
Abstract
Abstract
Objective:
The aim of this research was to assess the microbiologic diversity and the adequacy of empirical antibiotic treatment of surgical site infections (SSIs) following cesarean sections (CS) and abdominal gynecologic operations.
Materials and Methods:
A retrospective single-center study was conducted between January 2011 and December 2014. Medical records of all patients with positive SSI cultures following CS or laparotomies for gynecologic indications were reviewed. The adequacy of empirical antibiotic treatment was assessed with antibiotic susceptibility testing results of the isolated pathogens.
Results:
The empirical drugs of choice were a first-generation cephalosporin and amoxicillin–clavulanic acid. Of the 178 positive cultures 99 (55.8%) were obtained from 72 post-CS patients and 79 (44.2%) from 49 post-gynecologic operation patients. The most common pathogens in both groups were enterobacteriaceae, with notable variance in the rate of Staphylococcus aureus between the groups (30.3% versus 6.3%, respectively). In up to 55% of the patients in both groups (62.5% of post-CS patients and 44.8% of post-gynecologic operation patients), inadequate empirical antibiotic treatment was administered.
Conclusions:
Variance in post-CS and post-gynecologic procedure SSIs may render the current uniform empirical antibiotic treatment suboptimal. Assessment of local flora and resistance patterns should dictate tailor-made protocols for both SSI groups.
Introduction
S
Risk factors for SSI have been studied extensively and include advanced age; high body mass index; immunocompromised states; anemia; and associated comorbidities, such as malignancies, diabetes, and prior hospitalizations.3–5 Recognition of nonmodifiable risk factors as well as management of modifiable risk factors can assist in reducing SSI.6,7
The widespread implementation of various antibiotic prophylaxis protocols along with the use of aseptic techniques, such as abdominal and vaginal scrub preparations,8,9 have significantly reduced infection rates and associated postoperative morbidity.10–12 Nonetheless, SSI post abdominal surgery affect up to 5% of patients and remains the second most common complication of gynecologic surgical procedures and the most common cause of nosocomial infections. 13 Given that patient populations and procedures differ greatly between obstetric and gynecologic disciplines, commonly used generic antibiotic protocols might compromise the quality of treatment that patients receive.
The aim of this study was to assess the microbiologic diversity and the adequacy of empirical antibiotic treatment for SSIs in both obstetric and gynecologic operations.
Materials and Methods
Study design
A retrospective study was conducted in a single tertiary medical center with annual cesarean section (CS (and abdominal gynecologic operation rates of ∼2800 and 1500 surgeries, respectively. Comprehensive electronic medical records were reviewed, obtaining all cases of positive cultures from SSIs, as defined by Centers for Disease Control and Prevention (CDC) criteria, 14 following CS or laparotomies for various gynecologic indications (hysterectomies, open conservative myomectomies, and explorative laparotomies (between January 2011 and December 2014. Culture results were compared to empirical antibiotic treatments and treatment adequacy was determined according to pathogen susceptibility testing; a treatment was deemed adequate if the eventual cultured pathogen was susceptible to the antibiotic regimen.
Study population
Patients included in the analysis were those presenting with positive SSI cultures according to CDC criteria for SSI 14 during the patients' initial hospitalizations, or patients who were readmitted to the emergency department due to SSI within 30 days of surgery. Bacterial identification and antibiotic susceptibility test results from clinical specimens were performed at a local microbiology laboratory using the Vitek® 2 system (bioMerieux, St. Louis, MO), according to Clinical and Laboratory Standards Institute criteria. Isolates that were considered to be contaminants were excluded from the analysis.
Operating room conditions and antibiotic protocols
All operations were performed in the same operating suites with identical sanitary conditions. Incisions were made after uniform abdominal scrubbing, using alcohol-chlorhexidine solution (0.5% chlorhexidine–gluconate in 70% isopropyl alcohol). During the 4-year study period, the current authors' antibiotic prophylactic protocol was consistent; it included cefazolin, a first-generation cephalosporin, as the single drug of choice (excluding cases of allergies). One g of intravenous (IV) cefazolin was administered 30 minutes prior to the skin incision in both CS and abdominal gynecologic surgeries.
