
Abstract
Abstract
Background:
Ovarian mature cystic teratomas are common, benign, pelvic tumors easily detected by ultrasonography. These tumors are bilateral in 8% to 15%, and recurrent teratomas are uncommon and underdiagnosed. A benign dermoid cyst is the most common ovarian mass to develop torsion. Although uncommon, adnexal torsions are an important cause of gynecological emergencies. It was previously thought that untwisting the adnexa could result in an embolus from thrombosed veins but this has proved untrue. Currently, it is considered that laparoscopic conservative management by untwisting the ovary allows recovery of almost all cases, even when the ovaries seem nonviable.
Case:
This article presents a case of an ovarian torsion in a 23-year-old nulliparous woman referred to our emergency room because of acute right iliac fossa pain. Ultrasound showed a complex right adnexal mass 60 × 60 mm. Three years earlier she had undergone, in an urgent context, a left adnexectomy and a right cystectomy for bilateral teratoma and torsion of the left ovary. We decided on a conservative laparoscopic approach with adnexal detorsion.
Results:
At a follow-up visit, one year after the episode, the TVUS showed an ovary of normal size and appearance.
Conclusion:
This case demonstrates the importance of conservative treatment of adnexal torsion, especially in young women, allowing them to maintain their fertility.
Introduction
A
Almost 15% of mature cystic teratomas develop torsion, with rupture being a rarer complication. Adnexal twist accounts for 3% of gynecologic emergencies. 4
Until recently, the recommended treatment was oophorectomy in order to avoid the release of potential embolic thrombi from the ovarian vein. However, conservative treatment with adnexal detorsion has shown that ovarian function can be restored, which is critical in young women who have not yet completed their families. 5
This article presents a clinical case of a nulliparous woman, who had previously undergone unilateral oophorectomy for a mature cystic teratoma. She developed ovarian torsion after recurrence of the neoplasia. Despite the poor aspect of this ovary, in order to preserve this patient's fertility, conservative treatment with laparoscopic adnexal detorsion was chosen. This approach proved to be effective. In a second-look surgery, cystectomy was performed, and the follow-up showed a reestablishment of ovarian function.
Case
