
Abstract
Abstract
Objectives:
The aim of this study was to evaluate the outcomes and procedural safety of cesarean myomectomy (CM).
Materials and
Results:
Mean myoma size was 9.6 ± 2.35 (3–25) cm and mean myoma weight was 805.22 ± 221.27 (190–3530) g. Nine patients had ≤5-cm myomas and 46 patients had >5-cm myomas. Eleven patients (20%) had undergone abdominal/laparoscopic myomectomy prior to the current pregnancy. Estimated blood loss was comparable between the 2 groups (555.56 ± 212.78 mL and 726.01 ± 290.16 mL; p = 0.10). Hb fall after surgery was also comparable (1.32 ± 1.31 g% and 1.94 ± 1.15 g%; p = 0.15) between the 2 groups. Duration of surgery was significantly longer in group B, compared to group A. The largest myoma removed in the series was 25 cm (3530 g). Three or more myomas were considered to be multiple myoma. The maximum number of myomas removed in one patient was 13. There was no difference in postoperative hospital stay and any other complications in the two groups. None of the patients required cesarean hysterectomy.
Conclusions:
CM may be considered safe and feasible for both small and large leiomyoma. Surgical expertise is the key factor and the advantage of two surgeries together should be offered to patients after counseling. (J GYNECOL SURG 34:203)
Introduction
U
Vaginal delivery per se is not a contraindication in pregnancies complicated by myomas, but studies have shown a 27% increased risk of cesarean section among pregnant women with myomas, even after adjusting other confounding factors. 3
Myomectomy during cesarean section has been considered controversial and has been discouraged due to fear of intractable hemorrhage and risk of peripartum hysterectomy. Incidence of intraoperative blood loss in cesarean myomectomy (CM) varies from 0% to 35% depending upon the size of the myoma. 4 The main outcome measured in most studies of CM is intraoperative or perioperative blood loss during CM.
However, in the last 2 decades, there have been reports and a meta-analysis of CM, and the procedure has been documented to be safe, compared to cesarean alone.5,6 If these two procedures can be performed safely at the same time, the risk of anesthetic complications, multiple surgeries, adhesions and intra- or postoperative hemorrhage, exorbitant costs of operative procedures, and hospital stay could be reduced.
Myomectomy is relatively easy for small myomas but large myomas (>5 cm) are more difficult to manage due to the risk of intractable hemorrhage and inadvertent hysterectomy. The current authors evaluated 5 years of experience at the All India Institute of Medical Sciences (AIIMS), New Delhi, India, including all patients who presented in pregnancy with myomas and in whom CM was performed. The main outcome measure was intraoperative blood loss during surgery. Secondary outcome measures included hemoglobulin (Hb) fall after surgery, duration of surgery, postoperative hospital stay, need for blood transfusion, and any other major and minor complications.
Materials and Methods
This was a retrospective cohort study including 54 patients who underwent CM during a 5-year period (March 2012 to February 2017) at AIIMS. One patient underwent CM twice; thus, a total 55 cases of CM were analyzed. As this was a retrospective study, institute ethical approval was not required.
All of the patients' antenatal details were reviewed. The information extracted included: whether myomas were diagnosed before or during pregnancy; size, number, and location of myomas; periods of gestation and modes of delivery; indication of cesarean section; infants' birth weights; weight, size, and number of myomas removed; postpartum complications (fever, bleeding, subinvolution); intraoperative, or postoperative hemorrhage; fall in Hb after surgery; need for blood transfusion; and any other minor or major adverse events.
All CMs were performed by a single surgeon (A.K.). Myomectomy was performed after written informed consent was obtained from the patients and assessments of the myomas' operability without incurring increased risks of procedural complications. Baseline hemograms were performed, and patients with Hb <9 g/dL were given iron therapy. The aim was to keep baseline Hb above 11 g/dL, with either oral or injectable iron therapy.
The CM procedure was performed under spinal or combined spinal/epidural anesthesia, except in 3 patients who required general anesthesia (2 emergency cesareans due to nonreassuring fetal heart rate and one due to failed spinal anesthesia).
