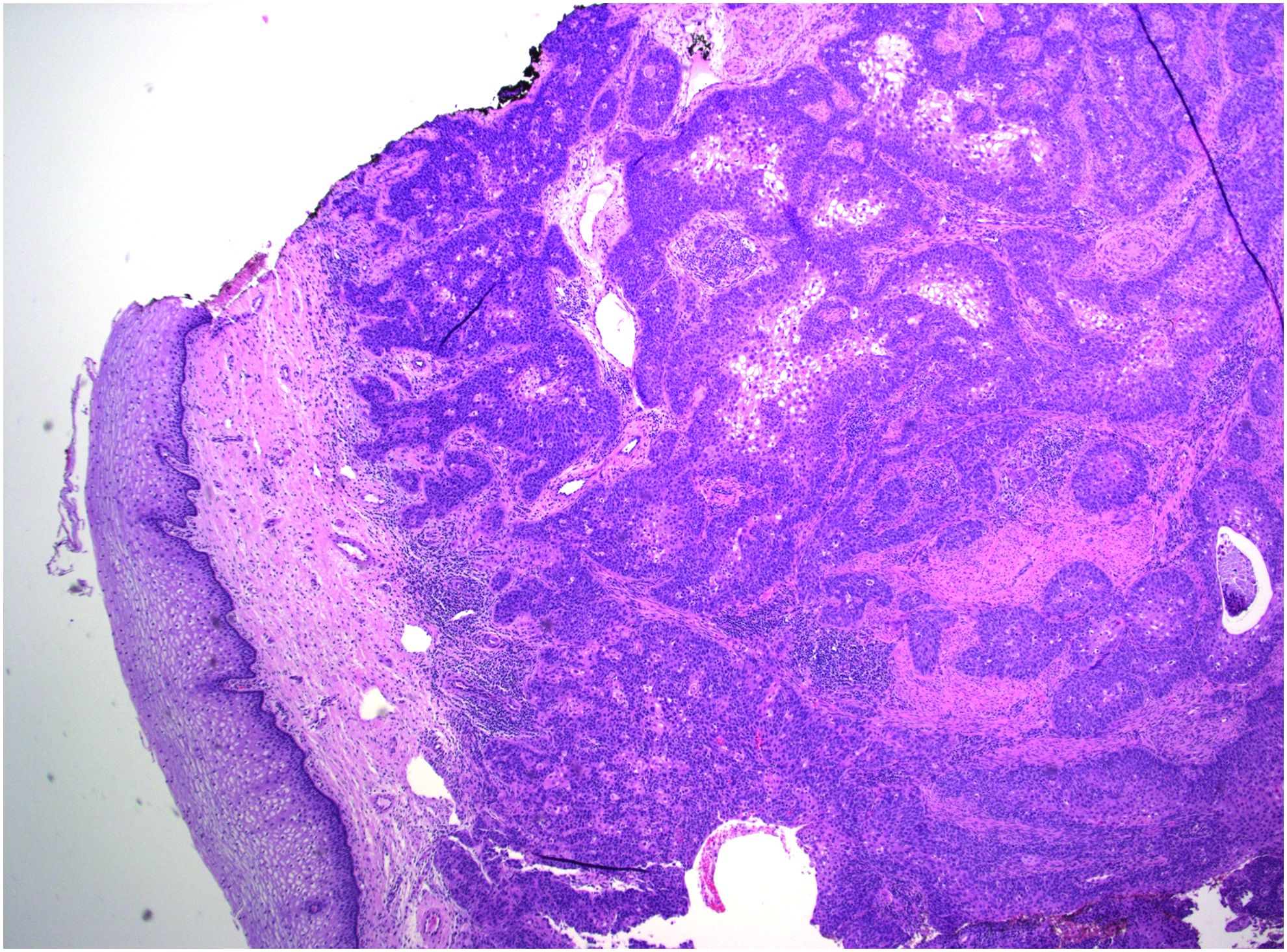
A 28-year-old, healthy, gravida 0 female presented to her gynecologist for abdominal pain and bloating for 3 months and occasional painless postcoital vaginal bleeding for 9 months. This patient had no history of abnormal Papanicolaou smears, and her most recent Papanicolaou smear had been 9 months ago. She had received the quadrivalent Gardasil® series prior to coitarche at age 17 and had more than 10 lifetime sexual partners. She never smoked. Her pelvic examination was unremarkable, and her cervix appeared grossly normal and mobile. Colposcopy was performed to investigate her postcoital bleeding (Fig. 1), and the histology of the specimen was significant for cervical intraepithelial neoplasia III on both cervical biopsy (Fig. 2) and endocervical curetting. A subsequent cold knife cone was significant for SCC with positive margins (Fig. 3).

