
Abstract
Abstract
Objective:
The aims of this research were to characterize unscheduled postoperative contacts made by gynecologic surgical patients and to identify factors that predispose patients to contact their providers postoperatively.
Materials and Methods:
This was a retrospective chart review. A convenience sample of all patients undergoing gynecologic surgery at the Cleveland Clinic in Cleveland, OH, over 3 months was utilized. Patients were identified by reviewing the electronic medical records (EMRs). Patient charts were reviewed for potentially relevant demographic and clinical information, as well as any patient-initiated telephone or clinic encounters occurring within 30 days of hospital discharge. Patients with at least one encounter (“Contact” group) were compared to those with no encounters (“No Contact” group).
Results:
Of the 547 patients undergoing surgery during this time frame, 331 (60%) contacted their providers at unscheduled times postoperatively, resulting in a total of 797 postoperative contact encounters. Patients most commonly contacted their providers regarding new (316 encounters; 50%) or existing (104 encounters; 17%) symptoms. Pain (29% [n = 123]) and wound issues (19% [n = 81]) were the most commonly reported symptoms. The outcome of these encounters was most often reassurance (37% [n = 232]), particularly for complaints about vaginal bleeding, pain, and wound concerns. Patients in the Contact group were significantly more likely to have diagnoses of chronic pelvic pain (14.2% [n = 47] versus 7.4% [n = 16], p = 0.015) or anxiety and/or depression (34.7% [n = 115] versus 26.4% [n = 57], p = 0.04).
Conclusions:
The majority of patients undergoing gynecologic surgery seek medical advice via telephone postoperatively, primarily due to new or existing symptoms. A substantial number of these encounters do not require any further management, highlighting areas where patient education can be improved before hospital discharge.
Introduction
T
Despite the growing prevalence of telephone consultations postoperatively, the literature on this topic remains relatively limited, with the majority of existing studies based in pediatrics5,6 or family medicine.7,8 A PubMed review of the literature from 1980 to 2017, using the search terms telephone, phone calls, postoperative, women's health, and gynecology found no studies that examined postoperative calls made specifically by gynecologic patients. Thus, the objective of this study was to characterize the reasons for seeking unscheduled medical advice (telephone calls, secure e-messages, unscheduled office visits, or emergency department visits) postoperatively among gynecologic patients. Furthermore, the current authors sought to gain a better understanding of this cohort by determining any potential demographic or clinical factors that predispose patients to contact their providers postoperatively.
Materials and Methods
This retrospective chart review was approved by the institutional review board at the Cleveland Clinic. We utilized a convenience sample of all consecutive patients who underwent gynecologic surgery at the Cleveland Clinic in Cleveland, OH, from April 1 to June 30, 2016. This included surgeries performed by surgeons in the Benign Gynecology, Urogynecology, Gynecologic Oncology, and Reproductive Endocrinology & Infertility divisions. Eligible patients were identified through the electronic medical records (EMRs). Any obstetric or nonpostoperative patients were excluded, as were patients who underwent surgery at one of the satellite hospitals. Study data were collected and managed using REDCap [Research Electronic Data Capture] electronic data capture tools hosted at the Cleveland Clinic. 9 REDCap is a secure, web-based application designed to support data capture for research studies, and among other features, provides functionality to validate database accuracy.
Once identified, patient charts were reviewed for relevant demographic and clinical information, as well as any postoperative encounters occurring within 30 days of hospital discharge. This included telephone calls, MyChart messages (an online portal in which patients and physicians can communicate through secure e-messages), emergency room visits, and unscheduled office visits. All types of postoperative encounters were incorporated, rather than just telephone calls, in order to capture all patients who sought medical advice in the postoperative period outside of their routine scheduled postoperative visits. Postoperative visits or telephone calls that were scheduled or initiated by the gynecology surgical team were not considered in this analysis, as the goal was to examine solely unscheduled postoperative encounters. For patients with more than 3 postoperative encounters, detailed information was only collected about the first 3 encounters. Patients were dichotomized into 2 groups: (1) those who contacted their providers postoperatively outside of scheduled postoperative encounters (Contact group) and (2) those who did not (No Contact group).