The main procedural steps of each CM were as follows:
Transverse/vertical abdominal incision was made, depending upon the size, number, and location of the myoma(s). Assessment was performed and the infant was delivered. If a fibroid was in the lower uterine segment, then a higher transverse/vertical incision was made. After the infant was delivered, 30 international units (IU) of oxytocin was given intravenously (IV) to the mother. The surgeon waited until the uterus was well-contracted. Additional uterotonics/hemostatic procedures were performed at the surgeon's discretion, depending upon the size and number of myomas. The following methods were used to reduce blood loss during surgery:
Injection of carboprost (0.25 mg intramuscularly [IM]) Injection of methergin (0.2mg IV) Hot mops applied to the exteriorized uterus Tablet of misoprostol administered (1000 mcg per rectal) Bilateral uterine artery ligation Bilateral internal iliac ligation Intermittent clamping of infundibulopelvic ligaments. Once uterine contraction was ensured, diluted vasopressin was injected (20 IU in 200 mL of normal saline) into the subcapsular space of the myoma. Incision over the myoma was made, and enucleation was performed using electrocautery and blunt dissection. Myomectomy was performed by dissecting in the correct plane and dissecting inside the myoma capsule. The myoma bed was sutured with barbed sutures (V-Loc™180; 03.5 Mteric; M/s Covidien, United States Surgical, North Haven, CT). Hemostasis was ensured and an intra-abdominal drain was inserted if required. 20 IU/500 mL of oxytocin infusion was continued for first 24 hours after CM.
The primary outcome measure was estimated blood loss (EBL) during CM. Secondary outcome measures included Hb fall after surgery, duration of surgery, hospital stay, postoperative fever, and any other minor and major complications. Duration of surgery was calculated from skin incision to skin closure. Postoperative fever was defined as a temperature ≥ to 38°C.
Subgroup analysis was performed among patients with the largest myomas ≤5 cm (group A) and with patients with myomas >5 cm (group B). This 5-cm cutoff was chosen, as it amounts to an ∼50 cm3 volume. Maternal characteristics, features of myomas, pregnancy, and procedural outcomes were compared between the 2 groups.
Results
Fifty-four patients underwent cesarean myomectomy during the study period. One patient underwent CM twice so a total of 55 cases were analyzed. Of this total, 36 (65.4%) patients were already aware of having myomas and conceived during treatment or while waiting for surgery. The rest of the patients (19/55; 34.5%) learned that they had myomas only after conception during routine antenatal scans. AIIMS is a tertiary-care center, and most of these patients were referred from other hospitals, either for laparoscopic myomectomy or with the diagnosis of pregnancy with myoma. This was the reason for most of the patients having >5-cm myomas.
Table 1 shows the baseline characteristics of the study subjects. An attempt was made in the antenatal period to keep the Hb of these patients ≥11 g%, either with therapeutic oral or injectable iron therapy. Because of having moderate-to-severe anemia in the antenatal period, 16/55 (29%) patients received injectable iron therapy as either iron sucrose or ferric carboxymaltose, which was given IV according to the Hb deficit.
Data are presented at mean ± standard deviation (minimum–maximum).
BMI, body mass index; POG, period of gestation; Hb, hemoglobulin; EBL, estimated blood loss.
Table 2 shows the indications of cesarean section in the study group. Elective CM was performed in 35/55 (63.6%) patients at 37–39 weeks. Figures 1 and 2 show different sizes and locations of myomas in different cases.

Different locations and types of myomas.

Different myomas.
CS, cesarean section.
Eleven (20%) patients had undergone laparoscopic myomectomy prior to the current conception. Figure 2C illustrates a patient with recurrent multiple myoma after laparoscopic myomectomy was performed 4 years prior at AIIMS.
Table 3 shows different locations of leiomyomas in the study groups. The largest myoma removed was 25 cm (3530 g). Three or more myomas were considered to be multiple myomas. The maximum number of myomas in 1 patient was 13. In patients with multiple myomas, the total weight of all the myomas was given for analysis.
LUS, lower uterine segment.
As large myomas are expected to be associated with more blood loss and other complications, an arbitrary cutoff of 5 cm was chosen, and outcome parameters were compared between ≤5 cm myomas (n = 9) and >5 cm myomas (n = 46). Table 4 shows the baseline characteristics and outcome parameters in the 2 groups according to the sizes of their myomas.
Values are presented as mean ± standard deviation.
p-Value <0.05 is significant.
BMI, body mass index; POG, period of gestation; EBL, estimated blood loss; Hb, hemoglobulin.
Bilateral uterine artery ligation was done in 26% (12/46) patients in group B as a measure to reduce intraoperative blood loss.
Lower uterine segment (LUS) cesarean section was performed in all patients except 1, in whom a classical cesarean section had to be performed due to a large lower-segment myoma (20 × 25cm; Fig. 1F).
In 5 patients, the myomas were anterior in the LUS (Fig. 1B and C). After delivering the infants, these myomas were removed through same LSCS incisions as the myomas protruded through the incisions. Myomectomy was done only after delivering the infants.
In patients with multiple myoma, different incisions were made on the anterior and posterior walls (Fig. 2B).
If adjacent, the myomas were removed through tunneling incisions. A transcavitary approach was avoided due to its detrimental effect on endometrium.
The endometrial cavity was opened in 6/55 patients and was sutured with 2-0 Vicryl.
