
Abstract
Abstract
Background:
Interventional radiologic techniques can be used to aid in the management of complex obstetric and gynecological disorders such as postpartum hemorrhage, fibroids, placenta accreta/percreta, arteriovenous malformations (AVMs) and other disorders associated with morbidity and mortality.
Case:
A 36-year-old female, with a history of 2 second-trimester spontaneous abortions, presented for surgical evaluation for a planned hysterectomy after pelvic magnetic resonance imaging showed a significant uterine AVM. Due to concern about hemorrhage during the surgery, bilateral iliac and bilateral ovarian arterial balloon catheters were placed intra-arterially, under fluoroscopic guidance, prior to surgery. After placement of the balloon catheters, with the patient under conscious sedation, she was transferred to the operating room and given general anesthesia. Diagnostic hysteroscopy showed that she had intrauterine scarring consistent with prior dilations and curettages. The balloons were inflated during surgical removal of the uterus and fallopian tubes. After the hysterectomy and salpingectomies, the balloon catheters were deflated. The patient was hemodynamically stable. The catheters were removed. The abdomen was suction irrigated and CO2 was suctioned out. The ports were removed, and the fascia and skin were closed. She underwent cystoscopy, which showed no injury to the bladder and ureters. Given her risk of potential intra-abdominal bleeding, she was then transferred to the intensive care unit for observation.
Results:
She was stable overnight and was transferred to the regular floor the following day. Her complete blood count in the morning was normal. Once she tolerated a regular diet, and ambulated and voided spontaneously, she was discharged from the hospital.
Conclusions:
As this clinical case illustrated, percutaneous, minimally invasive image–guided, interventional techniques may be used for patients with complex obstetric/gynecologic conditions. It is vital to recognize the importance of the multidisciplinary approach to the treatment of such patients.
Introduction
T
Case
A 36-year old female, with a history of 2 second-trimester spontaneous abortions, presented for a preoperative appointment for a planned hysterectomy after pelvic magnetic resonance imaging (MRI) showed that she had a significant uterine AVM. She wished to have children; therefore, she desired ovarian stimulation and subsequent egg retrieval as well as use of a surrogate to carry a pregnancy to term. However, given her AVM and high risk for bleeding, her infertility specialists recommended a hysterectomy prior to fertility treatment. Of note, a previous uterine artery embolization (UAE) had failed due to the size of her AVM.
She reported having regular monthly menses, and did not have dysmenorrhea, dysuria, or unusual vaginal discharge/odor/itching. She denied having any rectal bleeding. Her past surgical history included diagnostic laparoscopy for reasons not elicited, tonsillectomy, and dilation and curettages.
On physical examination, it was noted that she had an audible bruit over the uterus. Her vulva, vagina, cervix, uterus, adnexae, and cul-de-sac were all normal. Rectal examination and hemoccult blood tests were not performed.
The patient was informed of the risks of interventions and surgery, and she consented to both. Bilateral iliac and bilateral ovarian, arterial balloon catheters were placed, with fluoroscopic guidance prior to diagnostic hysteroscopy, supracervical hysterectomy, bilateral salpingectomy, and cystoscopy.
After placement of the balloon occlusion catheters (Fig. 1) with this patient under conscious sedation, she was transferred immediately to the operating room (OR). Occlusion balloons were placed through four separate percutaneous, common, femoral arterial punctures. Over the wire, five French Fogarty embolectomy catheters were used, with one placed in the main trunk of each internal iliac artery and the others placed in the orifices of the hypertrophied ovarian arteries. Once in place, the occlusion balloons could be inflated during surgery. Once she was in the OR, this patient was given general anesthesia.
