
Abstract
Abstract
Background:
Mesh erosion is a well-known complication after use of mesh for pelvic organ prolapse repair. The most common site of mesh erosion is the vagina. Nonvaginal mesh erosions into bowel and bladder are rare. Mesh erosion into the bowel can be a devastating complication with significant morbidity and could need multiple surgeries for repair and recovery. Mesh erosion presenting as thigh sinus-tract abscess is unusual and rare.
Case:
A 41-year-old female had rectosigmoid mesh erosion after laparoscopic sacrocervicopexy; this condition presented with a recurrent left sinus-tract thigh abscess. Rectosigmoid mesh erosion, with a thigh sinus-tract abscess was suspected on the basis of local and pelvic examination findings as well as ultrasonography findings. This case was managed by excision of the mesh with closure of the sinus tract, and bowel diversion and repair.
Results:
This patient was asymptomatic after 3 years of follow-up.
Conclusions:
Total excision of the mesh with repair of the bowel defect seems to be an appropriate treatment for patients with mesh eroding into the bowel. Sometimes bowel diversion (ileostomy or colostomy) is needed. Any unusual anorectal or gynecologic symptom should alarm the physician, and the possibility of mesh erosion should be suspected.
Introduction
P
Owing to more rapid recovery and less morbidity, the laparoscopic approach has dramatically increased in popularity and has been rapidly adopted by the urogynecologic community. To improve results obtained with native tissue usage, surgeons started using nonabsorbable synthetic mesh in pelvic floor surgery. In the last decade, due to a dramatic increase in incidence, mesh-related complications have received significant attention, including a report and warning from the U.S. Food and Drug Administration. 2 Mesh erosion is a well- known complication occurring in nearly 10% of procedures. 2 While mesh erosion into the vagina is by far the most common, rectal and other nonvaginal mesh erosions after laparoscopic sacrocolpopexy is rare. 3 This article reports on a unique late complication of laparoscopic sacrocervicopexy presenting as a left thigh sinus-tract abscess along with rectosigmoid mesh erosion.
P.P.G. was the surgeon. Written informed consent was obtained from the patient for publication of the images and other details. The retrospective observational nature of this report did not necessitate local institutional ethics committee approval.
Case
A 41-year-old multiparous woman (BMI-22) had undergone laparoscopic Shirodkar's sacrocervicopexy 4 with posterior colpoperineorrhaphy in 2011 for stage 3 uterovaginal prolapse and a moderate rectocele. One end of Mersilene® (Polyester, Ethicon, Sommerville, NJ) tape had been fixed to the anterior longitudinal ligament (Fig. 1A), then passed subperitoneally along the right pelvic wall between the two leaves of the broad ligament, and transfixed to isthmus posteriorly (Fig. 1B). The tape had been then passed posteriorly through the left broad ligament and taken out through the psoas loop on the left side (Fig. 1C). The tape had been finally fixed to the anterior longitudinal ligament after passing it beneath the sigmoid mesentery (Fig. 1D). The peritoneum had been closed over the tape with absorbable sutures. Postoperatively, she had intermittent pain in her left leg and left thigh region. However, magnetic resonance imaging (MRI) of lumbosacral spine with pelvis and both lower legs revealed normal findings. Yet, she continued to have intermittent pain in her left leg; this pain was managed with analgesics.