A 23-year-old female patient—nulliparous, with no relevant personal history—went to an emergency department due to pain in the right iliac fossa; this pain had lasted for 2 days. Three years earlier, she had undergone, in an urgent context, a left adnexectomy and a right cystectomy for bilateral teratomas and for torsion of her left ovary. Anatomopathologic testing had revealed bilateral mature cystic teratomas. There had been no follow-up with a gynecology consultation after this event.
On this patient's current admission, a physical examination revealed that she had pain on palpation of the right lower quadrant of her abdomen, but she did not have any signs of peritonitis. She was afebrile and hemodynamically stable. Gynecologic transvaginal ultrasonography (TVUS) identified a complex right adnexal mass with solid components, focal echogenic areas, and heterogeneous content. The mass was 60 × 60 mm, and there was a small amount of free liquid in the Douglas sac fundus.
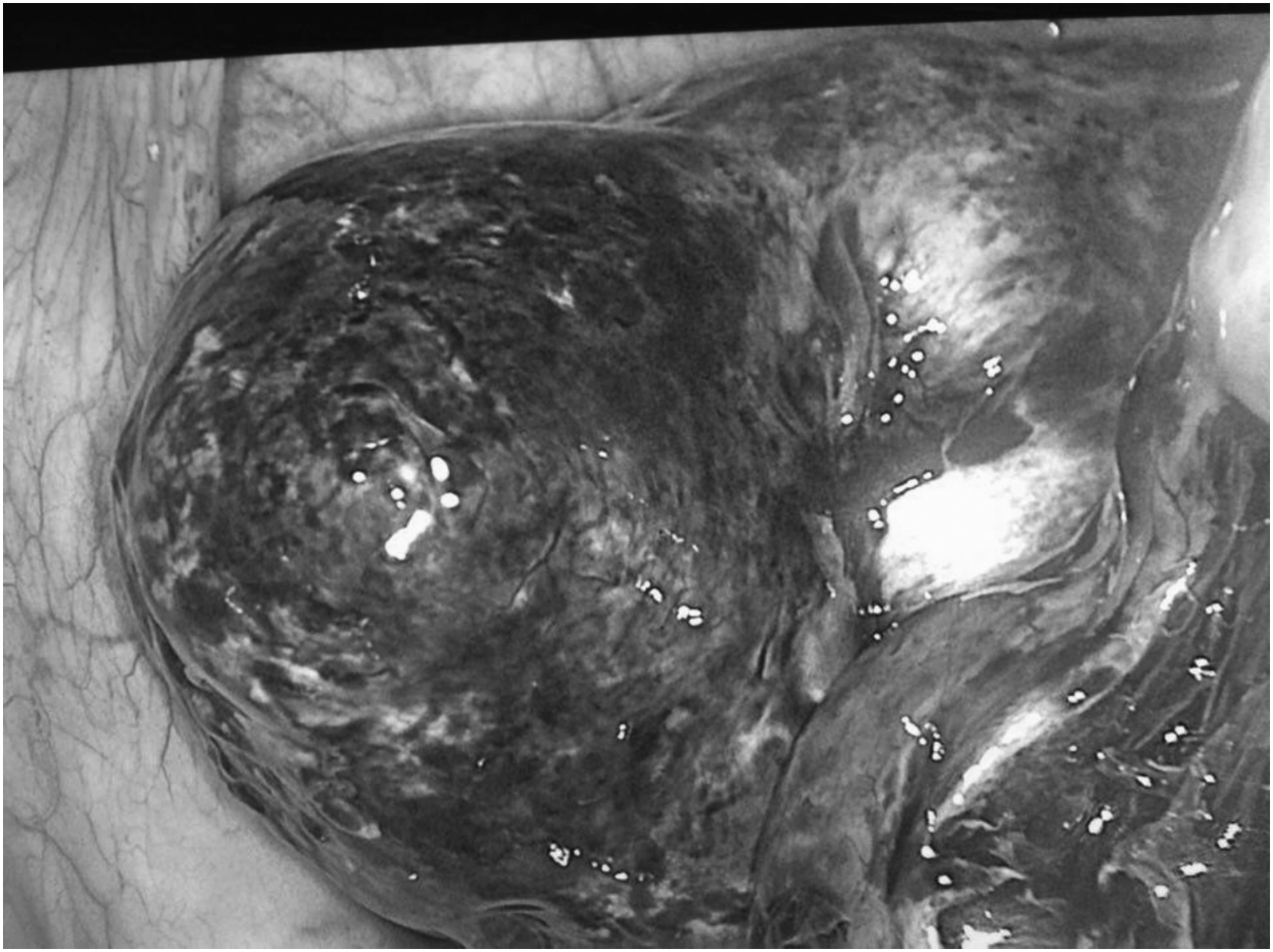
The suspected diagnosis was torsion of this right adnexal mass. Diagnostic laparoscopy, performed 48 hours after this patient's admission, confirmed the torsion of the right adnexa that was transformed into a mass of ∼60 mm that was dark, hemorrhagic, and edematous (Fig. 1). Laparoscopic detorsion was performed, and 30 minutes later normal color of the mass was partially restored (Fig. 2). In an effort to prevent recurrence, ovariopexy was performed on the posterior wall of the uterus.
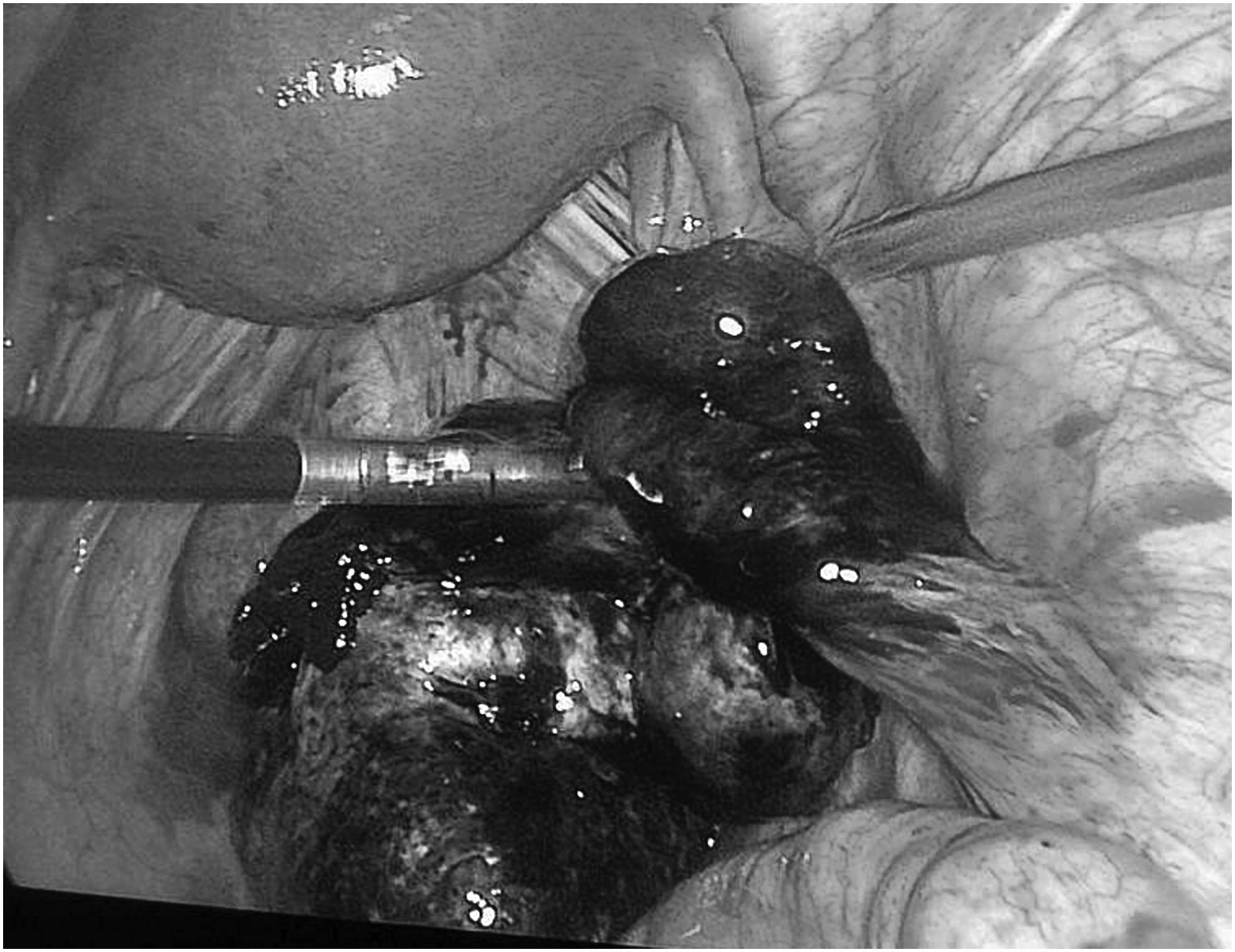
Right adnexa and round ligament rotated under the midline.
Ovary with diffuse edema, increased volume, black color, and hemorrhagic appearance.
Results
This patient's postoperative period was uneventful, and she was discharged on the second postoperative day. Six weeks later, diagnostic laparoscopy was repeated and the ovarian cyst was smaller, with no signs suggestive of ischemia (Fig. 3). It was decided to proceed to laparoscopic cystectomy. Histologic testing confirmed that she had a dermoid cyst.

Detorsion of the adnexa via laparoscopy.
After the surgery clinical, imaging (with TVUS) and an analytical follow-up (with evaluation of basal levels of follicle-stimulating hormone and estradiol) were performed. At a follow-up visit, 1 year after the current episode, TVUS revealed that she had complete resolution of the torsion, and the TVUS also showed an ovary of normal size and appearance.
Discussion
The current patient presented with a mature cystic teratoma in the right ovary, complicated by torsion. She had a history of bilateral mature cystic teratomas that had been resolved with a left adnexectomy and a right cystectomy. Thus, this present case shows recurrence and the potential bilaterality of mature cystic teratomas, as well as providing information for discussion regarding appropriate treatment in situations involving adnexal torsion.