Two patients in group A (1 patient—1 pint; 1 patient—2 pints) and 7 patients in group B (4 patients—1 pint; 2 patients—2 pints; and 1 patient—3 pints) received blood transfusions.
One patient had undergone laparoscopic myomectomy for multiple leiomyomas prior to conception. Later on, she had a recurrence of her myomas and conceived spontaneously twice. Cesarean myomectomy was done both times, and 5 and 7 myomas were removed, respectively. The procedure was uneventful both the times.
Mean blood loss (Fig. 3A) was higher in group B (726.01 ± 290.16 mL) than in group A (555.56 ± 212.78 mL), although the difference was not statistically significant. Mean Hb fall (Fig. 3B) was also comparable among the 2 groups. Duration of surgery was significantly higher in group B than in group A. There was no significant difference in postoperative hospital stay and febrile morbidity. None of the patients underwent cesarean hysterectomy.
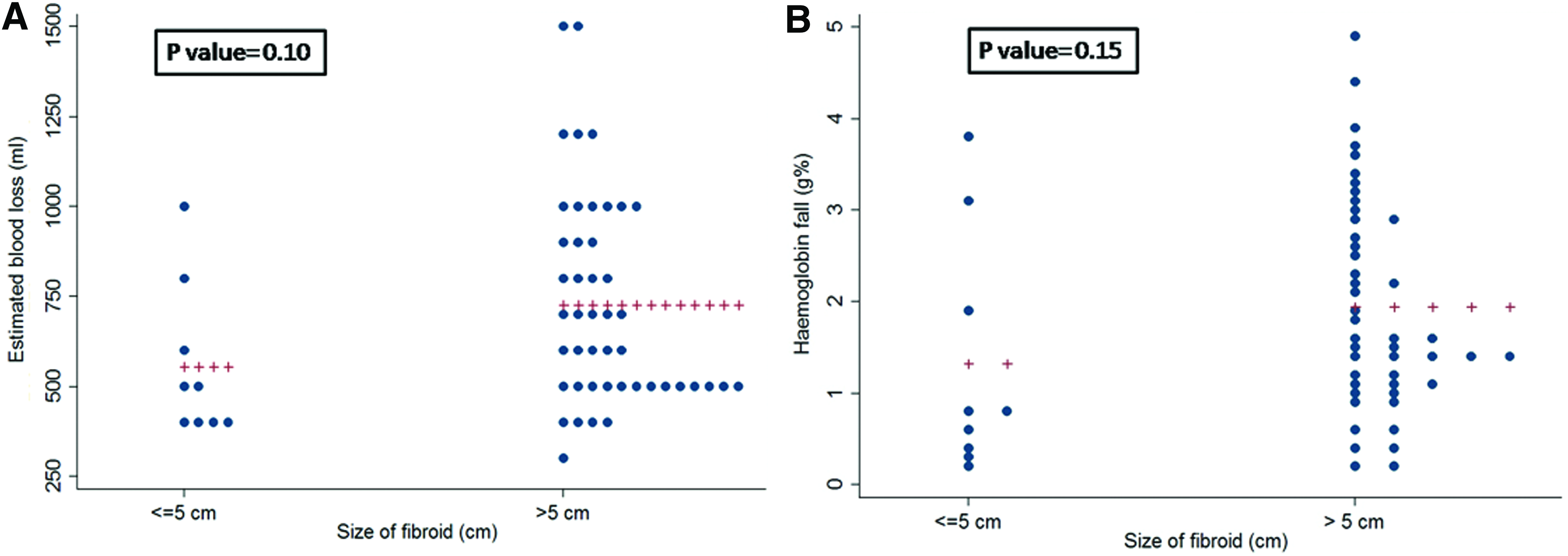
Dot plot showing
Histopathology of all cases revealed benign leiomyomas. Most of the cases had features of cystic or hyaline degeneration, with 6/55 cases showing features of red degeneration. One patient had features of calcification, and none of the cases reported had leiomyosarcomas.
Discussion
The present retrospective cohort study was performed to evaluate the efficacy and feasibility of CM in current obstetrics practice.
The first CM was performed by Bonney et al. 7 in 1913 but has been discouraged by most researchers and writers of textbooks until recently. It is still controversial whether or not to do CM. The reason this procedure is not popular is risk of intractable hemorrhage and risk of peripartum hysterectomy. 8
There are no prospective randomized studies published on the safety and feasibility of CM, but there are a few case reports and retrospective studies. Lately, due to technical advances in surgery, availability of blood products, anesthesia expertise, the acceptance for CM is increasing.
In a meta-analysis by Song et al., the outcomes—estimated blood loss (EBL) and incidence of hemorrhage—was comparable whether cesarean section was performed with or without myomectomy. 9 In the present study also, EBL and Hb fall did not differ significantly among patients with small or large myoma.
