
Abstract
Abstract
Background:
Primary cervical malignant melanoma (MM), a very rare disease of the lower genital tract, has a poor prognosis. The diagnosis remains a challenge and the management is not standardized.
Case:
A primary cervical MM developed in a woman, age 44, who presented with menorrhagia and intermenstrual bleeding. A biopsy of a 5-cm, pigmented, exophytic cervical mass was reported locally as an undifferentiated cervical stromal sarcoma. The case was reviewed by a central gynecologic oncology multidisciplinary team (MDT). Additional immunohistochemistry testing revealed a primary cervical MM, which was staged as International Federation of Gynecology and Obstetrics (FIGO) 1B2. The patient underwent open radical hysterectomy, bilateral salpingo-oophorectomy and bilateral, pelvic lymph node dissection, with no adjuvant treatment.
Results:
She remained well at a follow-up in the last 20 months, with no evidence of recurrence.
Conclusions:
Primary cervical MM may be included in the differential diagnosis of premenopausal women diagnosed with cervical cancer. Central MDT review is key for making an accurate diagnosis of such a rare entity. Surgical intervention without any adjuvant treatment may be applied in FIGO stage 1 cases if satisfactory clear margins can be achieved and if there is no nodal involvement. Only in cases of BRAF or KIT mutations would adjuvant immunotherapy be considered. (J GYNECOL SURG 34:209)
Introduction
M
Following the discovery of melanocytes in 1959, primary cervical (uterine) MM (PCMM) has been recognized as a separate, even rarer entity of the female lower-genital tract. The treatment is not yet standardized and the overall prognosis is very poor.
When the MM is operable, radical hysterectomy with bilateral pelvic lymphadenectomy (BPLND) is considered to be the standard treatment. 3 Nevertheless, due to the rarity of the disease, there is a paucity of published information about optimal management. Herein, is a report of a rare case of early stage PCMM for which the patient underwent surgical management without any adjuvant treatment.
Case
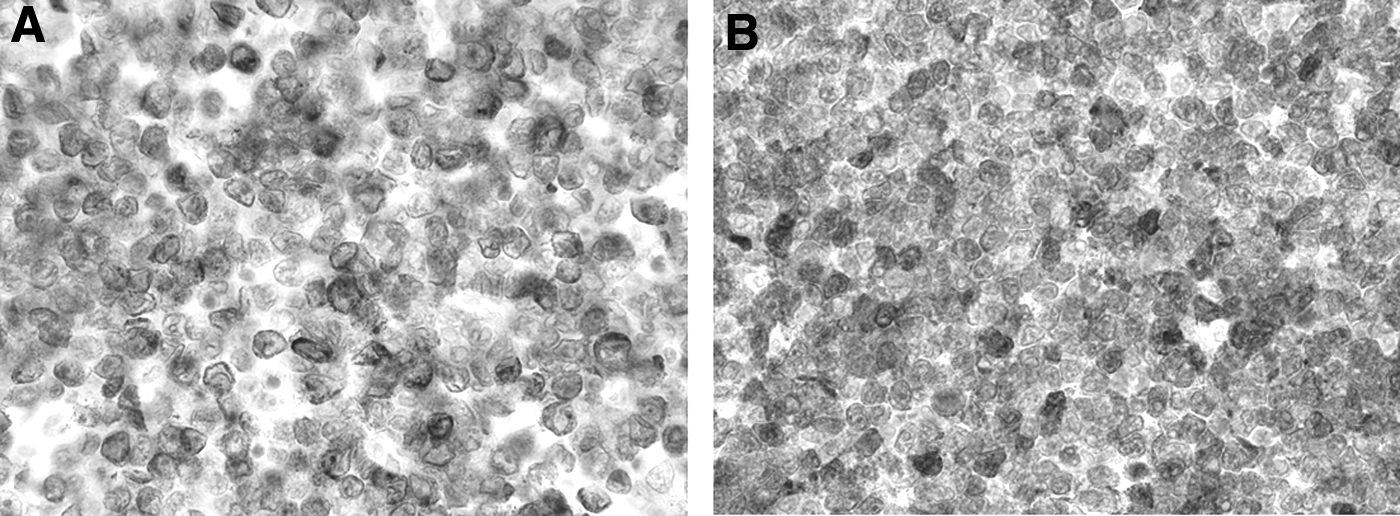
A 44-year-old patient presented with a 7-month history of menorrhagia, intermenstrual bleeding, and abdominal bloating. Gynecologic examination revealed a 5-cm, pigmented, exophytic cervical mass. Subsequently, a colposcopy-guided biopsy was performed and a local pathology review revealed cervical stromal infiltration by a poorly differentiated malignant tumor. It was composed of cells with a high nuclear:cytoplasmatic ratio and occasional prominent nucleoli, which was suggestive of an undifferentiated cervical sarcoma. The case was discussed further by a central gynecologic oncology multidisciplinary team (MDT). Immunohistochemical stains for AEI/3, desmin, and HMB45 were negative. There was positive staining with CD10 and an occasional cell was positive for CD56 and S100. The background lymphocytes were positive for leukocyte common antigen. The appearances and immunohistochemical profile were consistent with cervical melanoma (Fig. 1).

