
Abstract
Abstract
Background:
Hysterectomy is one of the most common female gynecologic surgeries. However, this surgery poses a risk for postoperative vaginal vault granulation, bleeding, infection, and dehiscence, which increases with patient comorbidities. These complications prolong recovery significantly and are the most common causes of postsurgical hospitalizations. Placental tissues have a long history of use for both wound treatments and surgical procedures. The benefits of placental tissues are attributed to their anti-inflammatory, antifibrotic, and antimicrobial properties. Advances in tissue preservation have led to the development and commercialization of this tissue for on-demand applications, including umbilical and amniotic grafts. This case report presents the first known use of viable cryopreserved umbilical tissue (vCUT) in a laparoscopic hysterectomy. The goals of this article are to assess safety and minimize risk for postoperative complications.
Case:
A 36-year-old female (gravida 0, para 0) with polycystic ovaries, insulin resistance, and recurrent, stage 4 endometriosis underwent an ovarian-sparing laparoscopic total hysterectomy. After removal of her uterus and cervix, vaginal cuff closure was augmented with vCUT.
Results:
Six weeks postoperatively, this patient had no granulation tissue, serosanguinous fluid formation, bleeding, odor, or pain. She did not report any other emergent events through 6 months post-op.
Conclusions:
This case report demonstrated the safety and proof-of-concept of vCUT use in patients who are at high risk for posthysterectomy surgical complications.
Introduction
H
This article describes the results of a laparoscopic total hysterectomy augmented with viable cryopreserved umbilical tissue (vCUT, Stravix,® Osiris Therapeutics, Inc., Columbus, MD) in a patient with multiple risk factors for vaginal cuff complications. vCUT is composed of human umbilical amnion, Wharton's jelly, and 2 layers of native umbilical cord tissue. The proprietary cryopreservation technique used for processing of vCUT is known to retain all components of fresh placental tissue (structural matrix, growth factors, and viable cells, including adult mesenchymal stem cells. 6 These unique components as well as favorable handling properties of the tissue make vCUT an ideal adjunct for standard vaginal cuff closure in high-risk patients undergoing hysterectomy.
Case
A 36-year-old female (gravida 0, para 0), with a body mass index of 40, a long smoking history, polycystic ovaries, and prediabetic insulin resistance, presented with pelvic pain, dyspareunia, and dysmenorrhea due to recurrent, stage 4 endometriosis. She had undergone previous conservative treatments for her endometriosis and infertility, including several laparoscopic surgeries for dense adhesions around her uterus and cul-de-sac, as well as a previous cervical procedure that had left her cervix and lower uterine segment distorted with scar tissue. All recent Papanicolaou test results were within normal limits.
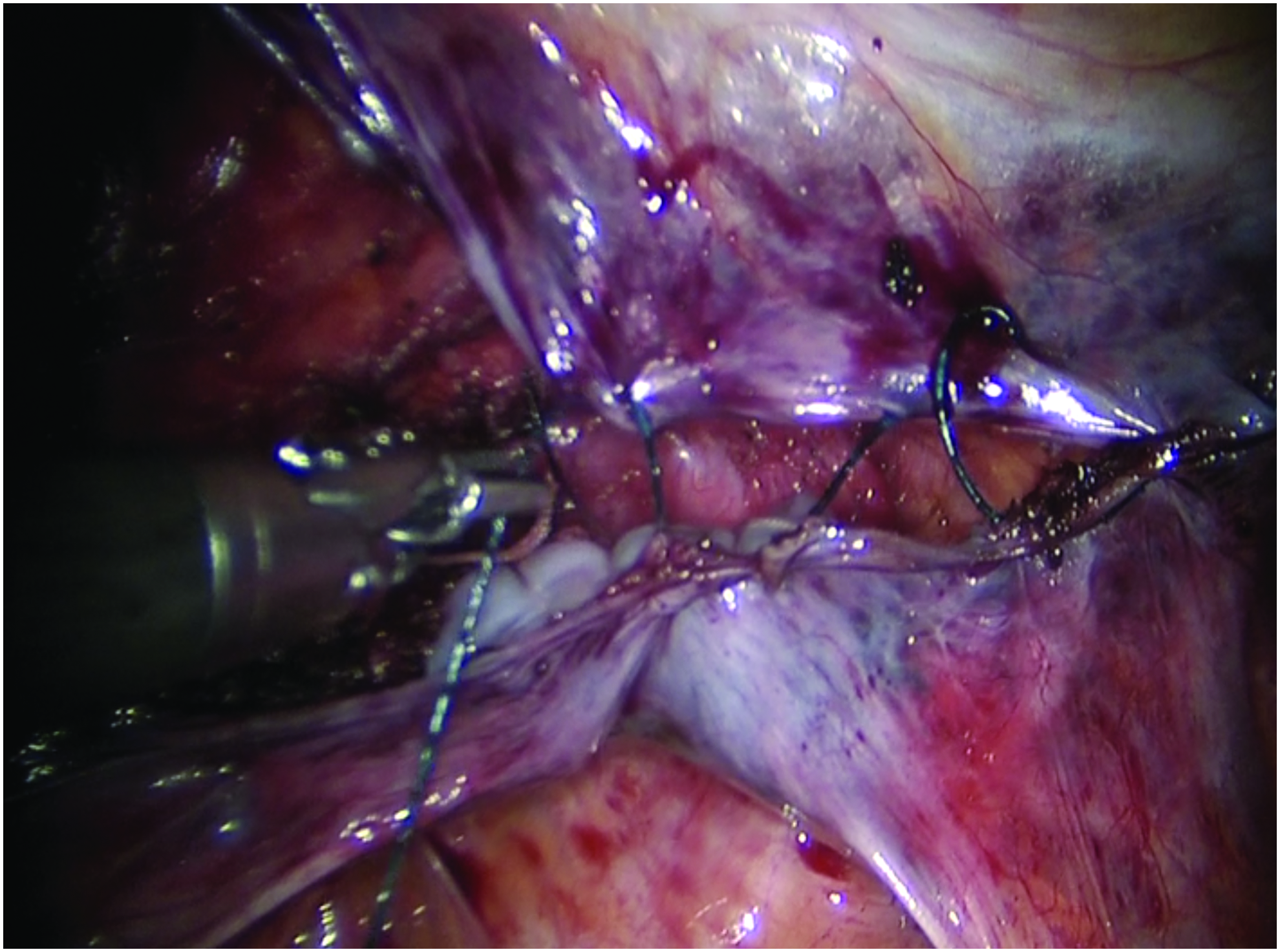
Due to her persistent endometriosis and chronic pain, this patient agreed per a physician recommendation to undergo a laparoscopic, robotic-assisted total hysterectomy with ovarian preservation. Care was taken to dissect the vaginal cuff away from the bladder and rectum, allowing room for a 2-layer closure without “bunching” the tissue. The first layer of the vaginal cuff was closed with a 0-Vicryl® suture (Ethicon Inc., Somerville, NJ) through the vaginal mucosa, ensuring close approximation of the edges. The second layer was also closed with a 0-Vicryl suture into which vCUT was incorporated in an imbricating fashion, with the Wharton's jelly side facing toward the vaginal cuff (Fig. 1). This ensured that vCUT would cover the vaginal cuff evenly. Finally, the peritoneum was closed over the vaginal cuff (Fig. 2).

Incorporation of viable cryopreserved umbilical tissue into second layer closure of vaginal cuff in imbricating fashion. Color images available online.
Closure of peritoneum over vaginal cuff with viable cryopreserved umbilical tissue incorporated. Color images available online.
Results