As leiomyoma complicating pregnancy is a predisposing factor for increased blood loss during cesarean section, building up Hb in the antenatal period can reduce intraoperative and postoperative blood transfusion rates. All patients in the present series were investigated for anemia and their Hb was kept at >11 g/dL, either with oral or injectable iron therapy.
Kwon et al. evaluated the safety of CM in >5-cm myomas. There was no significant difference in mean Hb drop, operative time, and length of hospital stay among patients with myomas <5 cm or >5 cm. The study researchers concluded that CM is equally safe for patients with larger myomas when CM is performed by expert surgeons. 5
AIIMS is an established tertiary-referral center for laparoscopic myomectomy and, due to a long waiting list, many patients conceive while waiting for laparoscopic myomectomy. Patients who are pregnant and have large fibroids are also referred due to the high-risk status of these cases. This is the reason for most of the patients having myomas >5 cm in the present series. Mean myoma size in the present study was 9.6 ± 2.35 (3–25) cm.
Use of barbed sutures helps achieve rapid and tight closure of the myomectomy bed, thus reducing the time for suturing and overall time for surgery. In a meta-analysis by Song et al, the operative time was 4.94 minutes longer in a CM group than in a cesarean delivery group, with the difference being nonsignificant. 9 In the current series, group B had significantly longer durations of surgery, compared to group A. This can be explained by significantly larger myometrial defects that needed to be closed in group B.
For a same-sized myoma, the incision required is smaller at the time of cesarean, compared to the incision required for a nongravid uterus. It is technically easier to visualize the ascending uterine artery against light after exteriorizing the uterus. It can be required either prophylactically for a large vascular myoma or as a measure to avoid excessive bleeding. 10 Due to more elasticity of the gravid uterus, closure of the uterine defect after myomectomy is easier, compared to closure of a nongravid uterus.
Multiple leiomyomas are considered as a relative contraindication to CM due to risk of increased blood loss and longer duration of surgery. 11 A decision for myomectomy should be made by the treating obstetrician, taking into account management of excessive intraoperative blood loss and need for repairing multiple myometrial defects. Tunneling incisions or separate anterior- and posterior-wall incisions can be made to approach different myoma. A transcavitary approach should be avoided due to the risk of endometrial damage. In the present series, 18/55 (32.7%) patients had multiple myomas, and the maximum number of myomas removed in 1 patient was 13.
Leiomyomas, if left in situ, have their own complications in the postpartum period and in future pregnancies. The notable complications include postpartum hemorrhage, subinvolution of the uterus, myoma prolapse due to uterine contraction, future infertility, pregnancy losses, preterm deliveries, fetal growth restriction, malpresentations, and increased chances of cesarean deliveries. All of these complications increase with increasing size of the myomas and are more likely to occur with myomas sized >5 cm or a fibroid volume >50 cc 3 . 12
Careful selection of cases and decisions by the obstetrician are very crucial. Uterine atony, close proximity of myomas to large vessels, associated congenital or acquired coagulopathy, and multiple myomas are relative contraindications and CM should be avoided. 13 Only surgeons who are proficient in performing myomectomy in a nongravid uterus should do CM.
CM has been discouraged in patients with previous myomectomies due to the higher rate of complications.5,14 However, in the current series, 11 patients had previous laparoscopic/abdominal myomectomies and no major/minor complications were recorded in these patients.
Complications of CM in future pregnancies include uterine dehiscence, uterine scar rupture, placental implantation abnormalities, adhesions, and recurrence of myomas. Akkurt et al. did not report recurrence of myomas in their study of subsequent pregnancies. 15 In the current series, one patient underwent CM twice after laparoscopic myomectomy and the procedures were uneventful both times.
Technical aspects that led to successful management of the current patients were: antenatal Hb buildup; an experienced operating obstetrician delaying myomectomy until the uterus was well-contracted; use of diluted vasopressin along with uterotonics; a minimum number of incisions and avoiding the endometrial cavity; exteriorizing the uterus and ligation of uterine arteries against light; dissecting inside the myoma capsule; use of barbed sutures; and fast and accurate approximation of myometrial defect.
Conclusions
CM, if done by an experienced obstetrician, may be performed even in patients with large leiomyomas. If two procedures can be performed safely at the same time, the risk of anesthetic complications, multiple surgeries, adhesions, intra- or postoperative hemorrhage, exorbitant costs of operative procedures; and hospital stays could be reduced.
Footnotes
Acknowledgments
A.K. was the main operating surgeon in all of the cases and provided final approval of the article. R.M. was the chief assistant in all of the cases. R.M., G.K., I.K., and T.G, drafted the article and assisted in the surgery. M.K. analyzed the data.
Author Disclosure Statement
There are no conflicts of interest for any of the authors.