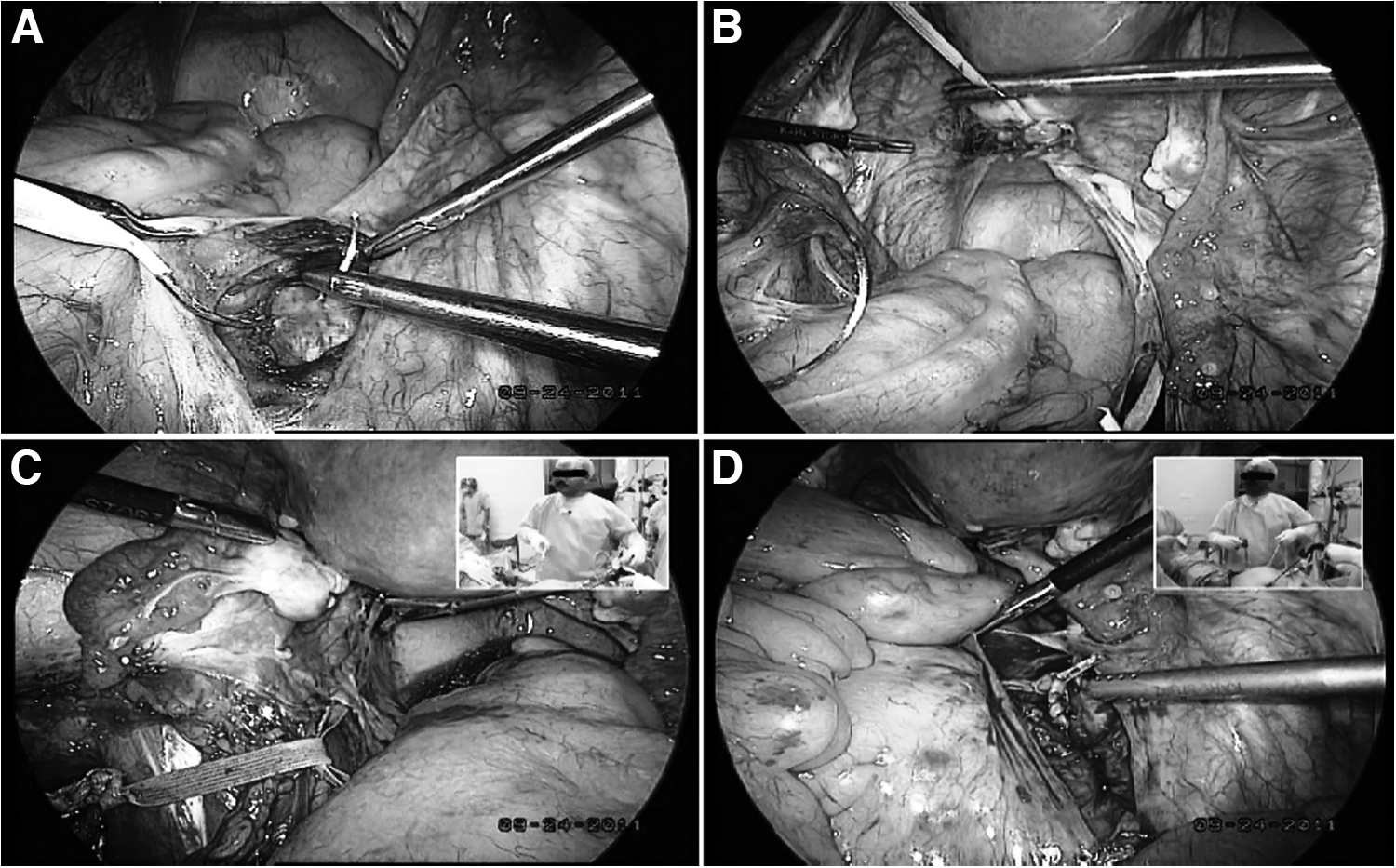
Shirodhkar's sacrocervicopexy.
Three years later, in 2014, she observed pus discharge from the lateral aspect of her left thigh. Incision and drainage of this left lateral thigh abscess was performed, and she was given a course of antibiotics. Despite this, the pus discharge persisted.
She presented again 3 months later. Per vaginal examination, there was tenderness on deep palpation in the left fornix. Ultrasonography (USG) of her left thigh revealed an ill-defined hypoechoic collection along the intermuscular planes of the lateral aspect of the upper one-third of the left thigh, with a tract of 1 cm width extending from the anterior superior iliac crest to the upper one-third of the thigh. There was also mild subcutaneous edema. Transvaginal sonography (TVS) showed that she had a normal uterus and right ovary but her left ovary could not be clearly imaged. A hyperechoic area was seen posteriorly at the isthmic region measuring 1.1 × 0.9 cm, suggestive of mesh, and another hypoechoic lesion measuring 1.9 × 1.5 cm. A provisional diagnosis of a pelvic abscess with a left lateral thigh sinus tract with the possibility of mesh erosion was made.
