
Abstract
Abstract
Background:
Oncofertility is an emerging field that addresses the fertility and reproductive needs of patients who have cancer.
Case:
A 28-year-old patient with IB1 squamous-cell cervical cancer with pelvic node metastasis underwent laparoscopic ovarian transposition and bilateral pelvic lymph node dissection followed by concurrent chemoradiation.
Results:
At a 6-year follow-up, the cancer had not metastasized or recurred and this patient's ovarian function was well-maintained.
Conclusions:
It is important to transpose and safeguard the ovaries when radiotherapy is planned in early stages of squamous-cell cervical cancer, even with lymph node metastasis. Laparoscopic ovarian transposition is an effective and simple technique for avoiding early menopause and preserving the fertility potential of patients. (J GYNECOL SURG 34:171)
Introduction
A
Surgical treatment such as radical or total hysterectomy, pelvic and para-aortic lymphadenectomy, and adjuvant chemotherapy or pelvic irradiation are utilized—sometimes simultaneously—to fight this vicious disease in an attempt to stop it in its tracks. And although doctors are successful in prolonging disease-free survival if the cancer is caught early, 2 this comes at a cost of female patients' reproductive health and early onset of menopause.
Oncofertility is an emerging field that aims to balance life-preserving treatments with fertility-preserving options. The American Society of Clinical Oncology recommends offering ovarian transposition prior to pelvic radiotherapy as an option for optimizing fertility preservation in patients with this cancer. 3
Ovarian transposition—or oophoropexy or ovariopexy—for patients undergoing pelvic irradiation as a part of cancer treatment was described as early as 1958, when it was performed by way of laparotomy. 4 As endoscopy revolutionized the management of most diseases, ovarian transposition was performed increasingly by the laparoscopic route. Recently, a robotic approach has also been shown to be equally effective. 5
Here, this article describes 6 years of successful management and follow-up in the case of a 28-year-old patient with invasive squamous-cell cervical carcinoma with lymph node metastasis, who underwent ovarian transposition before concomitant chemoradiation.
Case
An unmarried, 28-year-old, Taiwanese patient, gravida 2, para 0, with two abortions, presented with International Federation of Gynecology and Obstetrics (FIGO) IB1 squamous-cell cervical carcinoma that was confirmed with a colposcopy-directed cervical biopsy performed for a 3-cm nodule over her anterior cervical lip. Magnetic resolution imaging confirmed the presence of a 3.1 × 2.9 × 2.8–cm, hyperintense cervical mass on the anterior cervical lip and a 1.6 × 1.5 × 1.57–cm enlarged lymph node in the left external iliac region, which was suspicious for metastasis.
This patient's baseline squamous-cell carcinoma (SCC) antigen concentration was 1.8 ng/mL (normal: <1.5 ng/mL) and her carcinoembryonic antigen (CEA) concentration was 1.2 ng/mL (normal: <5 ng/mL).
The patient underwent laparoscopic, bilateral, pelvic lymph node dissection and bilateral ovarian transposition. A primary optical trocar was inserted at the Lee–Huang point (midway between the subxiphoid and umbilicus) to enable higher positioning of her ovaries. 6 Three 5-mm ports were inserted, and the upper lateral ports were at least 3 cm above the level of the umbilicus; thus, marking the site of transposition. Given that the left external iliac lymph node was enlarged, necrotic, and suspicious for malignancy, the lymph node was retrieved with an endobag and sent for frozen section, which revealed metastatic SCC. A bilateral pelvic lymphadenectomy was completed.
For ovarian transposition, first a bilateral salpingectomy was performed. The infundibulopelvic ligaments and ovaries were then mobilized to enable tension-free transposition and to maintain the blood supply. Both ovaries were sutured to the anterolateral abdominal wall, near the level of the upper lateral ports, with extracorporeal sutures using 1-0 polypropylene. Radio-opaque hemoclips were applied near the ovaries for identification during radiation therapy.
Results
Postsurgery, this patient was given her first dose of gonadotropin-releasing hormone (GnRH) agonist (a 3.75-mg depot formulation) and 2 additional doses were given at 4-weekly intervals.
Concurrent chemoradiation was planned as her lymph node status was positive. Twenty-eight cycles of weekly external-beam radiation therapy of 5040 cGy/cycle and 3 cycles of weekly 430-cGy intracavitary brachytherapy to point A were given. Concurrently, 6 cycles of cisplatin (40 mg/m2/week) were administered.
