
Abstract
Abstract
Background:
A huge ovarian cyst can be seen in a patient, due to rapid progression of its growth or late presentation. In benign cases, this poses a dilemma, especially in adolescents. Should a surgeon proceed conventionally with laparotomy or take a more appealing laparoscopic approach? This article presents a case of a huge ovarian cyst in an adolescent that was removed successfully via laparoscopic cystectomy, using a Cystofix® balloon catheter as a drainage tool.
Case:
A 19-year-old Indian girl, with no known medical illnesses, presented with a huge abdominal swelling. Systematic examinations were unremarkable. Imaging, including a computed tomography scan, showed a homogenous ovarian cyst with no malignant features; all of this patient's biochemical tumor markers were within normal values. Therefore, a laparoscopic cystectomy with a possible oophorectomy was planned. Initial cystic decompression was performed with a Cystofix balloon puncture set and this procedure was followed by a laparoscopic cystectomy in usual manner.
Results:
The laparoscopic operation was uneventful and use of the Cystofix balloon facilitated the decompression without causing any spillage of the cysts content. The operation lasted 75 minutes with minimal blood loss in the patient. The patient recovered well and her cyst was benign.
Conclusions:
With good patient selection and proper preoperative evaluation of the nature of an ovarian cyst, even an enormous ovarian cyst can be removed by laparoscopy using this method, especially in a young patient. (J GYNECOL SURG 34:167)
Introduction
O

Cystofix® suprapubic catheter.
Case
A 19-year-old single Indian adolescent, with no known medical illness and no malignancy profile, presented in January 2017 with progressive abdominal distension that had begun 3 weeks prior. This swelling was associated with vague abdominal discomfort, a reduced appetite, and constipation. There was no loss of weight, nor urinary symptoms or heavy menstrual flows. The rest of this patient's history was unremarkable. She had no previous surgical history. She began her menarche at age 10 with a subsequently regular cycle.
Her height was 155 cm and her weight was 78 kg making her body mass index 32.5, which is overweight. She was afebrile (36.8°C), and her vital signs were stable with normotensive blood pressure (127/88 mm Hg) and no tachycardia (88 beats/minute). She was pink, had no jaundice, and her thyroid and breasts were normal. There was no edema in her lower limbs and no lymphadenopathy. Tanner staging was appropriate to her age. Her abdomen was distended with a palpable mass corresponding to 36-week uterine size. The mass had a sizeable irregular border with ill-defined margins, was cystic in consistency, extended from the epigastrium to pubic area, was not tender, and made dull note on percussion. It was not possible to rule out the presence of ascites clinically. There were no abnormal vessels or bowel sounds. No abnormalities of her external genitalia were noted.
