
Abstract
Abstract
Background:
Isolated tubal torsion in pregnant women is a rare diagnosis often treated with laparotomy.
Case:
A 37-year-old woman at 25 weeks of gestation presented with severe lower abdominal pain and vomiting. Ultrasound revealed a 6-cm ovarian cyst. She was taken to the operating room for a diagnostic laparoscopy.
Results:
She was found to have an isolated tubal torsion. The tube was detorted and treated with a salpingectomy. Her postoperative course, the remainder of her pregnancy, and her delivery were uncomplicated. No adverse pregnancy outcomes were associated with the laparoscopic management of her isolated tubal torsion in pregnancy.
Conclusions:
Laparoscopic management of adnexal pathology in pregnancy should be considered in view of the benefits of laparoscopy, including decreased postoperative pain, shorter hospital stay, quicker recovery, and improved cosmesis. (J GYNECOL SURG 34:174)
Introduction
T
Case
A 37-year-old Asian woman, gravida 1, para 0, was referred to the obstetrics division of the Department of Obstetrics and Gynaecology at St. Michael's Hospital in Toronto, Ontario, Canada, for routine antenatal care. Her previous medical history was unremarkable aside from a family history of two atrial septal defects in other family members. Her antenatal course was uncomplicated, with negative multiple marker screening and normal anatomy seen on ultrasound (US) and fetal echocardiography.
The patient presented to the hospital at 24 weeks and 5 days of gestation with diffuse lower abdominal pain and cramping. She also described having fever, chills, and nausea. She was not experiencing any signs of labor and her fetus was active. On assessment, she was afebrile; her nonstress test was normal; and her cervix was long, closed, and posterior. A urine dip was positive for ketones and negative for nitrites and leukocytes. Her white blood cell (WBC) count was mildly elevated at 12 with a neutrophil count of 11, which was felt to be consistent with pregnancy-induced leukocytosis. A midstream urine culture was ordered. She was admitted to the hospital for hydration and pain medications. Within 24 hours, her pain had resolved and she was discharged with instructions to return if she had worsening abdominal pain or further symptoms.
The following day, she returned to hospital at 25 weeks of gestation. Again, she described a constant, sharp, left lower-abdominal pain that was associated with nausea and vomiting and decreased oral intake. Acetaminophen was ineffective for controlling her pain. She had no fetal concerns or signs of labor. She was afebrile with a normal nonstress test result; and her cervix was long, closed, and posterior. Her WBC count was 9 with a neutrophil count of 7. She was admitted to the hospital and an US was arranged to rule out any gastrointestinal or genitourinary causes.
The US, performed at 25 weeks and 1 day of gestation, revealed a single live fetus measuring 25 weeks and 5 days and a left-sided, thin-walled anechoic, unilocular cystic structure measuring 6.7 × 4.6 cm. It was close to the anterior abdominal wall, showing probe tenderness. No internal debris or solid components were identified. Although no ovarian tissue was identified, this was felt to represent a simple ovarian cyst (Fig. 1). The rest of her abdomen appeared normal.