Total laparoscopic hysterectomy and bilateral salpingectomy with excision of the sinus tract abscess was planned. Dense omental adhesions to the posterior surface of the uterus, the left adnexa, and the rectosigmoid region were noted. The cul-de-sac was completely obliterated due to dense rectosigmoid adhesions to the posterior surface of the uterus (Fig. 2A), with inflammation and fibrosis at the tape attachment site. The left ovary and fallopian tube were also densely adherent to the lateral pelvic wall, rectosigmoid colon, and the inflamed area near the tape attachment. Adhesiolysis was performed with sharp and blunt dissection. The tape attachment to the posterior surface of the uterus was identified and traced posteriorly through the inflammatory and fibrosed area in the rectosigmoid colon up to the sacrum. The tape was incarcerated and was found eroding into the rectum (Fig. 2B). During dissection of the tape from the rectum, a defect of 1.5 cm was noted in the rectum (Fig. 2C), which was sutured laparoscopically with 2-0 polyglactin 910 suture material.
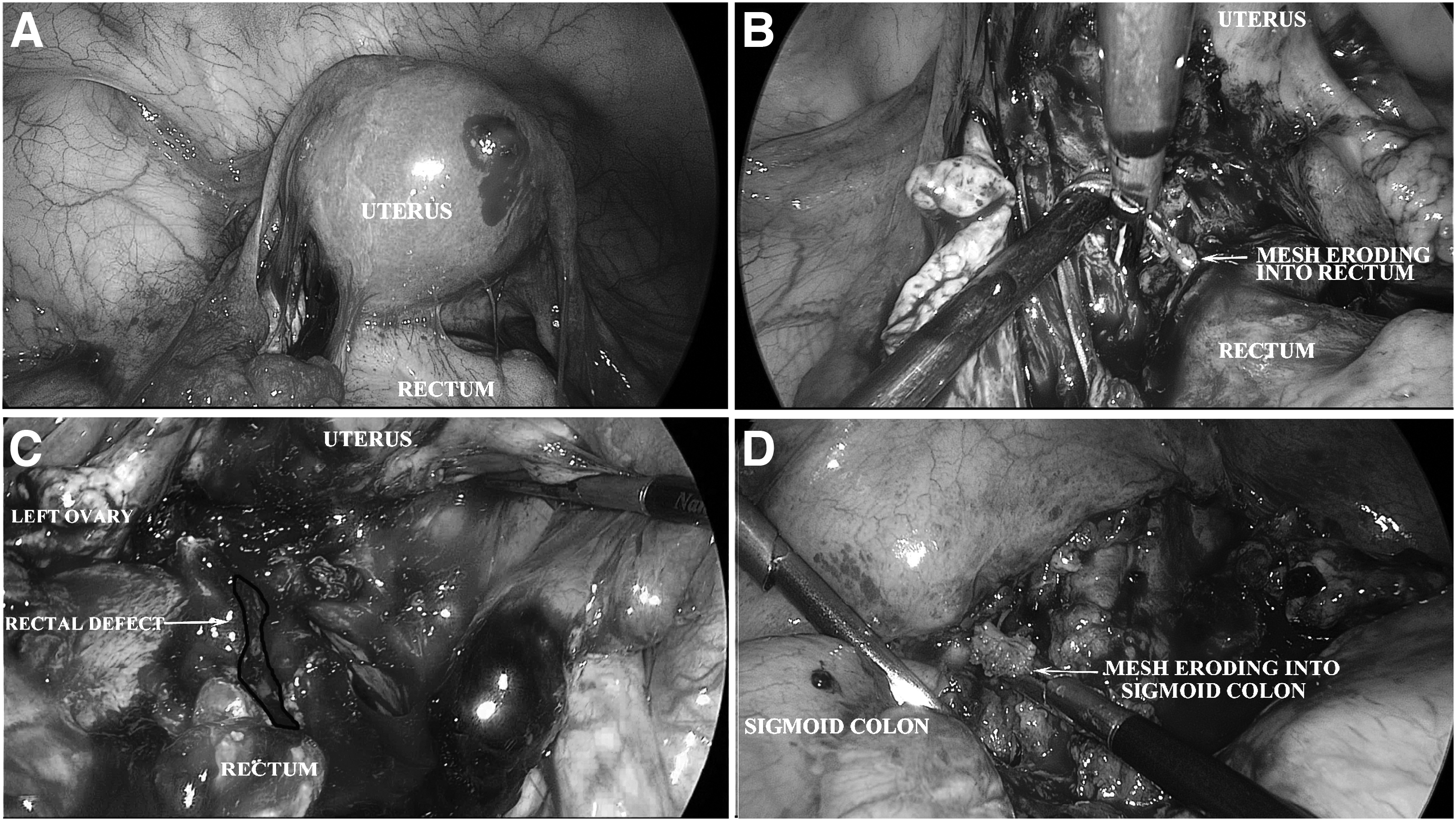
Hysterectomy and right salpingectomy, with a left salpingo-oophorectomy, were performed in a routine fashion. The sigmoid colon was found densely adherent to the tape and to the paracolic gutter, where the tape was eroding through the sigmoid colon (Fig. 2D). The psoas loop of the tape was traced left laterally behind the mesentery of the sigmoid loop, and was found to be firmly adherent to the sigmoid, lateral pelvic wall, and left paracolic gutter. Hence, the surgery proceeded to a laparotomy with a midline infraumbilical vertical incision. While releasing the tape, a small defect in the sigmoid colon was identified and closed with 2-0 polyglactin 910 suture material. The psoas loop and the rest of the Mersilene tape was removed, revealing the sinus-tract tracking to the lateral aspect of the