At a 6 week postoperative follow-up, there was no vaginal discharge, bleeding, or odor, and the patient reported no problems. No serosanguinous-fluid formation, scabbing, granulation tissue, or signs of graft rejection were noted. The patient reported minimal-to-no pain during recovery and did not request additional pain medication beyond the standard postoperative prescription. For these reasons, she was given permission to resume normal physical and sexual activities. The patient did not report any other emergent events or complaints 6 months postoperatively.
Discussion
To the best of the current authors' knowledge, this is the first report of umbilical tissue used in vaginal cuff closure during hysterectomy. Although the patient described here was at higher risk for vaginal cuff complications—particularly vaginal vault granulation—she did not experience any of these events after vCUT was applied.
Vaginal vault granulation is the growth of excessive scar tissue at the blind end of the vagina after cervical removal. Depending on the technique applied, this occurs in 10%–34% of total hysterectomies, and can lead to impaired healing of the vaginal cuff and delayed return to normal activity due to excessive discharge and postcoital bleeding.1–3 This granulation is commonly treated postoperatively by cauterization with silver nitrate, although this treatment can be painful for the patient, is not always successful, and could still delay healing, as the granulation is addressed only after developing. In addition, friable granulation and discharge is often accompanied by bacterial infection. Infection is the main cause of vaginal odor, necessitates antibiotic treatment, and increases the likelihood of a subsequent vaginal yeast infection.
Fresh amniotic tissue has been used in gynecologic surgery for decades to promote regenerative processes. 7 For example, application of fresh amnion grafts was shown to improve uterine cavity length significantly and reduce adhesion formation by 50% in women with Asherman's syndrome who were undergoing hysteroscopic lysis of intrauterine adhesions. 8 However, in routine practice, fresh tissue is not available on demand and, even if collected, has a short storage time that is not sufficient to complete required donor– and tissue–safety testing.
To overcome these limitations, different methods of tissue processing have been developed, including cryopreservation. Certain methods of cryopreservation—such as vCUT used in the current case—retain of all of the components of fresh tissue, including extracellular matrix proteins, growth factors, and viable cells. Dehydrated amnion/chorion membrane has been used in robotic laparoscopy for pelvic pain to prevent reformation of adhesions. 9 However, the thickness (1–3 mm) and handling properties (conformable and suturable) of vCUT are more appropriate for hysterectomy, and, unlike dehydrated tissue, vCUT retains all components of the native tissue, including viable cells. Thus, vCUT was selected for use in this case. Other clinical studies have also investigated the effects of stem-cell injections to treat a variety of gynecologic conditions, such as stress urinary incontinence. 10
In addition to this case, vCUT has been used to augment repair in rectovaginal fistulas and Achilles tendon rupture.11,12 In the example of fistula repair, vCUT was utilized due to the complex and high-risk nature of the case. Five failed surgical interventions for a perianal fistula resulted in a rectovaginal fistula with a 5-mm anterior defect within the anterior midanal canal. vCUT was placed on top of the anal mucosa and on the inner vaginal mucosa, and, 3 months postoperatively, the fistula repair remained intact and the perineal wound had healed completely. 11
Conclusions
This case report demonstrated the novel adjunctive use of vCUT in laparoscopic hysterectomy. This single case report described how the patient recovered with no granulation tissue, infection, or other vaginal cuff–related complications. Further studies are required and are ongoing to assess the benefit of vCUT application in hysterectomy fully.
Footnotes
Author Disclosure Statement
No competing financial conflicts of interest exist. Dr. Hesp was a full-time employee at Osiris Therapeutics while this case was treated and assisted with writing and editing this article.