
Abstract
Abstract
Objectives:
This survey was conducted to examine variations in practice for selecting women with postmenopausal bleeding (PMB) in the United Kingdom for hysteroscopy and endometrial biopsy. A secondary objective was to drive future research to improve clinical effectiveness.
Materials and Methods:
An online anonymous questionnaire was sent to British Society for Gynaecological Endoscopy and British Gynaecological Cancer Society members regarding their current practices for selecting women with PMB for hysteroscopy and endometrial biopsy. A reminder was sent to nonresponders prior to the end of the study. Quantitative and qualitative analysis were performed.
Results:
Three hundred society members responded. The minimum endometrial thickness (ET) necessitating an endometrial biopsy varied among respondents from 3 mm to 5 mm. Twenty-five respondents, however, said that endometrial biopsy was always performed regardless of ET. Of the 53% of respondents who had a cutoff ET to indicate a need for hysteroscopy, there was significant disparity, with cutoffs varying between 3 and 12 mm. A significant majority of respondents suggested implementing an accreditation process for scanning and hysteroscopy in patients with PMB to improve clinical effectiveness.
Conclusions:
There is wide variation in patient selection protocols for hysteroscopy and endometrial biopsy after an initial assessment of the endometrium by ultrasound (US). There is an urgent need for further study to clarify which patients require diagnostic hysteroscopy and/or endometrial biopsy in addition to US as a part of the investigation for PMB. This research, however, should preferably be conducted only after nationally defined standards for gynecology scanning are accepted. (J GYNECOL SURG 34:197)
Introduction
E
Depending on the ET cutoff chosen, a greater or lesser proportion of patients require further testing, including endometrial biopsy2–4,9 and/or hysteroscopy. This decision has resource implications and to hysteroscope everyone is incompatible with the principles of prudent healthcare. 7 This study was conducted to gain an understanding of the variation in clinical practices regarding hysteroscopy for post-menopausal bleeding (PMB) and to identify potential reasons behind these variations. Another aim was to identify current clinical governance practice and clinical effectiveness in PMB clinics, with the idea that the findings could help to make progress in service improvement in PMB management.
Materials and Methods
In 2016, an online questionnaire, organized and distributed through Survey Monkey, was sent to the BSGE and British Gynaecological Cancer Society (BGCS). The survey was sent to United Kingdom members and only those who were directly involved in the investigation and management of PMB were able to respond. These two societies encompass almost all clinicians in the United Kingdom who treat patients with PMB who are referred through rapid-access clinics. The questionnaire was designed with the help of gynecologic oncologists and non-oncology gynecologists who were involved in managing PMB and endometrial malignancy.
To ensure the highest possible response rate, a reminder was sent to all members before the end of the study. Responses were designed to allow for selection of multiple answers and choices. Responders were also able to comment in free text. There was one open question at the end of the survey. Responses were collated by the survey platform and analyzed manually with descriptive statistics. Free-text responses were coded qualitatively by common keywords or themes and tabulated further. A copy of the survey is in Appendix 1. The questionnaire was anonymous and self-administered to protect confidentiality. There was no direct patient involvement in this study.
Results
A total of 300 responses were received. Given the overlap between the two society memberships and the unknown proportion of members who are directly involved in PMB services, it was impossible to define a response rate. Of 300 responses, 184 (61%) were from consultants, 39 from nurse–practitioners, 77 from trainees, fellows, and staff grade doctors (Table 1). Forty-seven percent of respondents reported using a 4-mm cutoff on TVUS for performing an office-based Pipelle biopsy®; 18.6% reported using an ET of ≥5 mm as the threshold; and 8.5% indicated that they always performed endometrial biopsy regardless of ET value.
Participants were asked to specify particular indications for hysteroscopy in addition to blind endometrial biopsy when endometrial thickness was more than their selected cutoffs. The indications for hysteroscopy included risk factors, for example, recurrent PMB or use of tamoxifen. Other indications mentioned included fluid in the cavity and suspected endometrial polyp on TVUS (Table 2). Ninety-eight respondents (35.1%) reported that they perform hysteroscopy regardless of endometrial findings on ultrasound whenever an endometrial biopsy was required. Seventeen respondents indicated hysteroscopy was done only when an endometrial polyp was suspected. One hundred and fifty-three (51%) respondents specifically mentioned that they have a local protocol for endometrial thickness cutoff for hysteroscopy in addition to blind endometrial biopsy; however this cutoff varied from 3 mm to 12 mm (Fig. 1).