Bedside ultrasonography was performed, showing a cystic ovarian mass measuring 25 cm × 16 cm with no evidence of ascites, and there was a solid area, septation, a substantial area, and papillary projections. The uterus was of average size with a thin endometrial thickness noted. Biochemical evaluations including tumor markers—such as CA-125, CA 19.9 and α-fetoprotein—were all in healthy ranges. Further evaluation with a computed tomography (CT) scan of her abdomen/pelvis showed a similar finding of a cystic, well-defined ovarian mass measuring 15 cm × 21.6 cm × 25.6 cm (Fig. 2) This suggested a possible ovarian cystadenoma with no evidence of metastasis and lymphadenopathy. Therefore, she was counseled to undergo laparoscopic cystectomy, possible oophorectomy, and conversion to laparotomy if needed.
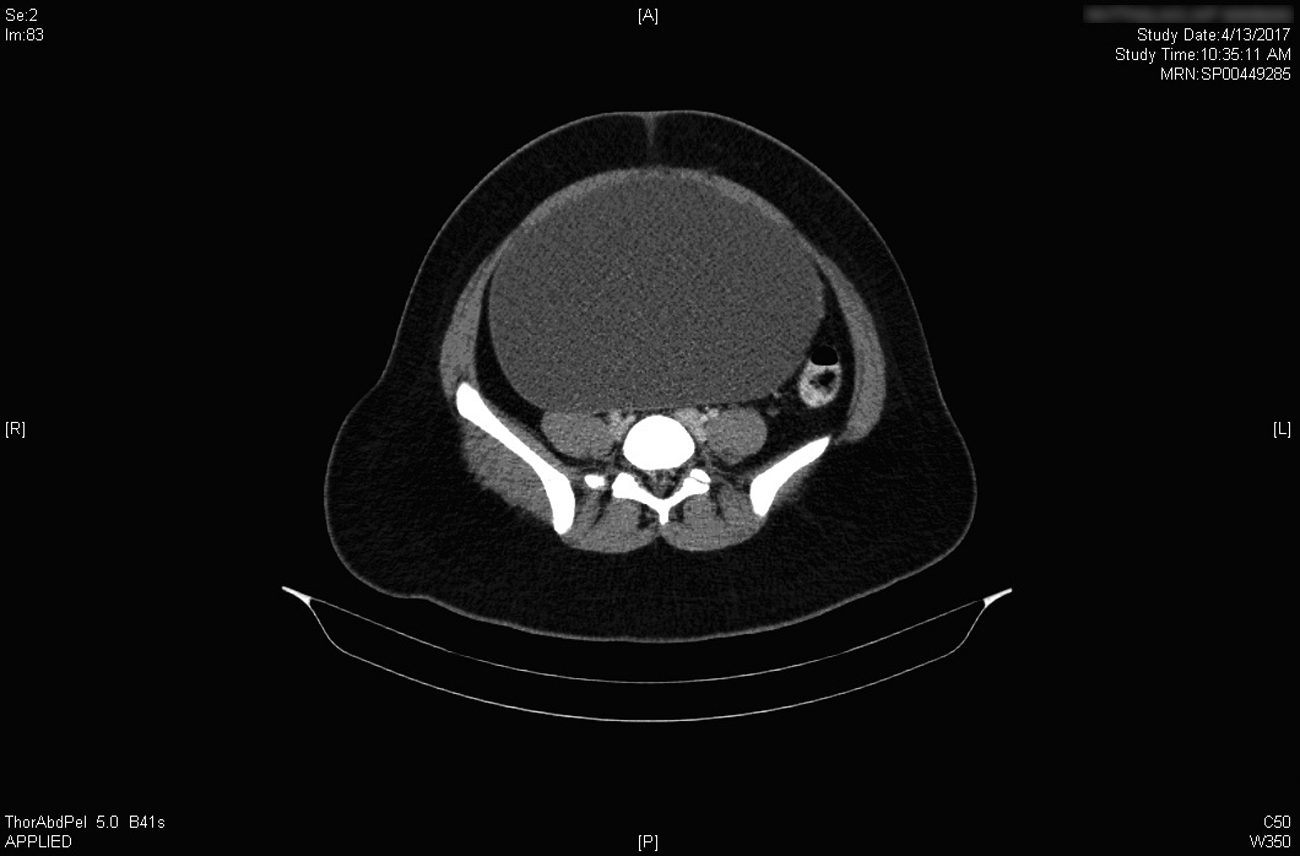
Computed tomography scan of the abdomen.
During the procedure, the patient was clean and draped, and her bladder was emptied in the usual manner. The procedure started with a “direct stab” incision made at the suprapubic area to decompress the cyst content using a size 14F Cystofix cannula (Fig. 3). Once content was observed, the catheter was introduced further to empty the content; a total of 5 L of serous fluid was drained. After that, the entry to peritoneum was performed in the usual manner. The first trocar (size 5 mm) was placed just above the umbilical area, and the abdominal cavity was visualized.

Decompression procedure.
The colossal cyst was seen arising from the left ovary, while the right ovary was normal. The liver surface was unremarkable. A cytology specimen was prepared, using a peritoneal wash. The second trocar (size 10 mm) was introduced at the right iliac fossa area. Following that, a laparoscopic cystectomy was performed in a usual manner as the cyst was already empty and easy to manipulate in a sterile bag to ensure no spillage from any potential remnant cyst content via the 10-mm trocar (Fig. 4). With this method, the left ovary was reconstructed, using two interrupted sutures with Vicryl
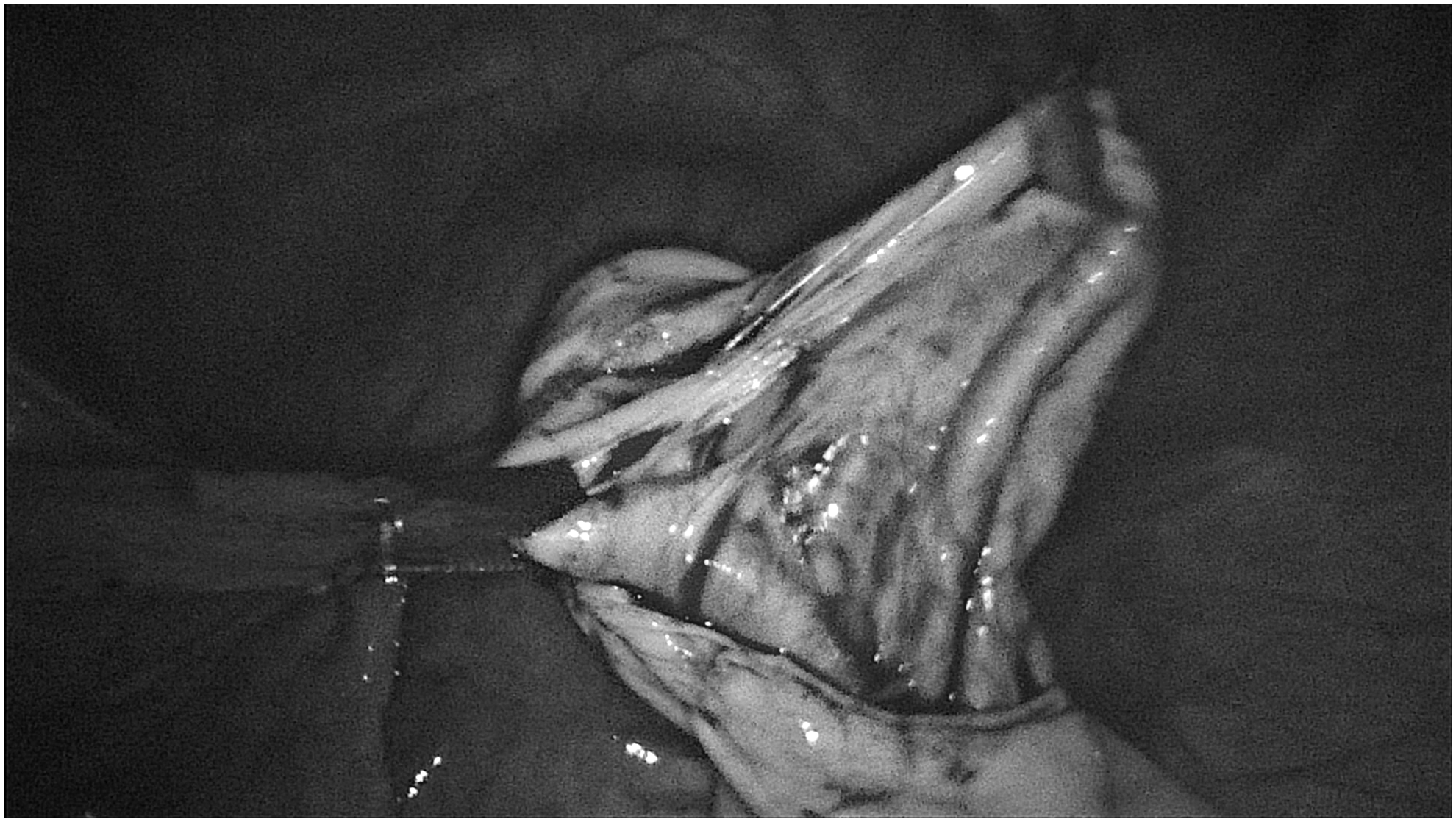
Ovarian cyst post-decompression.
Results
This patient's postoperative period was uneventful. She was well and discharged on day 2 after the surgery. She recovered well as noted at a 6-week postoperative follow-up. Histopathologic testing revealed that the cyst was a benign mucinous cystadenoma with negative cytology. This indicated that her surgery was a complete treatment.
Discussion
The majority of ovarian cysts are small, asymptomatic, and found incidentally by today's advanced ultrasound technology. The most frequent subtypes are endometriomas or simple cysts. Among large cysts, most are cystadenomas comprised 75% serous and 25% mucinous contents. This subtype is rarely malignant in origin. 3 However, there are limitations to detecting small solid—and potentially malignant components—with imaging of a massive ovarian cyst. CT is a good way to supplement evidence in these cases. 4 A large cyst was reported before from extreme of 148.6 kg in 1922 by Spohn et al. 5 to 72 kg by Zamora-Garza et al. in 19926; with the latest being 11 kg by Baradwan et al. in 2017. 1