This patient's serum tumor markers at 6 months postsurgery were SCC 1.5 ng/mL and CEA 0.77 ng/mL. These markers remained well within normal range at serial 6-monthly intervals. As of this writing, her last report at her 6-year follow-up was SCC 1.3 ng/mL and CEA 1.1 ng/mL.
Three months after radiotherapy was completed, a serum hormonal assay was performed (follicle stimulating hormone [FSH], 71.8 mIU/mL; and estradiol, 42.8 pg/mL). Serum concentrations 7 months postradiotherapy were FSH, 6.4 mIU/mL; and estradiol 469 pg/mL. Similar values were maintained at yearly measurements. The last reports at a 6-year follow-up were FSH 3.7, mIU/mL; and estradiol, 223.2 pg/mL. She did not complain of any menopausal symptoms, such as hot flushes, at any point of time.
A computed tomography scan 2 years after surgery showed no evidence of tumor recurrence or ovarian metastasis (Fig. 1) Ultrasound scanning showed a normal ovarian size and a good number of antral follicles. Regular Papanicolaou smear results were normal.
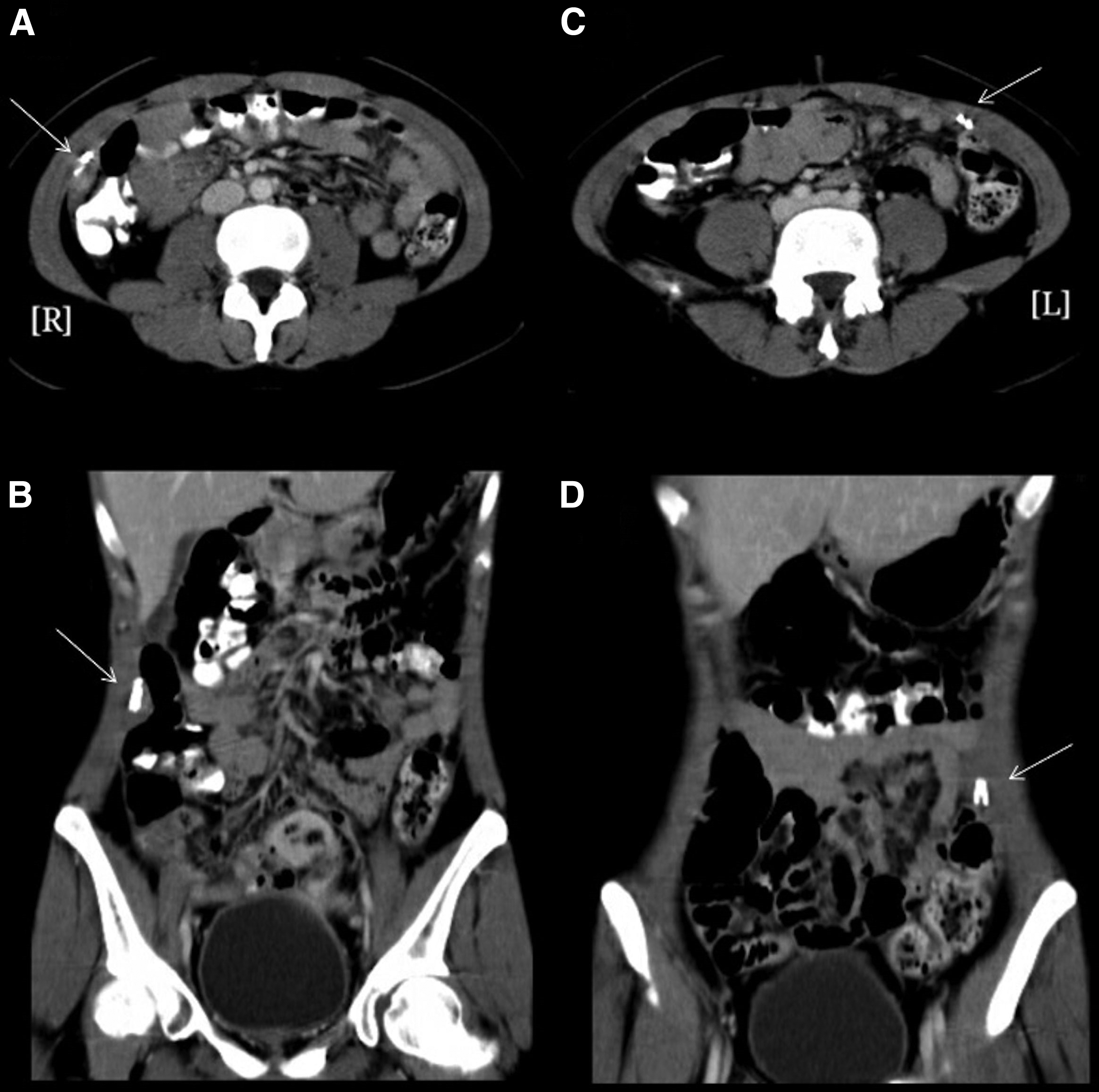
Computed tomography scan 2 years after transposition showing right (
In view of her good ovarian function but no resumption of menstrual activity, the patient was advised to consider surrogacy.