15
Both inpatient and outpatient empirical SSI treatment included either a first-generation cephalosporin or amoxicillin–clavulanic acid (Augmentin
Data collection
Data included patients' demographics and relevant medical histories, such as previous hospitalizations (>3 days in the 6 months preceding the operation), chronic illnesses, and known risk factors for infection (diabetes, obesity, immunocompromised states, and smoking). Microbiologic data included identification and antibiotic susceptibility testing of isolated pathogens. In cases of prolonged and complicated hospitalizations, only the first significant isolate was included in order to exclude secondary nosocomial acquisitions. Identical isolates were regarded as one isolate and were counted once.
The study was approved by the local institutional review board.
Statistical analysis
Statistical analyses were performed using SPSS 22.0 statistical software (SPSS, Chicago, IL). Descriptive statistics are expressed as mean, standard deviation (SD), and minimum and maximum values. Student's t-test was used for parametric variables that are normally distributed. Fisher's exact test was used for small samples of categorical variables. All tests were two-sided, and p-values of <0.05 were considered to be significant.
Results
During the 4-year study period, 16,165 women underwent abdominal operations in the Department of Obstetrics and Gynecology of Lis Maternity Hospital, Tel-Aviv Medical Center, in Tel-Aviv, Israel.
Of these patients, 10,127 women (62.6%) underwent CS and 6038 women (37.3%) underwent abdominal gynecologic operations. Of all clinically suspected SSIs, 323 incision site wound cultures were positive for bacteria. A total of 144 cultures were excluded due to presumably nonpathogenic microorganisms, such as coagulase-negative staphylococci (apart from Staphylococcus lugdonensis), viridans-group streptococci, and diphtheroids. Of the remaining 178 isolates, 99 (55.8%) cultures were obtained from 72 post-CS patients (59.5% of all SSI cases) and 79 (44.2%) cultures were obtained from 49 post-gynecologic operation patients (40.5% of all SSI cases). Regarding pathogens isolated in more than one culture, there were the following: in 22 cases 2 pathogens were isolated; in 11 cases, 3 pathogens were isolated; and, in 4 cases, 4 pathogens were isolated. The rates of scheduled and nonscheduled (urgent and emergent) CS in the hospital's maternity center were comparable during the study period (5056 scheduled CS and 5091 nonscheduled CS). Positive culture SSI rates were significantly higher in nonscheduled patients than in scheduled patients (67 pathogens from 48 patients and 32 pathogens from 27 patients, respectively; p = 0.0002).
Clinical and microbiologic characteristics
Patient and surgery characteristics of SSIs in patients who were post-CS and post-gynecologic operations are presented in Table 1. Most of the patients with culture-positive SSIs (69.4%; n = 84) were affected by at least one of the following: hypertension; diabetes; immunocompromised state; or recent hospitalization.
Immunocompromised state—malignancy, severe neutropenia, or prolonged steroid use.
Prior hospitalization—up to 6 months prior to SSI for at least 3 days.
Data are presented as mean (SD) or n (%) where appropriate.
SSI surgical site infections; SD, standard deviation; NOS not otherwise specified; nr, non-relevant.
Microbial profiles (after omitting contaminants as aforementioned) are depicted in Figure 1 (A and B). Enterobacteriaceae were the most common pathogens in both groups of patients followed by Staphylococcus aureus. The rate of S. aureus was sixfold higher in the post-CS group versus in the post-gynecologic operation group (30.3% [n = 30] versus 6.3% [n = 8]; p = 0.0001). Rates of enterococci, Pseudomonas aeruginosa, and streptococci also differed significantly between the groups.