Colposcopy with acetic acid showing a grossly normal cervix. Color images available online at www.liebertpub.com/gyn
Cervical biopsy showing complex nests of high grade squamous dysplasia suspicious for invasive squamous cell carcinoma. Color images available online at www.liebertpub.com/gyn
Cold knife cone showing squamous cell carcinoma deeply invading cervical stroma with overlying normal ectocervical mucosa. Color images available online at www.liebertpub.com/gyn
A Papanicolaou smear was then performed for HPV typing. It was remarkable for atypical squamous cells of undetermined significance with positive HPV 31 and HPV 68 and negative HPV 16 and HPV 18. A positron emission tomography scan was negative for metastases; thus, this patient was referred to gynecologic oncology and consented to undergo a robotic-assisted radical hysterectomy following egg retrieval. Upon entry of the abdomen, it was noted that the VCare® uterine manipulator had perforated the area immediately inferior to the uterus through an area of soft gray tissue that appeared consistent with cancer (Figs. 4–6). Sigmoid epiploica was adherent to this tissue, and metastatic implants were noted on the epiploica. The hysterectomy was abandoned, and the patient underwent a bilateral salpingectomy and bilateral oophoropexy with the goal of shielding her ovaries from future radiation therapy, and pelvic and para-aortic lymph-node dissection.
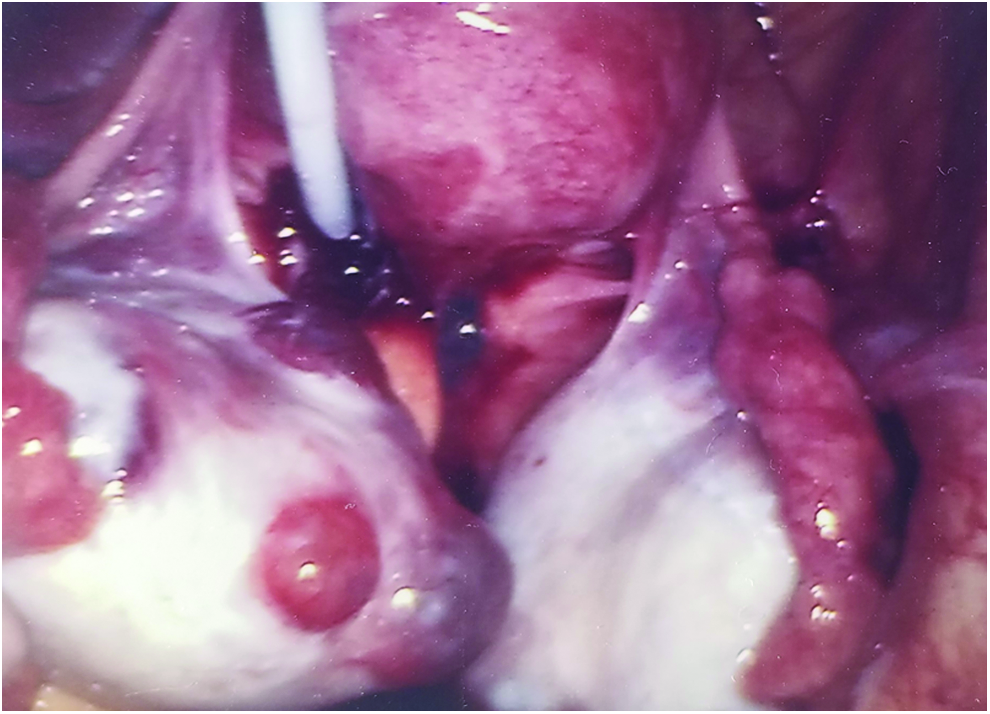
Uterine manipulator perforating immediately inferior to the uterus. Color images available online at www.liebertpub.com/gyn

Uterine manipulator perforating through soft, gray tissue highly suspicious for cancer. Color images available online at www.liebertpub.com/gyn
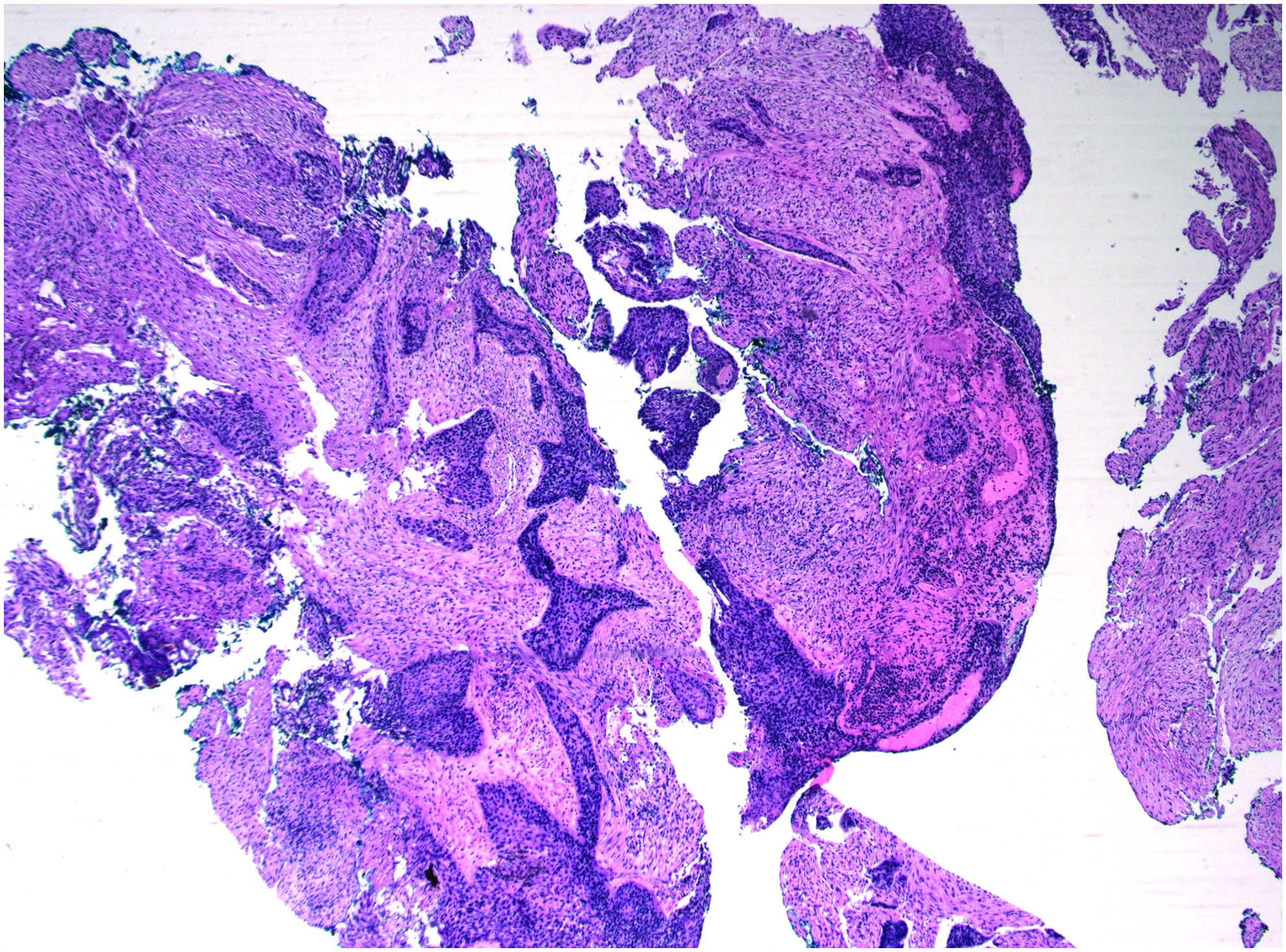
Tissue perforated by uterine manipulator showing inflamed connective tissue with nests of malignant squamous epithelium. Color images available online at www.liebertpub.com/gyn
Results
Pathology testing revealed SCC with metastasis to the sigmoid epiploica and 2 pelvic lymph nodes (Fig. 7). Immunohistochemical staining was positive for p16. The patient was diagnosed with stage IVA SCC of the cervix. As of this writing, the patient stated that she intends to undergo radiation therapy followed by chemotherapy.
