
Abstract
Abstract
Background:
Female genital-tract infection is not uncommon. However, a tubo-ovarian abscess (TOA) secondary to Streptococcus pneumoniae is extremely rare.
Case:
A 46-year-old, para 3, woman presented with a 2-week history of lower abdominal pain and constipation. Assessment showed the presence of a right adnexal mass and free fluid in the pouch of Douglas. Thus, a decision was made to perform a diagnostic laparoscopy, with a working diagnosis of an ovarian cyst accident. Intraoperatively, a right TOA was found and drainage was performed. The pus culture grew out S. pneumoniae.
Results:
Postoperatively, this patient completed a 14-day course of broad-spectrum antibiotics and recovered well. Sexually transmitted infection screenings were nonreactive. She has remained well with no recurrence of S. pneumoniae observed during follow-up.
Conclusions:
This case demonstrated the diagnostic challenges involved in detecting and treating a TOA with S. pneumoniae. Management of such a rare infection was revisited.
Introduction
T
Case
A healthy 46-year-old para 3 with a history of three previous lower-segment cesarean sections presented with severe lower abdominal pain of 2 weeks' duration; the pain was associated with bloating and constipation. She had no symptoms suggestive of a urinary tract infection, nor did she have vomiting, diarrhea, or a fever. There were no gynecologic symptoms, such as a foul-smelling vaginal discharge, abnormal vaginal bleeding, or dysmenorrhea. Upon assessment, she was noted to be comfortable with normal vital signs. She was afebrile. There was tenderness over her right iliac fossa region, but no mass was palpable. A vaginal examination yielded unremarkable results.
However, a full blood count showed a raised white cell count of 22,600/mm3 with 91.8% neutrophils and an elevated level of C-reactive protein at 8.86 mg/dL. This patient's renal profile was normal. Transvaginal ultrasound (TVUS) showed a uterus measuring 8.9 cm × 5.4 cm, with an endometrial thickness of 11 mm. There was a thickened, walled, uniloculated, right ovarian cyst measuring 3.5 × 5.5 cm, without internal echoes. The left ovary measured 3.6 cm × 2.2 cm. Free fluid was noted at the pouch of Douglas. An initial diagnosis of an ovarian cyst accident was made, and this patient was counseled to undergo diagnostic laparoscopy and procedures. Intraoperatively, it was noted that there was a minimal amount of pus and sloughing at the pelvic area with a right TOA (Fig. 1). Approximately 20 cc of pus were drained. There was no perihepatic adhesions. Other structures appeared to be normal. Histopathologic examination of the right cyst wall was consistent with an abscess. A culture of the ovarian tissue grew out Streptococcus pneumoniae (Fig. 2).

Laparoscopic view showed the presence of pus (arrows) and sloughing at the pelvic area with a right tubo-ovarian abscess.