Cervical melanoma.
A full-skin survey revealed no evidence of any lesions of concern, and a diagnosis of PPCM was made. Subsequently, magnetic resonance imaging showed a 40 × 30 × 46–mm intermediate-signal mass filling the lower aspect of the uterine cervix with a suspicion of a stromal breach on the left side (Fig. 2). The uterine corpus, the parametria, both ovaries, and both fallopian tubes appeared to be normal. Neither pelvic nor para-aortic lymphadenopathy was shown. Staging computed tomography (CT) scans of the patient's abdomen and thorax were negative for metastases. With a clinical diagnosis of International Federation of Gynecology and Obstetrics (FIGO) stage 1B2 PPCM, the gynecologic and melanoma MDT recommendations were for surgical treatment.

T2W magnetic resonance image of the pelvis showing a large, exophytic, well-circumscribed cervical mass. The stromal ring appears to be intact (sagittal view).
Results
The patient underwent a radical hysterectomy, bilateral salpingo-oophorectomy (BSO), and BPLND. Final histology testing confirmed the presence of a 45 × 32–mm cervical melanoma that had been excised completely, with the nearest margin of 9 mm × 11 mm. There was no evidence of lymphovascular space invasion. None of the 19 retrieved pelvic and para-aortic lymph nodes showed any evidence of malignancy. The main tumor showed strong diffuse positive immunoreactivity with Melan-A and patchy positive immunoreactivity with S100 and HMB 45 respectively (Fig. 3). A minute focus of melanoma was seen in a subepithelial location within the vaginal mucosa, which was interpreted as a focus of metastatic MM. Elsewhere within the vagina, very focally, there were features suggestive of in situ disease. Confirmatory immunohistochemistry was also performed in these areas. Targeted mutation analysis of BRAF codon 600 and NRAS codons 12, 13, 61 by pyrosequencing did not detect any mutations.
Cervical melanoma.
Following both gynecologic oncology and melanoma MDT discussions and given the absence of a BRAF mutation, the patient was deemed unlikely to benefit from BRAF-inhibitor adjuvant treatment. Therefore, a decision was made for surveillance. The patient had an uneventful recovery. She has been on close, 3-monthly surveillance follow-up. Examinations and CT scans have yielded normal results throughout this surveillance, and she remained well with no evidence of recurrence 20 months after the initial diagnosis.
Discussion
PPCM is considered to be a rare entity, particularly in postmenopausal women of the sixth and seventh decade.3–6 PPCM commonly is asymptomatic unless it becomes ulcerated and infected, causing vaginal bleeding or discharge. The main presenting symptoms include vaginal bleeding or discharge, abdominal pain, dyspareunia, and postcoital bleeding.7–9 Weight loss and hematuria are uncommon but are more prominent with advanced cases. 10 Diagnosis is based on digital examination, while colposcopy can sometimes be helpful for identifying small purpuralike areas. 11 Macroscopically, PPCM manifests with either an exophytic polypoid mass or multiple-plane or ulcerated nodules. Pigmented lesions are generally dark and sometimes reddish. 12
This case report highlights the importance and value of the central MDT review for the diagnosis following a biopsy of such a rare entity. Histologic features of PPCM include spindle-shaped cells, epithelioid cells, and, rarely, round or clear cells.13,14 As melanin is absent in 45% of such lesions, the diagnosis may be extremely difficult to make. The differential diagnoses include poorly differentiated squamous-cell carcinoma, adenocarcinoma, rhabdomyosarcoma, and stromal sarcoma. 3 In the current case, the pathology was initially reported locally as an undifferentiated sarcoma.