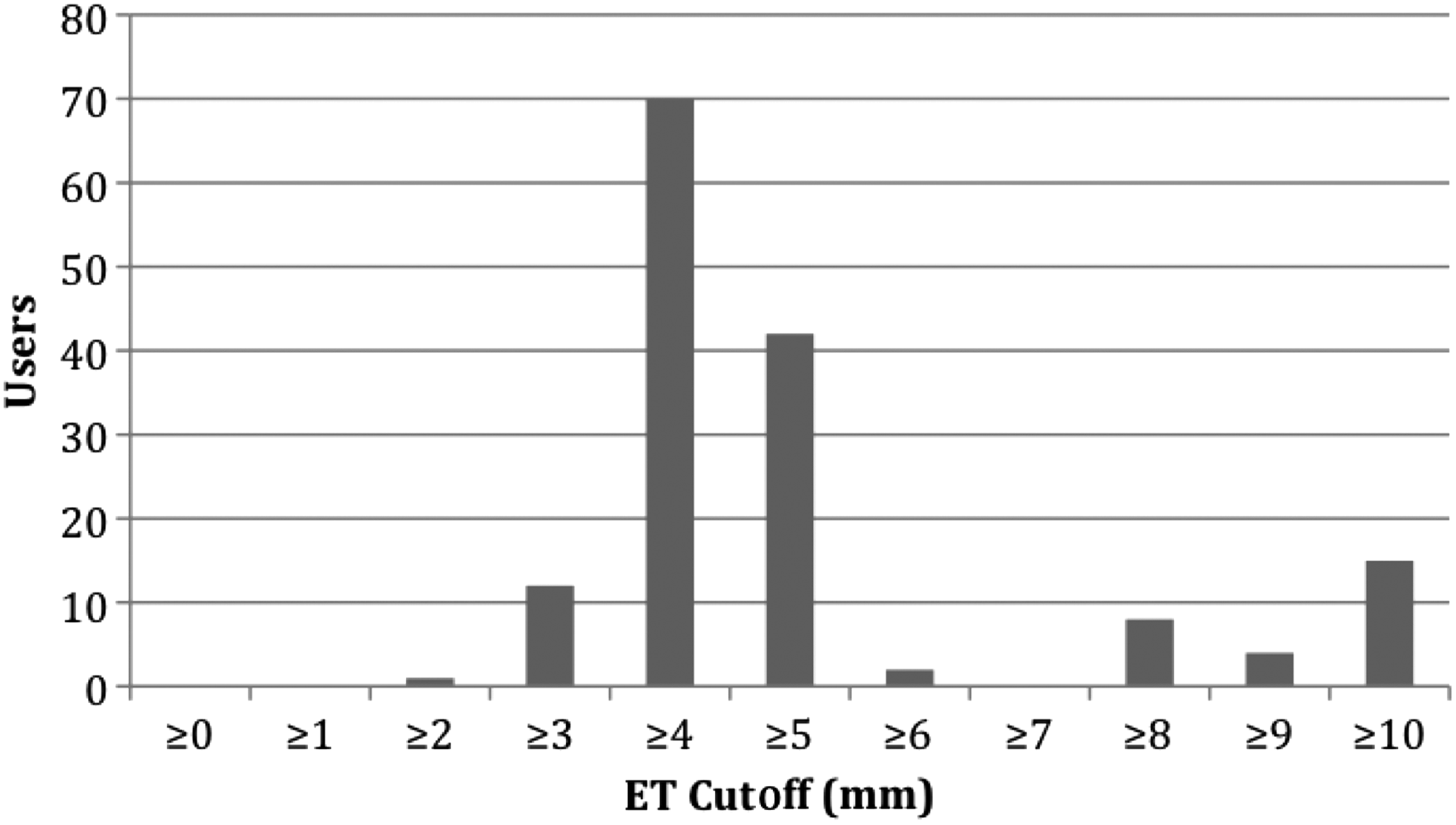
Endometrial thickness (ET) cutoff values for hysteroscopy in addition to endometrial biopsy.
PMB, postmenopausal bleeding; TVUS, transvaginal scan.
In the majority of units, scanning for PMB is performed by a mixture of sonographers (with radiographer training), and clinicians (gynecologists and gynecology nurse–practitioners). More than 70% of respondents indicated that scans for PMB are performed by sonographers with an interest in gynecology (Fig. 2), while 25% of respondents reported that scans in their unit are performed by non-specialist interest sonographers. Only 20.3% of participants reported that audits and surveys were completed in their units within the last 24 months to assess the quality of scanning. Thirty-four of the 53 individuals who reported quality-assurance systems commented on their outcomes of clinical audit.

Distribution of persons performing scans for postmenopausal bleeding.
The vast majority of respondents suggested different ways of improving clinical effectiveness in PMB investigations. Those suggestions include improving scanning quality, introducing standards for gynecology scanning and an accreditation program for scanning and/or hysteroscopy as a way forward. Sixty-four percent of respondents indicated that scanning accreditation for gynecology scanning would be a way to improve clinical effectiveness, followed closely by 61% who reported a need for regular audits on hysteroscopy/histology outcomes (Table 3). The majority of free-text responses were related to scanning, ranging from age and maintenance of equipment to variability of training and qualification for both scanning and hysteroscopy.