Discussion
Maturing oocytes in the ovaries are highly sensitive to radiation, in a dose-dependent manner. A radiation dose >8 Gray (Gy) causes permanent ovarian damage in patients older than 40, and doses >20 Gy cause permanent sterility. When compared with the high doses used in radiotherapy for cervical cancer, ranging from 45 Gy to 90 Gy, the importance of safeguarding the ovaries is apparent. Transposing the ovaries out of the field of radiation reduces the exposure to 1%–10% of the total radiation dose. 7
Cervical cancer is not a hormonally dependent cancer, nor is there a high risk of ovarian metastasis. 8 Landoni et al. reported that independent risk factors for ovarian metastasis were tumor histology (2.4% for nonsquamous and 0.5% for squamous histology), size of the tumor, invasion of cervical stroma, and lymphovascular space invasion; lymph node metastasis was not found to be an independent risk factor. 8 Moreover, concurrent chemoradiation has shown to be highly effective in such cases. Thus, in early cases, along with fertility-preserving surgery (radical hysterectomy or trachelectomy), ovarian transposition should also be performed when postoperative radiotherapy is anticipated.
Even after successful transposition, transient ovarian failure might occur, possibly caused by devascularization at surgery, scatter radiation,9,10 or gonadotoxic chemotherapeutic agents. Ovarian function has been reported to resume spontaneously when the chemoradiation insult is over, possibly due to dormant follicles resuming their maturation cycles. 10 GnRH agonist was given to the current patient to suppress her ovaries and cause less damage, as the dividing follicles are more sensitive to radiation. She was menopausal for a period of 6–8 months (FSH 71.8 mIU/mL; estradiol, 42.8 pg/mL), after which her ovarian function returned to normal (FSH 6.4 mIU/mL; estradiol 469 pg/mL) and was maintained since that time.
Pelvic irradiation reduces uterine volume, impairs uterine distensibility due to myometrial fibrosis, causes endometrial injury and uterine vascular damage, 11 and could have been responsible for the current patient's amenorrhea. She was advised to consider surrogacy, as patients with irradiated uteri are at an increased risk for pregnancy-related complications, such as spontaneous miscarriage, placental abnormalities, low birth weight, and preterm birth. 11 Steigrad et al. reported a case wherein the transposed ovaries recovered from transient failure and a successful twin pregnancy was conceived in a surrogate mother. 10
Conclusions
The current case was unique, as ovarian transposition was performed although she had FIGO IB1 SCC with pelvic node metastasis. Most of the existing studies involved patients with early stage cervical cancer, without lymph node metastasis, undergoing ovarian transposition. However, it is the current authors' firm belief that positive lymph nodes in early stages should not be a deterrent to ovarian preservation methods. With the growing success of chemoradiation treatments for early stage cervical cancers, and 5-year survival rates of ∼80%, these patients go on to live disease-free lives for many years. 2 Laparoscopic ovarian transposition is an effective and simple technique to save these patients from the further morbidity of early menopause and to preserve their fertility potential.
Footnotes
Acknowledgments
The current authors thank the Asia Pacific Association of Gynecologic Endoscopy and Minimally Invasive Therapy for providing International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital for Dr. Ankita Jain.
Author Disclosure Statement
All authors declare that there are no conflicts of interest related to this article.