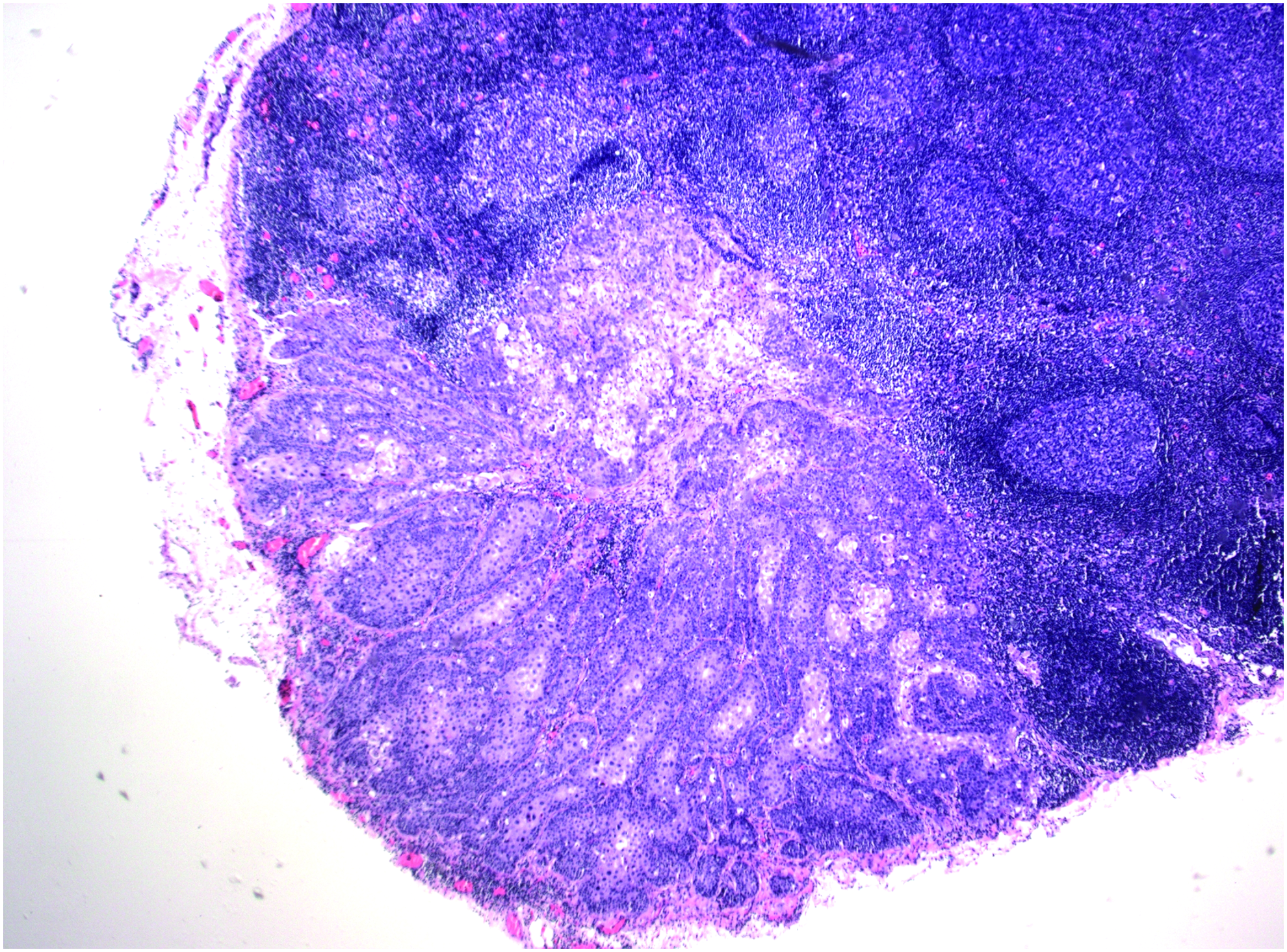
Left pelvic lymph node showing partial replacement by metastatic squamous-cell carcinoma. Color images available online at www.liebertpub.com/gyn
Discussion
This case was a highly unusual presentation of metastatic cervical SCC in a healthy female status post-Gardasil® series with normal Papanicolaou smears. When appropriate, a high index of suspicion is necessary to diagnose cervical cancer in low-risk individuals.