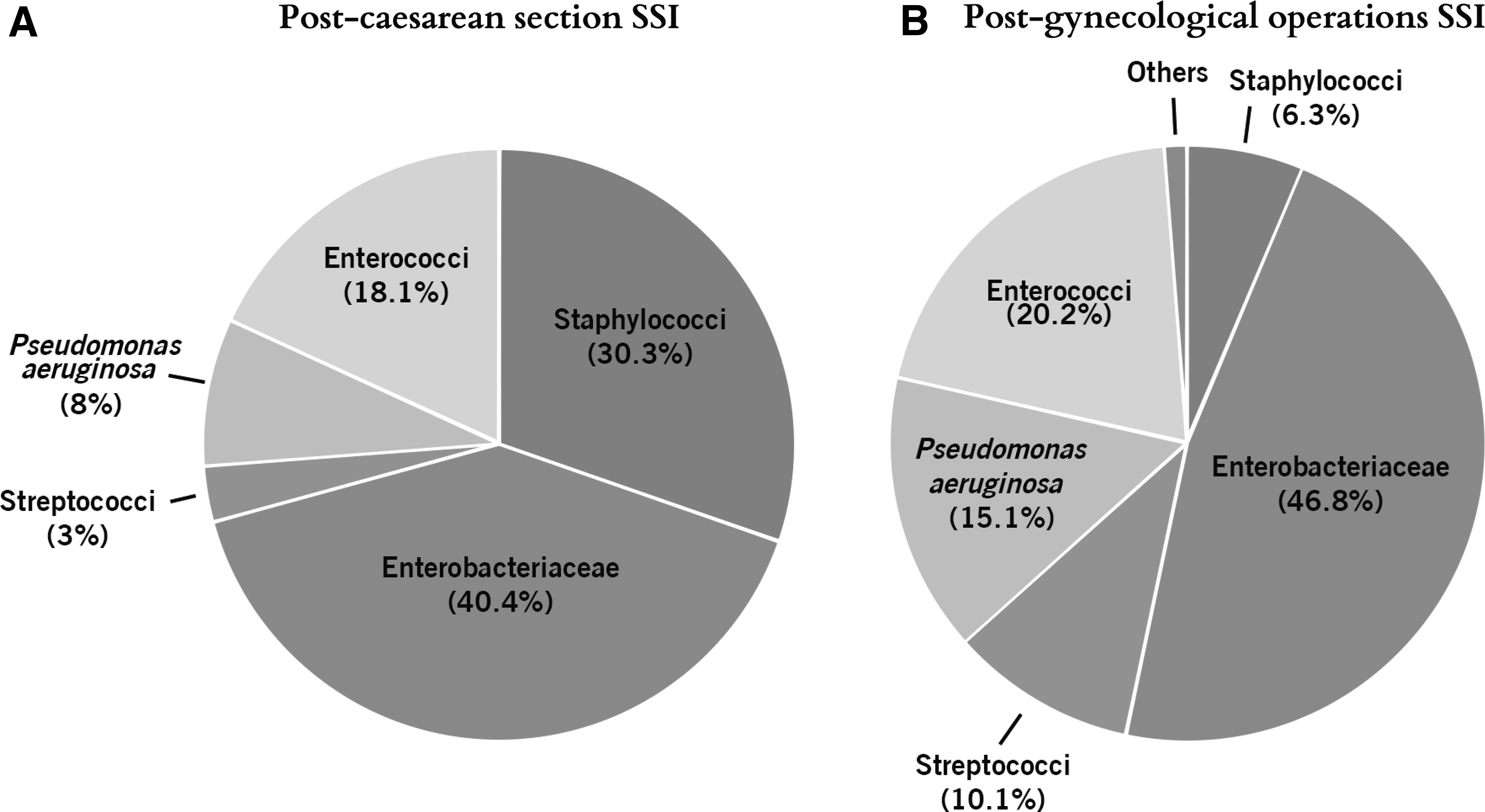
Microbial diversity of bacterial pathogenic flora isolated from surgical site infections following caesarean sections
Adequacy of treatment
The most commonly prescribed empirical antibiotic treatment for SSI was amoxicillin–clavulanic acid that was administered in 66 patients, followed by a first-generation cephalosporin that was administered in 55 patients. Only 55.3% (n = 67) patients received adequate empirical treatment—62.5% (45 of 72 patients) following CS SSIs and 44.8% (22 of 49 patients) following gynecologic operation-SSIs. Among the pathogens resistant to the empirical treatment administered, enterobacteriaceae were the most common, with a resistance rate of 50% (n = 38). Within this group, 50.6% (n = 40) isolates were resistant to first- and second-generation cephalosporins, and 10.1% (n = 8) isolates were resistant to a third-generation cephalosporin. Thirteen isolates (16.4%) were amoxicillin–clavulanic acid–resistant, and 12.6% (n = 10) isolates were aminoglycoside-resistant. P. aeruginosa was the second most common nonsusceptible pathogen cultured, with an inherent resistance to common empirical regimens. Of the S. aureus isolates, 13.1% (n = 5) were methicillin-resistant (MRSA); within this group 5.7% (n = 2) isolates were clindamycin-resistant and all were trimethoprim/sulfamethoxazole-susceptible. Among the enterococci 2 isolates were Vancomycin®-resistant.