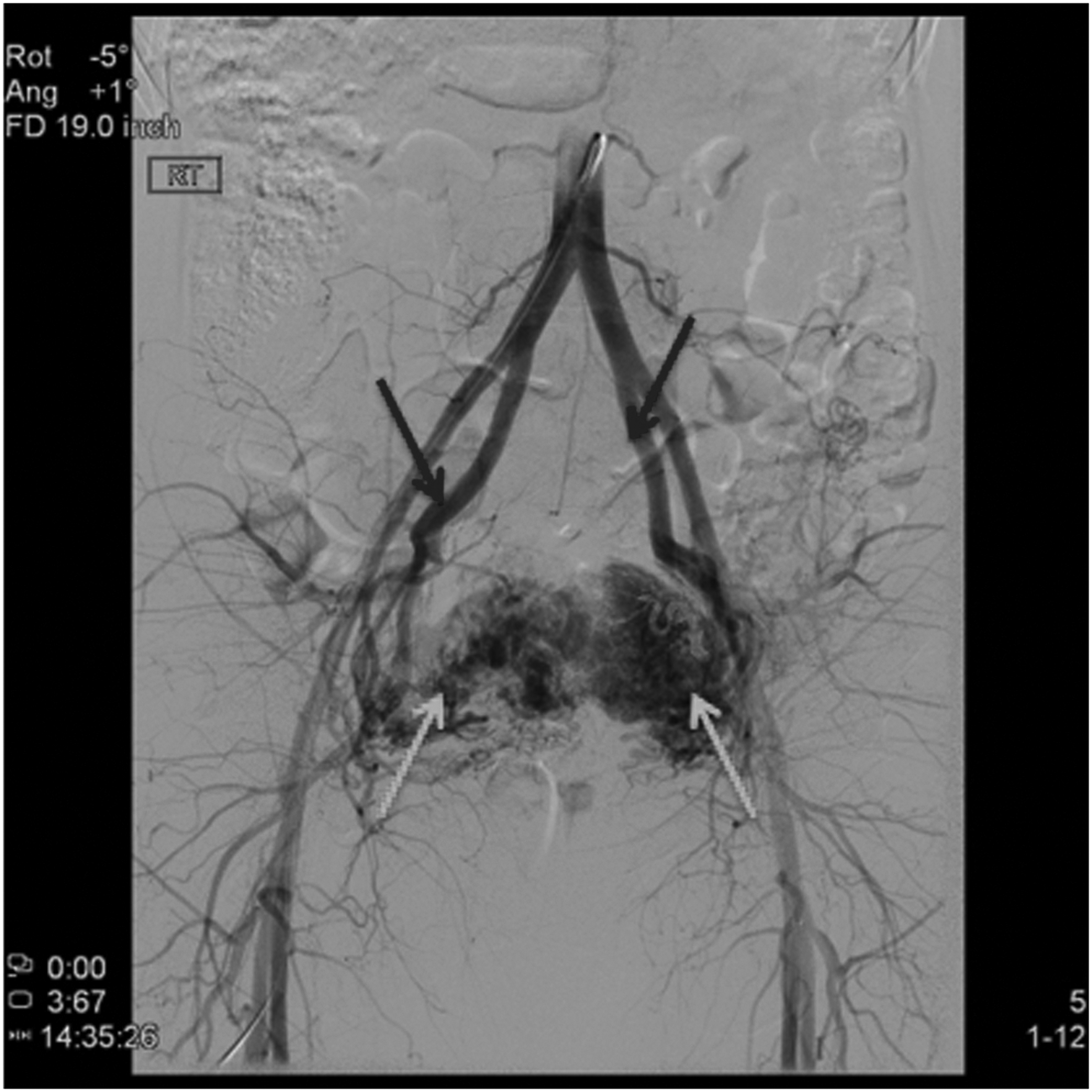
Black arrows: Internal iliac arteries, in which balloon catheters were placed proximally. White arrows: Large uterine arteriovenous malformation.
Diagnostic hysteroscopy showed that this patient had intrauterine scarring consistent with prior dilations and curettages. There was a suggestion of underlying vascularity deep to the endometrium. Otherwise, the endometrial cavity appeared to be normal. Diagnostic laparoscopy showed that the upper abdomen was normal. A pelvic examination revealed that she had prominent dilated vasculature that was most prevalent bilaterally at the ovarian vessels (Fig. 2). The balloons were inflated during the surgical removal of the uterus and fallopian tubes. With these occlusion balloons temporarily inflated to reduce arterial pressure to the four main arterial feeders to the large uterine/adnexal AVM, the entire uterus was removed via a 15-mm Karl Storz morcellator. After the hysterectomy and salpingectomies, the intra-arterial balloon catheters were deflated. The patient was hemodynamically stable, and the catheters were removed. The abdomen was suction irrigated, and CO2 was suctioned out. The ports were removed, and the fascia and skin were closed. She underwent cystoscopy, which showed no injury to the bladder and ureters. Given her risk of potential intra-abdominal bleeding, she was then transferred to the intensive care unit for observation.