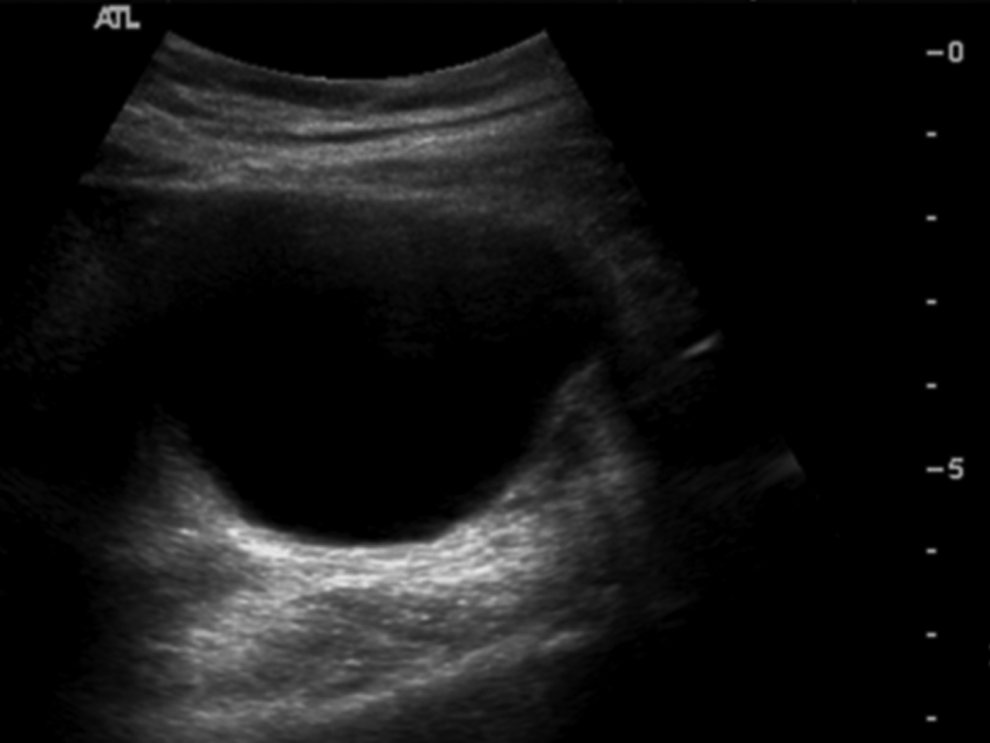
Transabdominal ultrasound image shows a left-sided, fluid-filled thin-walled structure with posterior acoustic enhancement that shows the features of a simple cyst.
The patient's pain resolved somewhat and she was monitored expectantly in the hospital. After several discussions with the patient and her husband regarding the options of expectant management versus surgical management, the couple felt more comfortable choosing surgery and she was consented for a diagnostic laparoscopy, ovarian detorsion, a possible oophorectomy, a possible cystectomy, and a possible laparotomy.
The patient was brought to the operating room 2 days post admission at 25 weeks and 2 days of gestation. A wedge was used to place her in a left lateral decubitus position, and a nasogastric tube was inserted to empty her stomach. The bladder was emptied and no instruments were introduced into the patient's vagina. Pneumoperitoneum was established using Palmer's point. Carbon dioxide (CO2) gas was instilled to a pressure of 15 mm Hg. A 5-mm trocar was inserted using a closed technique at the Palmer's point.
An isolated left tubal torsion was visualized where the fallopian tube had torted two-and-a-half times and appeared to be grossly enlarged (measuring 6 × 4 cm) and cyanotic (Fig. 2). Two 5-mm accessory ports were placed under direct visualization in the midline just below the xiphisternum and another was placed in the right midclavicular line below the costal margin. The laparoscope was used in the midline port for the remainder of the surgery with a CO2 pressure of 12 mm Hg. The other pelvic organs were inspected; the ovaries were normal bilaterally as was the right fallopian tube. The left fallopian tube was detorted, followed by a left salpingectomy. The areas of the tube most affected were the fimbriated and infundibular portions. The specimen was removed using an endobag in the left accessory port. At the conclusion of the surgery, indomethacin was given for 24 hours for prophylactic tocolysis.

At laparoscopy, it was noted that the tube was torted two-and-a-half times.
Results
Postoperatively the patient did well with no complications. She was discharged on postoperative day 1 with a follow-up arranged in the obstetrics clinic. Gross pathologic examination revealed a fallopian tube with an attached paratubal cyst. The fallopian tube measured 3.8 cm in length—including the fimbriated end—and was 1 cm in diameter. The entire fallopian tube was hemorrhagic, and its lumen was filled with blood clots. The findings were consistent with a history of torsion. A paratubal cyst measured 4.5 × 4 × 2 cm with a smooth inner lining. The rest of the patient's pregnancy was unremarkable. She went on to have a spontaneous vaginal delivery at 40 weeks and 5 days with no complications.