Patients receiving adequate empirical treatment were hospitalized for an average of 7.1 days, compared to 9.6 days of hospitalization in patients with isolates that were resistant to empirical treatment (p = 0.05) and 14.3 days in patients with MRSA or extended-spectrum ß-lactamase–producing enterobacteriaceae (ESBL-PE) (p = 0.0001). The rate of SSIs requiring surgical debridement was 17.3% (n = 21); yet, debridement did not correlate with inadequacy of empirical treatment. Nonetheless, the debridement rate in cases of MRSA/ESBL-PE was twice as high, compared to methicillin-sensitive S. aureus (MSSA). Patients with prior hospitalizations had a significantly greater likelihood to have pathogen-resistant strains, compared to patients with no prior hospitalizations (n = 17 [63%] versus n = 35 [37%], respectively; p = 0.01; data not shown).
In an attempt to assess the presumed adequacy of other empirical antibiotic protocols, several empirical antimicrobial regimens were compared with the antibiograms of all SSI isolates (Fig. 2). A first-generation cephalosporin was compared to amoxicillin–clavulanic acid and to a combination of a first-generation cephalosporin and gentamicin. Compared to treatment with a first-generation cephalosporin alone, its combination with gentamicin potentially yielded significantly better antimicrobial coverage for both post-CS and post-gynecologic operation SSIs (odds ratio [OR] = 2.1; confidence interval [CI]: 1.08–4.19, and OR = 3; CI: 1.31–6.93, respectively). Likewise, amoxicillin–clavulanic acid potentially yielded significantly better antimicrobial coverage than a first-generation cephalosporin alone for post-CS but not for post-gynecologic operation SSIs (OR = 2; CI: 1.01–3.9). Adequacy rates of a first-generation cephalosporin and gentamicin were comparable to those for amoxicillin–clavulanic acid in both post-CS and post-gynecologic operation SSIs.