Prior to referral for central management, further immunohistochemistry testing was requested. Immunohistochemical staining for S100 and HMB453,11 can assist with making a diagnosis (Fig. 1). The PCMM diagnosis was established once the metastasis from a primary cutaneous or ocular melanoma was ruled out. Generally, according to Norris and Taylor's recommendations, the following four criteria should be fulfilled for the final diagnosis of a PCMM:
Presence of melanin in the normal cervical epithelium Absence of melanoma in other body areas Evidence of junctional changes in the cervix Metastases according to the pattern of cervical melanoma.
15
Correct diagnosis in the current case altered the management plan dramatically. The patient was offered surgical management as opposed to the chemoradiation that had been recommended following the initial pathology opinion.
The staging of cervical MM remains debatable. PPCM usually follows loco-regional spread rather than lymphatic or hematogenous dissemination.16,17 In either case, PPCM follows the pattern of cervical carcinoma. 18 Despite tumor thickness (Fig. 4) being the best prognostic factor—which would warrant a staging system based upon this parameter—the FIGO staging system has been widely applied, given the similar pattern of spread, compared to that of cervical adenocarcinoma (Fig. 3). In addition, tumor thickness correlates better with the prognosis. 1

Schematic representation of the tumor element of TNM [T, size of the tumor; N, lymph nodes; M, metastasis] staging for cutaneous melanoma and International Federation of Gynecology and Obstetrics staging for 1B2 cervical melanoma.
To date, there has been little but a growing amount of literature regarding management of PCMM. In light of limited reported data, treatment recommendations vary, with no universally accepted standard of care as an optimal treatment modality. Nonetheless, surgical management is the most frequent treatment intervention, including total hysterectomy and/or radical hysterectomy and BPLND without routine use of BSO. Wide local excision is rarely implemented. The choice between a less- or more-conservative surgical approach remains a challenge. Taking into account the grave prognosis of the disease, 3 some researchers recommend less-aggressive surgical management, usually advocating total hysterectomy and BSO.19–21
To add to the controversy, radical hysterectomy ensures that there are clean surgical margins and, given the similar pattern of spread with that of cervical adenocarcinoma, this approach could theoretically contribute to a better prognosis. The current authors favored radical hysterectomy over total hysterectomy, which was in line with the Yuan et al. study, which reported an improved overall survival for women undergoing radical hysterectomy, compared to total hysterectomy (66.8 months versus 19.5 months; p = 0.016). 22 The current authors also performed BPLND and para-aortic lymph node dissection routine practice although the rationale of nodal dissection remains debatable.20,23 Radical hysterectomy and BSO should be offered to women with PCMM, especially when the disease is in early stages.
There is no role for routine adjuvant therapy in women with early stage PCMM. Such tumors are considered to be radioresistant, and none of the chemotherapeutic agents has been proven efficient for reducing the likelihood of recurrences. The current authors suggest that adjuvant radiotherapy be considered when there are unsatisfactory surgical margins and parametrial and/or nodal involvement. Chemotherapy should be used in cases of advanced or recurrent disease. Dacarbasine seems to produce the best response rates, reaching up to 15%–20%. 3 Notably, the use of monoclonal antibodies appears to be promising. Trials using targeted antibodies against BRAF mutations (vemurafenib, dabrafenib), KIT mutations (imatinib), and inhibitors of MEC1 and MED2 (trametinib) have produced relatively good results for treating advanced-stage melanomas.24–27 In the current case, no BRAF mutations were identified; hence, no adjuvant immunotherapy was recommended.
Conclusions
This case report adds to the small, yet growing, literature on the rare entity of MM. Based on the current authors' experience, they propose that stage I PCMM be treated with a surgical intervention, consisting of radical hysterectomy, BSO, and BPLND, without any adjuvant treatment. Adjuvant immunotherapy could be considered only for cases with BRAF or KIT mutations. PCMM should be included in the differential diagnoses of women diagnosed with carcinoma of the cervix. Central pathology review is key in making an accurate diagnosis of such a rare entity, which will subsequently help decide the optimum treatment.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.