
Abstract
Abstract
Background:
Juvenile granulosa-cell tumors (JGCTs) are rare. Commonly, they are associated with hyperestrogenic features. However, these tumors rarely manifest with virilizing features and bleeding necrotic tumors. Sonographic similarities are common among juvenile granulosa-cell tumors and benign juvenile ovarian cysts.
Case:
A 20-year-old woman presented with acute anemia, abdominal pain, and a large pelvic mass that was diagnosed at surgery as a JGCT.
Results:
This patient had an unremarkable postoperative course. Histopathology testing revealed that she did have a JGCT. She was referred for an oncology consultation.
Conclusions:
Imaging findings in JGCT may resemble those of benign ovarian masses; thus, a high index of suspicion is required. JGCT should be included in the differential diagnosis when anemia is present. A thorough preoperative evaluation—including measurements of tumor markers (e.g., inhibin) and serum hormone levels (testosterone)—is warranted in order to characterize the lesion better and prepare the patient for optimal surgical staging.
Introduction
Juvenile granulosa-cell tumors (JGCTs) of the ovary are rare estrogen-secreting sex-cord–stromal tumors. These tumors usually present as features of hyperestrogenism. This article reports an unusual case of a JGCT presenting as anemia in a 20-year-old woman who was experiencing abdominal pain.
Case
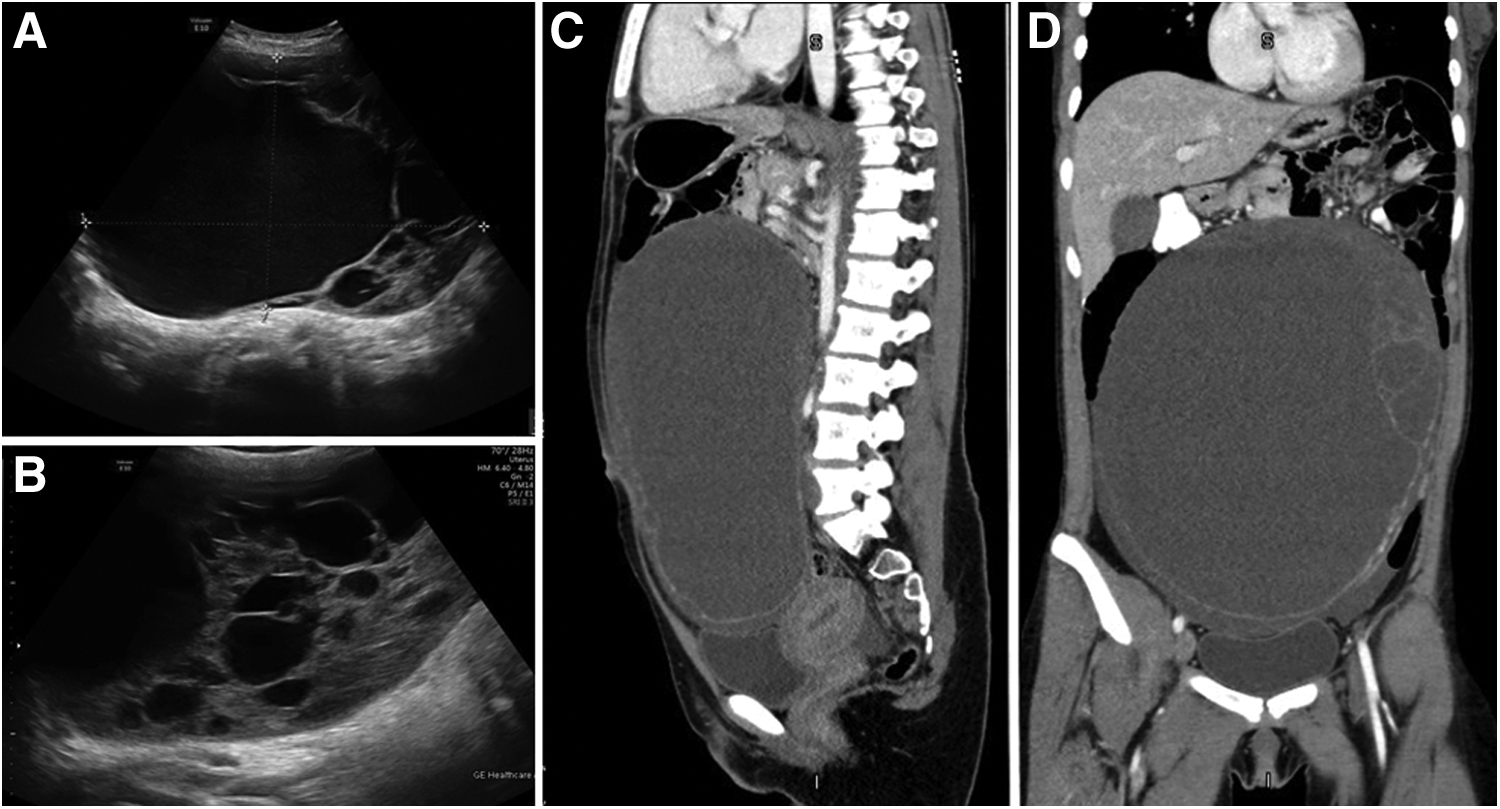
A virginal 20-year-old woman, without any previous medical history, was referred to an emergency room due to right upper abdominal pain lasting for 2 weeks and remarkable anemia of 7.0 g/dL. Her vital signs were normal. On examination, an epigastric abdominal mass was palpated, and notable signs of virilization, including facial hirsutism, were apparent. Her laboratory results were remarkable for a hemoglobin level of 6.7 g/dL and an elevated cancer antigen–125 level of 47.4 U/mL. Ultrasonography examination showed a large ovarian complex cyst with septations (Fig. 1A and B). Computed tomography examination showed a large complex cystic mass, measuring 27 × 12 × 22 cm, that was likely of ovarian origin (Fig. 1C and D). The patient was treated with 2 units of packed red blood cells and was admitted for surgery. During the surgery, a left ovarian cyst was revealed and aspirated with extraction of 2500 cc of bloody fluid, followed by its exteriorization and cystectomy. An intraoperative frozen section was apparently normal.