left thigh, which was identified by injection of methylene blue into the tract. The abdominal opening of the tract was closed with multiple sutures and covered with omentum. Bowel diversion was done with a transverse colostomy with the assistance of a gastrointestinal surgeon. An intraperitoneal drain was kept in the pelvis.
Results
The patient was kept nil per orally with intravenous fluids support for 72 hours, after which, she was started gradually on oral intake. She was given broad spectrum antibiotics coverage for 7 days. The colostomy started functioning on the fourth postoperative day. The patient was taught and counseled about colostomy care and was discharged on the eighth postoperative day. She recovered well and the colostomy closure was performed after 3 months. Three years after this last surgical intervention, she remains asymptomatic with no signs of vaginal or rectal fistulae and no recurrence of pelvic floor descent.
Discussion
Laparoscopic sacrocervicopexy is an effective option for women with POP who desire uterine preservation. The mesh-erosion rate after laparoscopic sacrocolpopexy is reported to be 2.7%. 5 Vaginal mesh erosion has been reported in many cases after laparoscopic sacrocolpopexy and sacrocervicopexy, but cases of rectal or other nonvaginal exposures are limited in number. 3
The current patient presented with left thigh pain postoperatively and later presented with a left thigh abscess and pus discharge. Other clinical symptoms of rectal mesh erosion are pain, dyspareunia, dyschezia, rectal discharge, and hematochezia. 6 This erosion can also present with nonspecific anorectal or gynecologic symptoms, such as vaginal discharge and rectal mucous discharge, transanal passage, or protrusion of mesh. 7 Mesh erosion can present as a late complication after the primary surgery. 3 In the current case, the time to presentation was 3 years after the initial surgery.