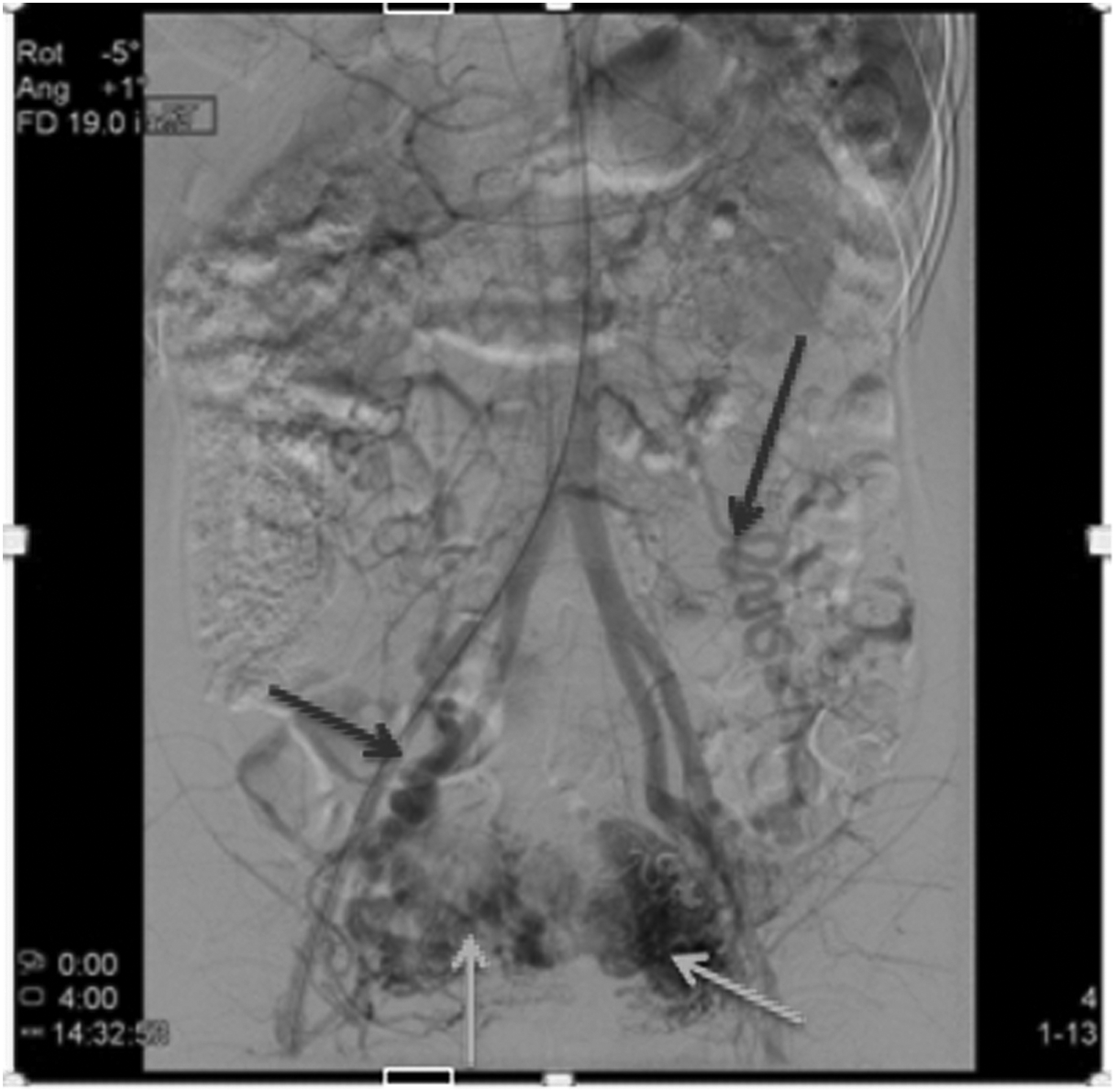
Black Arrows: Both ovarian arteries contributed to the arteriovenous malformation (AVM). White arrows: Large uterine AVM.