Results
This patient's postoperative course was unremarkable. A detailed histopathologic evaluation revealed a JGCT, and she was referred for oncologic consultation.
Discussion
JGCTs of the ovary are rare estrogen-secreting sex-cord–stromal tumors accounting for only 5% of granulosa-cell tumors. These tumors usually present as large solid-mass lesions. Most of the juvenile type tumors occur at a young age. 1 Although a JGCT is characterized by its ability to secrete estrogen and cause precocious puberty, its predominant manifestations are abdominal pain and distension, 2 whereas, in rare cases, this tumor presents with signs of virilization, 3 as in the current case. Virilizing tumors of the ovary are part of sex-cord–stromal tumors. Virilizing accounts for only 1%–2% of all ovarian tumors, and present with noticeable androgen and sometimes estrogen excesses of tumor-production origins. Virilizing tumors from the sex-cord family include Sertoli-Leydig–cell tumors, granulosa-cell tumors, and fibrothecomas. Most of these tumors are solid, are at an early stage at diagnosis, and are not associated with ascites.
Virilizing testosterone-producing JGCTs are extremely uncommon, occurring only in 2%–3% of cases of JGCTs. The most common presentations of virilizing JGCTs include amenorrhea, hirsutism, a deepening voice, clitoris hypertrophy, and acne.
In addition, granulosa-cell tumors can present with varying amounts of hemorrhage and necrosis inside the tumor mass, 4 as in the current case in which severe anemia was caused by massive bleeding into the necrotic mass.
Conclusions
JGCT is a rare entity that can present with features of a benign mass as in the current case. Imaging findings for JGCT can resemble those of a hemorrhagic corpus luteum or a simple mucinous cystadenoma. Thus, a high index of suspicion is required. Acknowledging the rarity of JGCT, it should be included in the differential diagnosis when anemia is present with a pelvic mass. Thorough preoperative evaluation—including measurements of tumor markers (e.g., inhibin) and serum hormone levels (e.g., testosterone)—is warranted in order to characterize the lesion better and prepare for optimal surgical staging.
Footnotes
Author Disclosure Statement
No competing financial interests exits.