
Abstract
Abstract
Background:
The levonorgestrel-releasing–intrauterine system (LNG-IUS) is a frequently used method of contraception worldwide. A rare, but bothersome complication of the LNG-IUS is a perforation of the uterus after insertion. Knowledge about the preferred management option in case of an intra-abdominally situated LNG-IUS during pregnancy is lacking.
Case:
This case report concerns a 33-year-old patient who became pregnant despite having an intra-abdominally situated LNG-IUS. The patient was counseled about the management options. The advantages and disadvantages of expectant management versus laparoscopic removal of the LNG-IUS were discussed, and the patient preferred removal of the IUS. The procedure was performed laparoscopically at 15 weeks of pregnancy.
Results:
The IUS was removed without complications, and the patient's pregnancy proceeded uneventfully.
Conclusions:
Considering the degree of evidence, it is important to make a tailor-made decision in case of a pregnancy with a perforated LNG-IUS. (J GYNECOL SURG 34:164)
Introduction
T
Case
A 33-year-old woman, gravida 3, para 2, visited the gynecology department because she became pregnant despite having a LNG-IUS. The LNG-IUS was inserted 2 years prior. A transvaginal ultrasound (TVUS) after the insertion showed the IUS positioned low in the uterus; thus, the IUS was placed higher in the uterus with grasping forceps, after which the TVUS showed a correct position of the LNG-IUS.
Two years later, during the visit in the gynecology department a TVUS showed a viable intrauterine gravidity of 7 weeks and 6 days. The LNG-IUS was visualized outside the uterus, which was confirmed by an abdominal X-ray (Fig. 1).

Abdominal X-ray showing the intra-abdominally located intrauterine system.
The patient was counseled about the management options. The advantages and disadvantages of expectant management versus laparoscopic removal of the LNG-IUS were discussed, and the patient preferred removal of the LNG-IUS. The removal was performed laparoscopically at 15 weeks of pregnancy.
Results
The LNG-IUS was found in an epiploic appendix of the colon (Fig. 2) and was removed without complications. The patient's pregnancy proceeded uneventfully, and at 40 + 4 weeks of gestation, she delivered a healthy male infant.
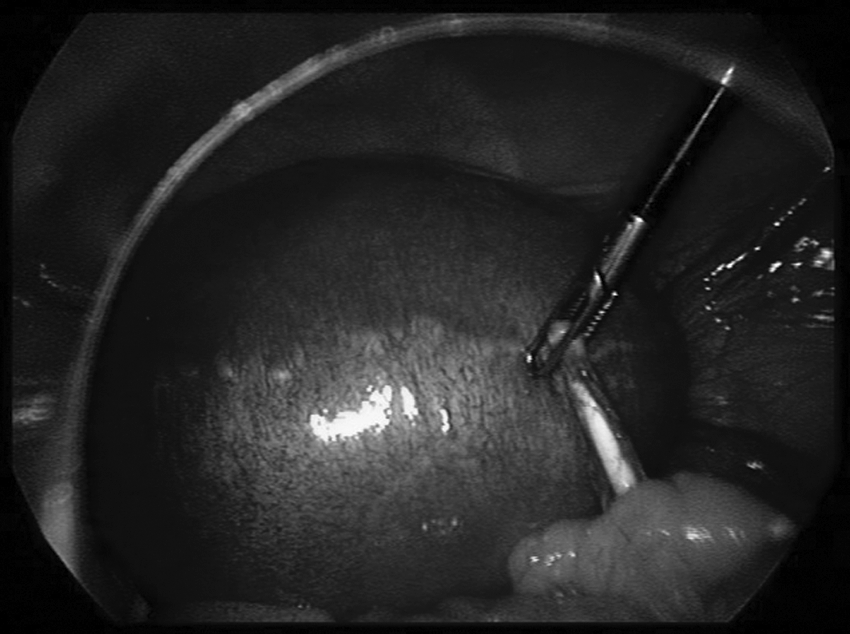
Intraoperative image of the intrauterine system embedded in an epiploic appendix of the colon.
Discussion
In this current case, the insertion of the LNG-IUS was not performed correctly. In the prescribing information of the LNG- IUS it is noted that a displaced LNG-IUS should be removed. A new system can be inserted directly afterward. 2 Instead, the displaced LNG-IUS was relocated in the patient's uterus with a grasping forceps, resulting in perforation of her uterus.
The best management option in case of a perforating LNG-IUS with a viable intrauterine pregnancy is not clear. It is important to take into account possible mechanical as well as hormonal complications in case the LNG-IUS is left in-situ. The occurrence of a mechanical complication is rare, but bothersome as the LNG-IUS can cause organ damage and abdominal adhesions.4,5 Hormonal complications might occur due to the continuous release of levonorgestrel, which results in constant levonorgestrel exposure to the fetus. In one case report, the plasma level of levonorgestrel in a patient with an extrauterine LNG-IUS was about ten times higher, compared to an intrauterine LNG-IUS due to the great absorptive capacity of the peritoneum. 7 This plasma level is similar to levels released by an oral contraceptive pill. 6
However, studies that investigated the use of oral contraceptive pills and levonorgestrel emergency contraception during pregnancy have concluded that there is no increased risk of virilization of the female fetus and other congenital anomalies.8–11 As incidence is low, limited literature is available considering the effect of an extrauterine LNG-IUS on fetal development. In the literature, there were 4 cases of pregnancy with a perforating LNG-IUS.12–15 In 3 cases, the LNG-IUS was left in-situ, and, in 1 case, it had been removed. All 4 pregnancies resulted in the deliveries of healthy infants.
In the Manufacturer and User Facility Device Experience Database (MAUDE), there were no reported cases of extrauterine LNG-IUS during pregnancy. 16 Based upon the available evidence, expectant management is justified. However, removal of the LNG-IUS could prevent mechanical complications associated with an intra-abdominal LNG-IUS. In case a patient opts for laparoscopic removal of the LNG-IUS, it is important to counsel that patient about possible complications of the laparoscopy, including low birth weight, growth restriction, and premature delivery.17–19 In general, the complication rate appears to be small, 20 and laparoscopic surgery is accepted as a safe procedure during pregnancy, with a preference for performing this procedure during the second trimester.
Conclusions
It is of great importance to prevent a perforation of the uterus by an LNG-IUS and to remove a displaced LNG-IUS instead of relocating the system. Considering the degree of evidence, it is important to make a tailor-made decision in case of a pregnancy with a perforating LNG-IUS. To contribute to better insight on the effect of an extrauterine LNG-IUS during pregnancy, it is advisable to improve registration and to report prospective complications in national and international databases.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.