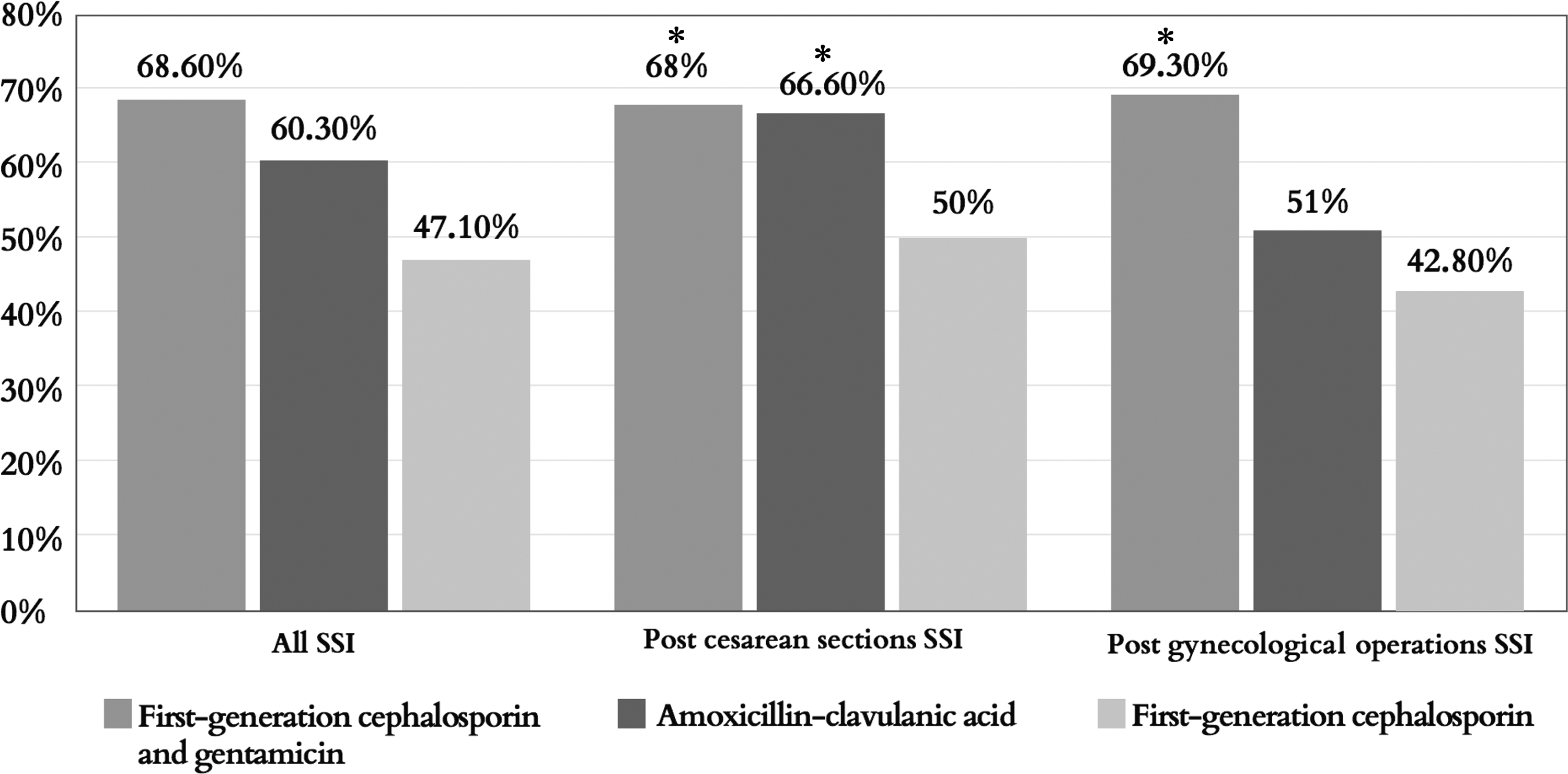
Three putative empirical antibiotic protocols were analyzed according to the antibiograms of all isolated pathogens, simulating the potential adequacy rates if the protocol had been universally prescribed to the various groups of patients. SSI, surgical site infection. *Significantly superior antimicrobial coverage, compared to a first-generation cephalosporin only.
Discussion
SSIs are devastating and often preventable complications of surgical procedures. Understanding causative agents, risk factors, and adequacy of empirical antibiotic treatments are essential for SSI prevention and improved outcomes. The purpose of the current study was to assess the microbiologic diversity and the adequacy of empirical antibiotic treatments for SSIs in both obstetric and gynecologic operations.