Results
This patient was stable overnight and was transferred to the regular floor the following day. Her complete blood count in the morning was normal. Once she tolerated a regular diet, ambulated, and voided spontaneously, she was discharged from the hospital.
Literature Review
AVM is an abnormal connection between arteries and veins without the normally connecting capillaries. 1 This abnormal shunting results in massive quantities of blood in the lower resistance veins, which then results in enlarged veins and enlarged tissues. 1 AVMs are very rare and complicated to treat due to a vast blood supply to them and a vast quantity of blood within them. 2 When found, they usually are located in the brain, neck, lungs, and kidneys. 3 Pelvic AVMs are relatively rare, but can be seen after trauma; for example, the current patient had prior dilations and curettages. 3 In such cases, some investigators feel the lesion is “acquired” due to instrumentation. Commonly, AVMs can become symptomatic during or after pregnancy. Symptoms include mild discomfort, dysuria, a sensation of pressure, vaginal or rectal bleeding, cardiac volume overload, and congestive heart failure. 4 When women present with major hemorrhage, embolization of the uterine AVMs can be necessary.
Angiography of the iliac arteries is the best diagnostic tool and potentially allows for embolization; however, angiography is invasive. Computed tomography with contrast can also be used to diagnose and monitor AVMs; however, this is not ideal for a pregnant woman or a woman of childbearing age. Uterine/pelvic AVMs can be seen using transvaginal ultrasonography or with pelvic MRI with intravenous gadolinium. As shown by Suzuki et al., pelvic AVMs can also be diagnosed by transrectal ultrasound (US). 3
Treatments have included percutaneous arterial embolization and surgical excision, both of which are associated with high recurrence rates. Surgical excision often results in massive hemorrhage. 1 As mentioned above in this case, bilateral femoral artery catheters were placed with balloons in both internal iliac and both ovarian arteries. This was accomplished and used to temporarily decrease blood flow to the large AVM during the hysterectomy. The purpose of this case study is to illustrate an interventional radiologic technique that can be used to reduce blood flow temporarily in a rare case of a large uterine AVM requiring hysterectomy. This procedure was performed several years ago, and the patient has had no complications from the intervention or procedure. A few weeks prior to writing this article, a surrogate for this patient had delivered healthy twin baby boys.
Postpartum hemorrhage
According to the World Health Organization, ∼800 women worldwide die each day from pregnancy-related or childbirth-related complications. 5 In the United States, the maternal mortality ratio is ∼18.5 deaths per 100,000 live births. In some developing countries, the maternal mortality ratio can be 500 deaths per 100,000 live births. 6
The leading cause of maternal mortality is postpartum hemorrhage, which, according to the American College of Obstetrics and Gynecology (ACOG), is defined as blood loss of >500 mL following vaginal delivery or >1000 mL following cesarean delivery. Estimated blood loss (EBL) is subjective; therefore, a drop in hematocrit by 10% may be used to measure EBL as well. 7 Recognizing and treating postpartum hemorrhage correctly is essential. It is necessary to resuscitate the patient and determine the cause of the bleeding. The ACOG suggests four main etiologies: (1) uterine atony; (2) retained placental tissue; (3) trauma (lacerations); and (4) coagulopathies. About 50%–75% of postpartum hemorrhages are due to uterine atony, and 5% of births result in uterine atony.7,8 Therefore, risk factors for all etiologies prior to delivery must be considered. If standard, noninvasive techniques are refractory, surgery and interventional techniques are often utilized. Surgical techniques—such as hysterectomy, uterine artery ligation, and B-Lynch suturing—could result in sterility and all patients who have these procedures face the risks of anesthesia.