In addition to size, the value of tumor markers in such cases is limited because of their potential inaccuracy. Therefore, clinical information and antigen testing results require careful interpretation to determine the severity of the mass. 7 A previously reported case highlighted the importance of decompression and manipulating technique for preventing spillage of cystic mass content, such as paracentesis or direct trocar puncture during the laparoscopic procedure. 4
In the current case, a suprapubic urinary catheter was used. This Cystofix balloon punction set includes a suprapubic catheter applied in cases of acute urinary retention. The device is comprised of a stainless-steel cannula and a silicone integral balloon catheter with a lumen at the tip of the catheter. The device drains urine and provides an inflatable balloon proximal to the lumen, which prevents slippage of the catheter. The other part of the catheter is then connected to the container bag. The Cystofix offers the advantage of removing cyst contents without causing any spillage, as this device works by using a universal connector that establishes a closed system to prevent any backflow and possible spillage. It also has three “wings” for better gripping of the cannula and easy handling. However, there is still a small possibility of spillage, which might raise the cancer stage if a case turns to be malignant, and, rarely, might cause a pseudomyxoma peritonei with an estimated incidence of 1–2 of 1,000,000 cases. Therefore, a careful selection of patients for which this catheter is to be used is paramount.2,4,6
Currently, there is no consensus regarding maximal size for a laparoscopic procedure, as it depends on the experience and skill of a surgeon and also on local department policy. Otherwise, a laparoscopic approach is considered to be the “gold standard” for the surgical management of benign ovarian cysts, as this approach enables a shorter hospital stay, less postoperative pain, a smaller surgical scar, and early recovery, compared to the laparotomy approach.2,6 In the current case, as the initial assessment showed that the cyst was benign in origin, a laparoscopic approach with decompression of the cyst content was highly possible and achievable to avoid a midline laparotomy incision, which is conventionally made for surgical management of a substantial ovarian cyst.
Conclusions
In a good patient selection and proper preoperative evaluation of the nature of an ovarian cyst, sizeable ovarian cyst can still be removed by laparoscopic approach using this method, especially in a young patient.
Footnotes
Acknowledgment
The authors would like to extend gratitude to the patient discussed in this report.
Author Disclosure Statement
The authors declare that there are no conflicts of interest and no financial interests connected to this report.