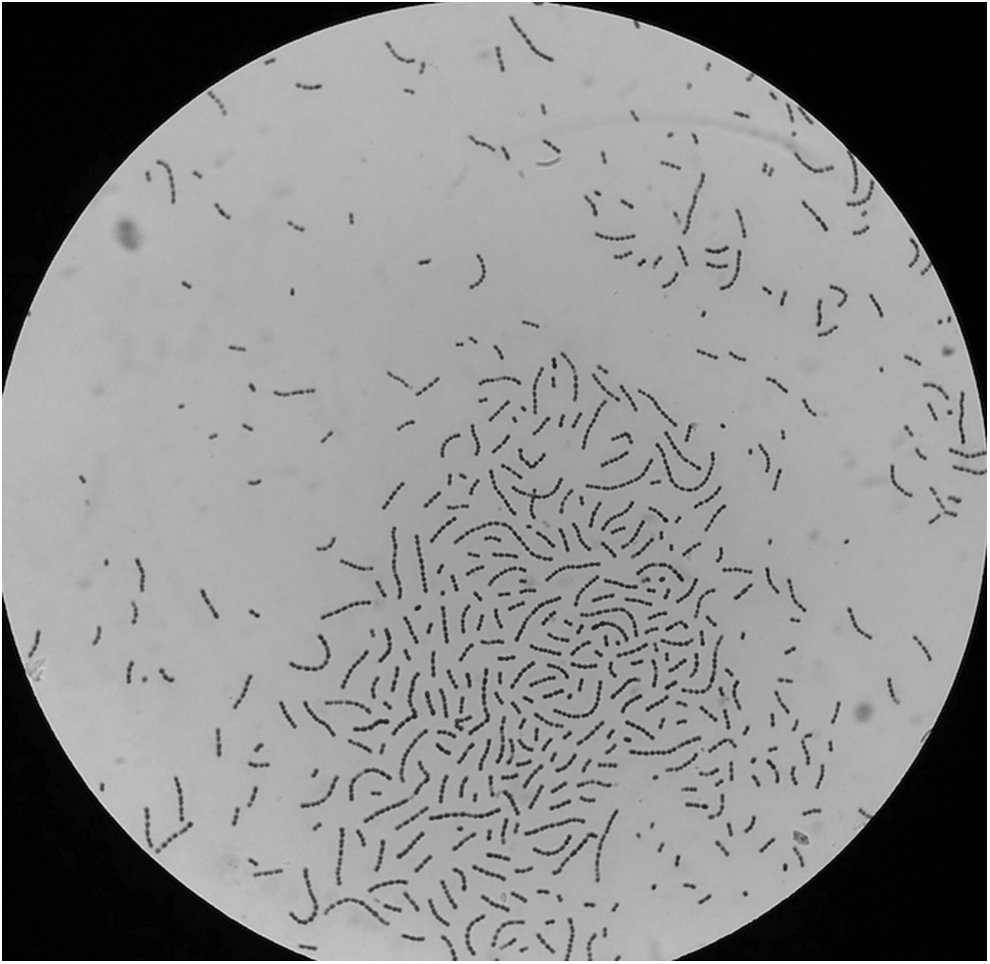
Gram staining under 1000 × magnification shows gram-positive cocci in a chain suggestive of Streptococcus pneumoniae.
Results
Postoperatively, this patient completed a 14-day course of broad-spectrum antibiotics and recovered well. Screenings for sexually transmitted infection were non-reactive. She remained well with no recurrences of TOAs observed during follow-up.
Discussion
Common organisms isolated from vaginal cultures include Escherichia coli, Group B Streptococcus, Enterococcus faecalis, Chlamydia trachomatis, Staphylococcus spp. and Streptococcus spp. (others). 5 However, up to 39.4% of intra-abdominal cultures are negative for any pathogens and, in up to one-third of cases, different bacteria are found in vaginal and intra-abdominal swabs. 5 S. pneumoniae is not considered part of normal commensal bacteria in the female genital tract. Therefore, the mechanism of acquiring such an infection from this unusual pathogen is poorly understood. Transient colonization via an orogenital route from contact with upper respiratory–tract infection is a possible explanation. Once colonized, this organism can result in an ascending infection via the fallopian tubes into the ovarian parenchyma, leading to abscess formation. 6 Risk factors, such as a history of PID, prior antimicrobial therapy within 30 days, use of a copper intrauterine contraceptive device, childbirth, and gynecological surgery, can contribute to such an infection.5–7
The diagnosis of TOA is usually made clinically with the aid of biochemical and radiologic imaging. Patients typically present with lower abdominal pain (98%), with or without fever (50%). Other symptoms include abnormal vaginal discharge (28%), and nausea and vomiting (26%).1,2 C-reactive protein and erythrocyte sedimentation rate (ESR) are statistically significantly higher in a patient with TOA, compared to PID, with a diagnostic ability of 73%—or 87% when using the cutoff values of 11.5 mg/L and 19.5 mm/1/2 hour. 1 Comparatively, the white blood cell count is usually within the normal range. 2
Given that clinical findings and laboratory results are not specific, radiologic imaging is essential in the assessment of patients suspected to have TOA. TVUS commonly shows a complex cystic mass, in the pouch of Douglas or adnexa, with a thick irregular wall, and presence of septation and internal echoes within. Other findings include a unilocular cystic mass and pyosalpinx, which are present in 34% and 21.3% of cases, respectively.2,8 As one-third of TOAs arise from the right side, it is important to differentiate this condition from other pathologies, such as periappendiceal abscesses. 9 The use of computed tomography (CT) scanning increases the diagnostic certainty for TOA by identifying the origin of the abscess. 10 A finding on CT of a right ovarian vein entering the mass has 100% specificity and 94% sensitivity for TOA. Other findings suggestive of TOA include a distended right fallopian tube (79%), the presence of a mass posterior to the mesovarium (76%), contralateral fat stranding (55%), and thickening of the uterosacral ligament (55%). 10
The current patient only had abdominal pain without other symptoms of TOA. Her blood tests and radiologic findings were not typical of TOA. Thus, she was counseled to undergo diagnostic laparoscopy, because there was a suspicion that she had sustained a cyst accident.