The first interventional technique—pelvic artery embolization (PAE)—was first reported in 1979 and gained acceptance rapidly as the primary treatment after failure of conservative treatment. 9 PAE begins with angiography to find active bleeding sites. Then, an absorbable gelatin sponge or other products are placed through catheters (embolization), which causes cessation of the bleeding. Lee et al. demonstrated in their retrospective study that PAE was technically successful (cessation of bleeding) in 225 of 251 (89.6%) patients. 8 The first attempt at embolization was clinically successful in 217 (86.5%) patients, while the overall clinical success rate of all PAE events was 90.4% (227 of 251 patients). 10
In a study by Niola et al., there were 63 obstetric patients with a high risk of hemorrhage. 10 Of these patients, 22 had ectopic cervical pregnancies and 41 had postpartum hemorrhage. All 63 patients were treated with an interventional approach and their charts were reviewed retrospectively. After gaining femoral access (generally on the right side) selective angiography of the internal iliac arteries and superselective angiography of the uterine arteries were performed. Of the 41 patients with postpartum hemorrhage, 32 were treated with polyvinyl alcohol as the embolization agent, 6 were treated with acrylic glue, 2 were treated with Gelfoam,® and 1 was treated with polyvinyl alcohol plus coils. These agents were selected after the interventional radiologist was able to visualize the angiographic map to determine which agent was best for each patient.
In 38/41 patients with postpartum hemorrhage, 1 procedure of embolization was adequate to prevent hemorrhage. The other 3 patients required a second treatment to achieve hemostasis. However, 14 patients did require hysterectomy. Thirteen of the 14 hysterectomies were performed due to placenta percreta and 1 hysterectomy was performed for unstated reasons. One-year post PAE, it was found that 11 of the 27 patients who had had postpartum hemorrhage were pregnant at this follow-up. The remaining 16 patients were ovulating regularly, as shown in US and patient records. 10 PAE is an effective technique for treating and preventing postpartum hemorrhage, and generally maintaining fertility.
Fibroids
Fibroids are the most common benign tumors in women, with an incidence ranging from 40% to 70%.11,12 Often, patients are asymptomatic when they have small fibroids. However, patients can become symptomatic, based on the size and location of the fibroids. According to the ACOG, symptoms include changes in menstruation, pain, pressure, enlarged uterus and abdomen, miscarriages, and infertility. 13
The first case of UAE to treat uterine fibroids was by Ravina in the late 1980s. 14 He performed the embolization on patients (e.g., those with symptomatic fibroids who underwent myomectomy) several days prior to surgery as a prophylactic attempt to control bleeding during the operations. What he found was that many of these patients experienced symptomatic relief of their fibroids and cancelled their upcoming surgeries. 14
Since then, UAE has been used to treat symptomatic fibroids. Due to the vast blood supply to the uterus, bilateral UAE is required. As previously mentioned, access is gained to the uterine arteries and embolic agents—such as polyvinyl alcohol, and, more recently, newer agents—are placed, causing infarction of the fibroids. 13
In a study by Dsouza et al., 25 patients were treated with UAE for symptomatic fibroids. 12 Pretreatment mean size of the fibroids was 7 cm (range: 4–11cm) on US. Of these 25 patients, 49 uterine arteries were embolized. It was not possible to embolize 1 artery due to the patient's congenital hypoplasia. Menorrhagia persisted in 7 patients (68% reduction), dysmenorrhea in 4 patients (71% reduction), and pressure symptoms in 2 patients (75% reduction), respectively, at a 6-month follow-up. At a 2-month follow-up post embolization, the mean size of the patients' fibroids was 4 cm (range: 2–5 cm; 45.5% reduction) and, at 6 months, the mean size was 3 cm (range: 1–4 cm; 57% reduction). One patient remained symptomatic with an increase in her fibroid size and had to undergo hysterectomy. 12
In another study, Spies et al. showed success in treating symptomatic fibroids with UAE, as well. In this study, 200 patients underwent UAE, and follow-ups were obtained. Menorrhagia was reduced in 87% and 90% of patients at 3 months and 1 year post UAE, respectively. Bulk symptoms were reduced in 93% and 91% of patients at 3 months and 1 year post UAE, respectively. 15