The rectosigmoid mesh erosion with the thigh sinus-tract abscess in current case was suspected on the basis of local and pelvic examination findings as well as USG findings. MRI was performed to investigate the immediate postoperative pain after the initial surgery but not before the second surgery. The diagnosis was confirmed only after laparoscopy. Rardin et al. 8 reported a vaginal sinus-tract extending to the thigh with abscess formation after a midurethral sling was used. These researchers used MRI as a diagnostic modality. The various diagnostic modalities that can be used in cases of rectal mesh erosion are proctoscopy, colonoscopy, USG, computed tomography (CT) scanning, and MRI of the pelvis.3,6–8 Laparoscopy or surgical exploration is usually needed for conclusive evidence of mesh erosion and for excision of the mesh with repair of the defect.
In the current case, laparoscopic sacrocervicopexy had been performed, using Mersilene tape. Shirodhkar's sacrocervicopexy involved fixation of the long Mersilene tape at two sites, which had eroded in the rectum and sigmoid colon. Thus, not only the kind of mesh but the mesh load itself also predisposed this patient to mesh erosion. Mersilene is a permanent macroporous mesh with multifilament microporous components. The pore size of Mersilene tape is smaller than the typical diameter of a macrophage (10 μm) but larger than the diameter of bacterial cells (typically <1 μm). For this reason, synthetic materials with woven microporous multifilament structures have been criticized as potential bacterial havens, allowing bacteria to colonize where macrophages cannot reach. In abdominal sacrocolpopexies, Mersilene erosions have been reported in the range of 2.5%–4%. 9 Other risk factors associated with mesh erosion are transvaginal mesh placement, young age and obesity of the patient, and experience of the surgeon. 10
The current patient was managed by laparoscopy converted to laparotomy for complete excision of the mesh with closure of the sinus tract and a diversion colostomy. As reported cases of mesh erosion into the bowel are limited, there is no consensus on management of such complications. Some patients have been treated with transanal excision or ablation of the mesh. 7 However, patients with large mesh erosion leading to large bowel defects; mesh fixed to the sacral promontory; suspected sinus-tracts or fistulae; or need of any concomitant surgical procedures, such as hysterectomy, might need a laparoscopic or abdominal approach.3,11 In cases complicated by bowel perforation, bowel resection and repair—with or without bowel diversion (ileostomy or colostomy)—with assistance of a colorectal surgeon might be needed. 3
In the current patient, colostomy closure was performed 3 months after the mesh excision without any complications. She was asymptomatic at a 3-year follow-up. Balzzaro et al. 3 performed abdominal excision of mesh with rectal repair and a diverting colostomy, followed by colostomy closure 3 months later. Their patient was asymptomatic at a 4-year of follow-up. In patients with persistent symptoms after a mesh excision, pelvic and rectal examination with follow-up colonoscopy might be useful to ensure complete healing.
The precise cause or mechanism of mesh erosion is still unknown. Acute inflammation with or without concurrent infection, chronic inflammation due to an immune-mediated foreign body reaction or a mechanical cause (tight sutures causing local ischemia or direct pressure of mesh on adjacent tissues) can lead to perforation and erosion. 12 In the current case, inflammation with infection might have been the possible cause of the rectosigmoid colon mesh erosion and left thigh sinus-tract abscess. The kind of mesh (Mersilene tape) and the mesh load might have been the contributing factors.
Conclusions
Mesh implants used for POP repair are associated with a risk of mesh erosion. The most common location of such erosions is the vagina. While rare, bowel and other nonvaginal visceral mesh erosions are devastating complications with significant morbidity. Before the use of mesh, extensive counseling of patients by the healthcare provider and informed decision-making by the patient are vital. Surgeons who perform pelvic reconstructive surgeries with mesh augmentation should practice stringent aseptic precautions during mesh placement. An active search with careful evaluation of gynecologic or anorectal signs and symptoms as well as nonspecific symptoms, such as groin pain or recurrent thigh abscesses, should be performed during follow-up. Local treatment is seldom curative, partial or total excision of the mesh with repair of the bowel defect, if needed, with or without bowel diversion, might be required.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest or disclosures.