Discussion
Isolated tubal torsion is a rare diagnosis that is difficult to identify preoperatively. 4 Initial presentation can include severe lower-abdominal pain and gastrointestinal symptoms in addition to peritoneal signs, fever, tachycardia, and leucocytosis.2,4,5 Ultrasonography generally reveals an adnexal mass on the ipsilateral side of the abdominal pain,2,5 as was the case in the current patient. In addition, color Doppler imaging is helpful for detecting the presence or absence of arterial flow to the adnexa, but this flow is sometimes present because venous flow interruptions often precede arterial ones and are not detected by Doppler ultrasonography. The exact etiology of tubal torsion is not known but might be related to pelvic congestion and local edema that induces torsion. 4 Risk factors for isolated tubal torsion include paratubal cysts, hematosalpinx, hydrosalpinx, or pregnancy.2,4
The differential diagnosis of fallopian tube torsion in pregnancy includes both obstetric and nonobstetric causes, including placental abruption, uterine rupture, appendicitis, adnexal torsion, degenerating fibroids, ureteral or renal colic, or bowel obstruction. 5 In addition, the signs or symptoms of tubal torsion could be masked by either term or preterm labor. 5 Early diagnosis of torsion enables prevention of adnexal loss and possibly compromised fertility. 6 Late or missed diagnosis could lead to potentially fatal thrombophlebitis or death. 2 The only method to diagnose tubal torsion reliably is surgery.2,6 Laparoscopy can be performed initially, followed by laparoscopic treatment or treatment with laparotomy. 2 Treatment should include detorsion followed by either cystectomy or adnexectomy. 2
This was an unusual case of a pregnancy complicated by an isolated tubal torsion that was treated with laparoscopic surgery at 25 weeks of gestation. There were no pregnancy complications secondary to the laparoscopic management. Isolated tubal torsion in pregnancy is extremely rare, with only 19 cases reported to date,
5
and is estimated to occur in 1 in 5000 pregnancies.
4
Although laparoscopy has been shown to be safe in any trimester of pregnancy1,2 to the current authors' knowledge, this is the first reported case of tubal torsion in pregnancy that was treated with laparoscopic surgery. Two previous cases of tubal torsion in pregnancy were described; both were treated with laparotomy for presumed appendicitis.
4
The benefits of laparoscopy for a pregnant patient are the same as in a nonpregnant patient, including quicker recovery, shorter hospital stays, decreased postoperative pain, and less postoperative ileus.
1
The Society for American General Endoscopic Laparoscopists presented clear guidelines for laparoscopic management of surgical cases in pregnancy
1
:
(1) The patient should be positioned in a left lateral decubitus to improve cardiac output and venous return. (2) Entry technique (Hasson or Veress needle) and port placement should take into account the size of the gravid uterus. (3) Insufflation pressures of 10–15 mm Hg can be used safely. (4) Intraoperative CO2 should be measured with capnography; serial blood gases are not recommended. (5) Intraoperative and postoperative compression devices in addition to early ambulation are recommended for venous thromboembolism prophylaxis. These recommendations were followed successfully in the current patient.
Conclusions
This report described laparoscopic management of an isolated tubal torsion during pregnancy with good fetal and maternal outcomes. Adnexal torsion is difficult to diagnose clinically. The only way to make a definitive diagnosis is through surgery, preferably laparoscopy. Laparoscopy is safe in any trimester of pregnancy and should be considered as first-line management for abdominal pathology, such as adnexal torsion, during pregnancy.
Footnotes
Acknowledgments
The current authors would like to acknowledge the patient for providing consent to publish her interesting case and allowing her experience to inform the surgical choice of other physicians who encounter similar clinical dilemmas in pregnant patients. The patient consented to participation and publication. Ethics approval was obtained from the St. Michael's Hospital Research Ethics Board, Toronto, Ontario, Canada (REB 16-299C).
Author Disclosure Statement
The authors report no conflicts of interest. There were no sources of funding for the project. All authors contributed equally to the manuscript preparation. M.H.Y. and E.M.S. were involved in the clinical care of the patient.