In order to deliver high-quality, accurate microbiologic data, the study focused on culture-positive SSIs, caused by true pathogenic bacteria, and distinguished between 2 populations that are currently treated similarly: (1) post-CS patients and (2) post-gynecologic operation patients. Not surprisingly, according to the results, post-CS women were younger and had fewer comorbidities. Nonetheless, hospitalization rates due to suspected SSIs were high in both groups (75%–84%), with hospitalization lengths of ∼7–8 days, regardless of the initial operations.
Pathogenic flora isolated from CS wounds differed from the pathogenic flora isolated from gynecologic surgical wounds—an observation not easily explained in light of identical operating conditions, sanitary protocols and prophylaxis, and shared medical staff. The different rates of staphylococcal-related SSI—30.3% in CS patients versus 6.3% in gynecologic operation patients—were most striking. This significant difference might be explained by pregnancy-related factors altering the skin microenvironment, rendering it favorable to certain bacteria.16,17 Previous studies have shown that S. aureus vaginal colonization and infections increase during pregnancy and postpartum as well as in neonates. 18 Another explanation might be related to the efficacy of prophylactic antibiotics. The hospital's institutional prophylactic protocol was universal during the study period and included a single IV dose of 1 g of a first-generation cephalosporin, given 30 minutes prior to skin incision. Such a protocol most likely provides therapeutic blood and tissue drug levels (that are higher than the bacterial minimal inhibitory concentration [MIC]) during the operation in an average, nonobese nonpregnant patient. However researchers in 2015 questioned if a 1-g dose sufficed in pregnant women. 19
Enterobacteriaceae were the most frequently detected pathogens isolated from SSIs in all patients in the current study. Anatomical considerations and hygiene-related factors in both patient groups could contribute to a greater abundance of these bacteria in superficial and deep tissues within the surgical field or to their frequent migration to this area postoperatively. The high rates of fecal/vaginal flora (i.e., enterobacteriaceae and enterococci) require preventive approaches that may include changing preoperative skin antisepsis, tailored prophylactic regimens, rigorous vaginal decontamination, and improved wound care protocols. 9
The adequacy of empirical antibiotic treatment is critical to the outcome of SSIs. The rate of pathogen susceptibility to empirical antibiotic treatment in the current study was 55.3% (n = 67), with patients following gynecologic operations having significantly higher rates of resistant pathogens. This could be attributed to population-related factors, such as comorbidities, and procedural factors, such as vaginal flora spillage. The 2 common empirical agents given in the current authors' hospital were a first-generation cephalosporin and amoxicillin–clavulanic acid; the latter showed superior coverage, particularly for gram-negative bacteria. In search for a better institutional empirical protocol, the potential efficacy of a first-generation cephalosporin combined with gentamicin was analyzed as an alternative regimen. Such a protocol would have provided significantly higher susceptibility rates following both CS and gynecologic operations due to superior coverage of enterobacteriaceae and P. aeruginosa. 20
For post-CS patients, amoxicillin–clavulanic acid would also provide significantly better coverage than a first-generation cephalosporin, while maintaining the benefit of parenteral and enteral formulations as well as breastfeeding compatibility. 20
The current study had several limitations. First, as a retrospective single-center study, it might not represent the case-mixes and flora of other institutions and regions, thus, limiting generalizability of the current study's results. Second, due to local laboratory practices, anaerobic bacteria, that—according to published data contribute to obstetric and gynecologic SSIs—are not routinely cultured from swabs. This, in turn, might lead to underestimation of the efficacy of amoxicillin–clavulanic acid. Finally, interventions—such as surgical debridement and topical antibiotics—that can change the characteristics of SSIs were not accounted for in the analyses.
Conclusions
The current study emphasizes that, due to the variance in pathogens causing SSI post-CS and post-gynecologic operations, the current uniform empirical antibiotic treatment is unsatisfactory. Future studies are needed to assess local microbiologic characteristics of SSIs and dictate the appropriate empirical treatment accordingly.
Footnotes
Author Disclosure Statement
All authors report no commercial associations nor any conflicts of interest in connection with this article.