PMB, postmenopausal bleeding; IETA, International Endometrial Tumor Analysis; SIS, saline infusion sonohysteroscopy.
Discussion
This survey highlighted variations among respondents on patient selection for invasive investigations in women with PMB. Timmermans et al. 8 investigated the sensitivities of various ET cutoffs in the diagnosis of endometrial cancer and found that 3 mm had a high sensitivity of 98%, while 4- and 5-mm cutoffs had lower sensitivity (95% and 90%, respectively), compared to the previously reported 96% sensitivity for 5-mm ET reported by Smith-Bindman et al. 5 In 2002, in a meta-anlysis Gupta et al. 6 concluded that a negative result ≤5 mm measuring both endometrial layers rules out endometrial pathology with good certainty. Based on these and other meta-analyses, TVUS, followed by office-based blind aspiration endometrial sampling, became the accepted screening methods for PMB according to many national guidelines.5–8 Hysteroscopy adds further value by identifying localized pathologies such as endometrial polyps. The current study highlighted the wide variation in patient selection for hysteroscopy before and/or after endometrial biopsy, which is a significant cause for concern for healthcare providers.
This is the first to report this wide variation in the practice of endometrial sampling and hysteroscopy for the investigation of patients with PMB in the United Kingdom. This variation possibly reflects the lack of prospective studies regarding the identification of patients with PMB who would benefit from hysteroscopy in addition to an endometrial biopsy. The survey respondents were current clinicians involved in the care of women with PMB. This study did not identify a number of people who may currently practice but who did not respond or who are not members of the two societies.
The main reason for hysteroscopy in patients with PMB is to identify focal pathology and to direct the endometrial biopsy. Endometrial polyps have been shown to be the single most important risk factor for recurrent PMB, 10 and the risk of endometrial cancer is higher when postmenopausal women present with bleeding in the presence of endometrial polyps.11–15 The risk of premalignant or malignant polyps is higher in women presenting with PMB, compared to asymptomatic postmenopausal women.13–16 When endometrial polyps or focal pathology is present, outpatient blind biopsies of the endometrium are not representative,17,18 resulting in benign histology with delay in diagnosis of endometrial malignancy. These findings are significant, as endometrial polyps can be an early focus of hyperplasia or adenocarcinoma.
Two-dimensional (2-D) TVUS detection of endometrial polyps varies significantly,4,19 depending on sonographer experience and patient endometrial characteristics especially in patients with PMB. The International Endometrial Tumor Analysis (IETA) 20 group developed a consensus statement on terms and definitions to predict the risk of different endometrial pathologies. The current survey indicated that the IETA description is not widely applied in the United Kingdom.
Failure to have higher positive predictive value for detection of endometrial polyps by 2-D TVUS and performing hysteroscopy in a large proportion of patients has significant cost implications for health services. Saline infusion sonohysteroscopy (SIS) is superior to TVUS alone, and the introduction of SIS can increase positive and negative predictive values for endometrial-polyp detection.21,22 SIS is not practiced widely in the United Kingdom, partly because TVUS for PMB is performed by nonclinicians in many units due to a lack of dedicated sonographers and/or clinicians with skills to perform saline sonography available within the National Health Service (NHS).
Conclusions
As a nation with an increasingly aging population and an obesity epidermic, the United Kingdom faces growing numbers of patients presenting with PMB and malignancy. Approximately 60% of endometrial adenocarcinoma presents at an early stage. A clinically effective investigation based on evidence should enable clinicians and their patients to avoid both unnecessary invasive tests as well as delays in diagnosis and treatment. Hysterectomy with bilateral salpingectomy is the treatment of choice for patients diagnosed with early stage endometrial adenocarcinoma and is curative. Thus, early diagnosis avoids costly additional adjuvant therapy, such as brachyradiotherapy, 14 making efficient screening of women with PMB cost-effective and truly “prudent healthcare.”
The results of this survey have implications for future clinical guidelines and research. The wide variations in both the practice of endometrial biopsy and the current indications for hysteroscopy are inappropriate. The authors strongly recommend further studies on the cost-effectiveness of SIS for postmenopausal patients. It is time for an accreditation program for “scanning for PMB”—like the British Society for Colposcopy and Cervical Pathology accreditation system for colposcopy—which will improve clinical effectiveness, clinical governance and save money for the NHS.
Footnotes
Acknowledgments
The authors are grateful to colleagues who have responded to the study questionnaire. Thanks are also extended to both the BSGE and BGCS for granting permission and access to their members. The authors would also like to acknowledge input from Thierry van den Bosch, MD, PhD a gynecologist in UZ Leuven.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1: Questionnaire
CCT, Certificate of Completion of Training; IETA, International Endometrial Tumor Analysis.