Ruling out a malignant neoplasm prior to any intervention is another important aspect in the management of TOA. Wang et al. described the superiority of diffusion-weighted magnetic resonance imaging (MRI) with apparent diffusion coefficient value, compared to conventional MRI in the assessment of a TOA mimicking an ovarian malignancy. 11
Patients with suspected TOAs need hospitalization and close observation. Options of management include administration of a broad-spectrum intravenous (IV) antibiotic and image-guided or surgical drainage of the abscess. Goharkhay et al. reported that, with IV antibiotic alone, up to 42% of patients' conditions did not respond clinically and the patients required further treatment, compared to all patients who underwent ultrasound (US)–guided drainage. Among 21 patients whose conditions had failed to respond to antibiotics, 18 of 19 had successful salvage drainage under US- or CT-guidance, while the remaining patients needed surgical drainage. 12 Another study reviewed 240 patients with pelvic abscesses, whereby 199 of these women received only antibiotics while 41 received additional image-guided drainage; the researchers reported that 16.1% of the women who received antibiotics alone required further surgical intervention, compared to 2.4% of the women in the drainage group. 13 Broad-spectrum antibiotics, such as combinations of cephalosporin, gentamicin, and metronidazole, are frequently used as initial treatments for TOAs. 2
Surgical intervention—either laparoscopy or laparotomy drainage of the abscess—is normally performed in cases of diagnostic uncertainty, as in the current case. 9 Other indications include failed medical therapy or when histopathologic examination of the specimen is needed, especially in cases of suspected malignancy. 9 In a review by Gjelland et al., 6.6% of patients who underwent transvaginal aspirations eventually needed to undergo laparoscopic drainage for persistent pain, residual abscesses, or therapeutic uncertainty. There were no procedure-related complications documented in same review. 9 In cases when surgical drainage is required, the size of the abscess has been found to be larger. 14 Dewitt et al. demonstrated that, for every 1 cm increase in size of an abscess, there was increase in hospitalization by 0.4 days. Abscesses >8 cm were associated with increased complications. 14
A multivariate analysis performed by Kinay et al. showed that factors—including parity >2, fever on admission, and abscess >6.5 cm—were independent predictors for surgical treatment. 8 In the current case, diagnostic laparoscopy was performed due to diagnostic uncertainty. This patient subsequently had surgical drainage followed by antibiotics. She had an uneventful recovery without any complications.
Conclusions
This report demonstrated that clinical presentations of TOA are not always straightforward. In addition to that, unusual pathogens, such as Streptococcus pneumoniae, can be isolated from TOA despite the rarity of this bacterium in TOAs. A high index of suspicion is needed for managing such cases so that early diagnosis and prompt treatment can be initiated to reduce any associated morbidity and mortality.
Footnotes
Acknowledgment
The authors would like to thank the Head of the Department of Obstetrics and Gynaecology for permission to publish this article about the case.
Author Disclosure Statement
No competing financial conflicts of interest exist.