The bilaterality rate of this type of tumor, reported in the literature, ranges from 8% to 15%. 6 There are few studies about recurrence of mature cystic teratomas, and the published data do not cover differentiating among true recurrences, incomplete excisions, or misdiagnosed cysts in the same ovary. It was not possible to find any published evidence about a second dermoid cyst misdiagnosed in surgery. One retrospective multicenter cohort study of mature cystic teratomas removed by laparoscopy, compared to exploratory laparotomy, found significantly more ipsilateral recurrences in the laparoscopy group between 2 and 24 months postoperatively, and calculated the probability of recurrence at 2 years to be 7.6% when laparoscopy was performed and 0% when laparotomy was performed. 7 Was it possible that the surgical technique affected the recurrence rate?
Similar to the present case, in Laberge and Levesque's study, 7 the relatively short time between initial surgery and recurrence was <24 months, and the fact that these cysts can grow slowly and without clinical symptoms, both suggest that an apparent recurrence could result from incomplete removal rather than a true new occurrence of a teratoma.
Another issue raised by the current case is optimal surveillance after surgery. According to Taskinen et al., after oophorectomy, 5 of 22 patients (23%) each developed benign tumor in the contralateral ovary. 8 These researchers suggest that annual ultrasonography surveillance be applied in such cases but, given the slow growth of teratomas, their small rate of recurrence, and their rare risk of malignancy, it could be argued that regular surveillance is not required.
Conventionally, it was believed that the detorsion of the adnexa could result in a plunger released by thrombosed veins, but this has not been proven. Two studies have demonstrated that a conservative laparoscopic approach, through adnexal detorsion, allows recovery of ovarian function in almost all cases, even when it is not feasible to the repair the adenexa.9,10
Conclusions
Through the described case, the current authors presented an atypical presentation of a frequent entity—a mature cystic teratoma of the ovary. In addition, this case demonstrated the advantage of avoiding radical surgery, regardless of the aspect of the ovary, given that a radical surgical approach is not justified and could compromise a patient's reproductive future.
Footnotes
Author Disclosure Statement
No competing financial conflicts of interest exist.