In the above case report, the patient's metastatic cervical SCC was associated with HPV 31 and HPV 68, but interestingly not with HPV 16 or HPV 18. Cervical SCC is most commonly associated with HPV 16 (59% of all cases), HPV 18 (13%), HPV 33 (5%), HPV 45 (5%), and HPV 58 (5%). 18 Both HPV 31 and 68 are considered high-risk genotypes and are phylogenetically related to HPV 16 and 18, respectively. 19 Clifford et al. found that the HPV 16 family, including HPV 31, is significantly more prevalent in SCC than ADC. The HPV 18 family is usually more prevalent in ADC than SCC, but HPV 68 has shown no significant difference in prevalence. 20 Multiple studies have shown that the survival rate of patients with HPV 31–associated cervical cancers was better than the survival rates of patients with HPV 16– and HPV–18 associated cervical cancers.21–23 One study even found HPV 31 to be an independent predictor of improved survival. 24 Not much is known about the prognosis of HPV 68.
As a screening test, the Papanicolaou smear has low sensitivity (57%) and specificity (76%). The test has a positive predictive value (PPV) of 26% and a relatively high negative predictive (NPV) value of 92%. 25 Typically, a negative Papanicolaou smear should be reassuring of normalcy. However, physicians must maintain a high level of suspicion for invasive SCC, because approximately 15% of invasive SCC cases present with normal cytology within 1 year of diagnosis. 26 As demonstrated by the above case report, colposcopy can assist in diagnosis. Colposcopy has a sensitivity, specificity, PPV, and NPV of 92%, 67%, 52%, and 96%, respectively. 25 Given that abnormal cytology and histology are correlated, 25 accuracy increases when Papanicolaou smears and colposcopy are used together to evaluate questionable cervical findings.
In June 2017, the American College of Obstetricians and Gynecologists published a committee opinion on HPV vaccinations that strongly encourages healthcare providers to educate patients about the benefits and safety of HPV vaccination. 27 The U.S. Food and Drug Administration has approved three HPV vaccinations: Cervarix™; Gardasil®; and Gardasil®9. These vaccinations cover two, four, and nine different HPV genotypes, respectively (Table 1). Gardasil®9 covers 9 of the 13 identified cancer-causing HPV genotypes, including HPV 31, and provides >99% efficacy against HPV disease related to genotypes HPV 6, HPV 11, HPV 16, and HPV 18. 28
Disease prevention limited to the associated HPV genotypes.
HPV, human papilloma virus; CIN, cervical intraepithelial neoplasia; AIS, adenocarcinoma in-situ; VIN, vulvar intraepithelial neoplasia; PeIN, penile intraepithelial neoplasia; AIN, anal intraepithelial neoplasia.
Conclusions
While HPV vaccination has drastically reduced the population's incidence of cervical cancer and decreases the individual risk of cervical cancer, physicians should consider cervical cancer as the differential diagnosis of postcoital bleeding in even low-risk patients whose status is post-HPV vaccination.
Footnotes
Acknowledgments
The authors would like to thank the Kapiolani Women's Cancer Center in Honolulu, HI, for their dedication to patient care.
Author Disclosure Statement
The authors have no actual or potential conflicts of interest.