In an even larger study by Walker and Pelage, 400 patients underwent UAE for symptomatic fibroids. At a mean follow up time of 16.7 months, menorrhagia was reduced in 84% of women and dysmenorrhea was reduced in 79%. Using US, the median uterine and dominant fibroid volumes before embolization were 608 cc and 112 cc, respectively, and, after embolization, 255 cc and 19 cc, respectively. Twenty-three (6%) patients had clinical failure or recurrence. Ninety-seven percent of women were pleased with the outcome and stated that they would recommend this treatment to others. 16
Placenta accreta
Abnormal placentation is another condition in pregnant patients with relatively high morbidity and mortality. The term placenta accreta is the general term to describe when the placenta, either partially or completely, attaches abnormally to the myometrium of the uterus. Placenta increta is defined as when the chorionic villi of the placenta invade the myometrium. Placenta percreta is defined as invasion of the placenta completely through the myometrium and serosa—and can invade adjacent structures. After the fetus is delivered, the placenta is unable to detach completely and can cause massive hemorrhage. 18 In these cases, a patient may lose 3–5 L of blood.17,18 Therefore, it is imperative to diagnose placenta accreta prior to delivery, as a multidisciplinary approach will be needed throughout pregnancy and delivery. Diagnosis can be made by US. In the last 30 years, the incidence of placenta accreta has increased from ∼0.8 per 1000 deliveries to 3 per 1000 in the past decade. This is presumed to be due to an increase in cesarean sections over this same amount of time. Other risk factors include prior placenta previa, advanced maternal age and multiparity, and other trauma to the uterus including surgery and curettage.17,18 For these reasons, cesarean section followed by hysterectomy should be scheduled at ∼36–37 weeks of pregnancy, prior to cervical effacement. 19
From an interventional radiology standpoint, while there are no definitive data on occlusion of the hypogastric arteries, it is a simple option that can be utilized to minimize blood loss. In a study by Kidney et al., 5 patients with placenta accreta underwent balloon occlusion of the hypogastric arteries after their cesarean sections, but prior to their hysterectomies, with hypogastric artery ligation. 20 The EBL in these patients was 1100 mL, 1600 mL, 2000 mL, 2500 mL, and 4000 mL. The authors concluded that perioperative balloon occlusion of the hypogastric arteries is an adequate option for reducing blood loss in patients with placenta accreta. 20
In a study by Bodner et al., 5 patients underwent prophylactic temporary balloon occlusion, followed by cesarean section, transcatheter embolization of the iliac arteries, and hysterectomy. 21 Twenty-two patients had cesarean hysterectomies without endovascular intervention. In this study, there was no significant difference in EBL or volume of fluids and red blood cell units replaced. 21
In a case-control study by Shrivastava et al., prophylactic intravascular balloon catheters did not benefit women with placenta accreta. 22 In this study, 19 women had balloon catheters and hysterectomies, while 50 women had only hysterectomies. There was no significant difference in EBL, transfused blood products, operative times, or postoperative hospital days. 22 As noted, there are no definitive data recommending or discouraging prophylactic balloon occlusion of the hypogastric arteries in placenta accrete; however, balloon occlusion is a tool that can be utilized.
About 10 years ago, some investigators advocated the injection of a Gelfoam slurry into the occlusion balloon catheters immediately after cesarean-section delivery. *
Conclusions
As this clinical case illustrates, and based on a review of the literature as outlined above, percutaneous, minimally invasive image–guided interventional techniques may be used in complex obstetric/gynecologic patients. Such techniques may be primary therapy (e.g., UAE for women with symptomatic fibroids) or used to assist the obstetric/gynecologic team during surgery. It is important to recognize the importance of a multidisciplinary approach to the treatment of such patients.
Footnotes
Acknowledgments
The authors thank all those individuals involved in the care of their patient.
Author Disclosure Statement
None of the authors have any relevant conflicts of interest to disclose. No funding was received for this project. This project has not been presented at any meetings. An institutional review board/ethics committee ruled that approval was not required for this study.
*
Personal communication with Anthony C. Venbrux, MD. The George Washington University Medical Center, Washington, DC, February 1, 2016.