Specific information about each postoperative encounter was recorded, including the reason and outcome of the encounter. Often, more than one reason or outcome was listed for a given encounter. For telephone calls, the time of the call was documented. Calls made between 5:00
It is routine at the Cleveland Clinic for all patients scheduled for surgery to undergo a preoperative teaching visit with a nurse in the days preceding surgery. During this visit, patients are educated regarding pre- and postoperative instructions. Postoperative teaching covers topics such as activity restrictions, incision care, pain medications, side-effects of pain medications, and symptoms of a urinary tract infection (UTI). Teaching also includes an overview of expected recovery (vaginal bleeding, pain, fatigue, flatulence-related pain, etc.) and when to notify a physician (fever, chills, nausea, vomiting, increased pain, heavy vaginal bleeding, etc.). Postoperative instructions are again provided to the patient in writing and reviewed by the nurse upon the patient's discharge from the hospital.
The Charlson comorbidity index (CCI) 10 —one of the most widely used indices for measuring comorbidity—was utilized as an indicator of disease burden. The CCI consists of 19 comorbidities that are weighted and summed to give a score from 0 to 33. The CCI was originally developed to predict 1-year mortality in a mixed population of internal medicine patients but has since been validated in a variety of populations. The Opioid Risk Tool (ORT) 11 —a validated screening tool designed to assess risk for opioid abuse—was also utilized. A score of 3 or less indicates low risk for future opioid abuse, 4–7 indicates moderate risk, and ≥8 indicates high risk.
Categorical factors were summarized using frequencies and percentages, while continuous measures summaries used means and standard deviations and median and range. To evaluate risk factors, Pearson's χ2 tests, Fisher's exact tests, a two-sample t-test, and a Kruskal–Wallis test were used. Analyses were performed using SAS software (version 9.4; Cary, NC). A significance level of p = 0.05 was assumed for all tests.
Results
Of the 547 patients who underwent surgery during the study period, 331 patients (60%) made some kind of postoperative contact outside of their regularly scheduled postoperative encounters, and were classified as being in the Contact group. Table 1 shows patient demographics and medical histories for the Contact and No Contact groups. The Contact group was more likely to have anxiety and/or depression and chronic pelvic pain. The Contact group had a statistically significant higher total ORT score, indicating greater risk of opioid abuse, compared to the No Contact group. There was no significant difference in preoperative narcotic prescription use or discharge narcotic prescriptions, however. The Contact group was more likely to use psychiatric medications preoperatively. Patients in this group were also more likely to have been discharged with a nonroutine prescription (prescriptions other than nonsteroidal anti-inflammatory drugs, narcotics, laxatives, or anticoagulants) and have a significantly higher number of unscheduled preoperative encounters. In addition, the Contact group was more likely to have had surgeries in the Urogynecology division and less likely to have had surgeries in the Benign Gynecology division (Table 1).
Demographics and Medical Histories: Contact Group Versus No Contact Group
Values are presented as mean ± SD, median (min, max), or n (%).
p-Values: *analysis of variance; †Pearson's χ2 test; ‡Kruskal–Wallis test.
SD, standard deviation; CCI, Charlson Comorbidity Index; min, minimum; max, maximum; ORT, Opioid Risk Tool.
Notable patient demographics and characteristics with no significant differences between the Contact and No Contact groups included age, ethnicity, body mass index, employment status, smoking status/pack-years, insurance status, menopause status, number of pregnancies, prior abdominal or pelvic surgery, and American Society of Anesthesiologists (ASA) score. There were no significant differences between CCI scores. There were also no differences between the individual comorbidities that make up the CCI (data not shown).
Table 2 compares surgical factors between the Contact group and No Contact group. The Contact group was more likely to have received general anesthesia. These patients had longer surgeries and longer hospitalizations, compared to patients in the No Contact group. The No Contact group was more likely to have had outpatient surgery. For outpatient procedures, the Contact group had a longer length of recovery in the post-anesthesia care unit before discharge. The Contact group was also more likely to have documented intraoperative or postoperative complications. The Contact group patients had a higher rate of being discharged with drains, lines, or indwelling transurethral catheters. The Contact group patients were more likely to be discharged with home health care or to be discharged to skilled nursing facilities or rehabilitation facilities.
Surgical Factors: Contact Group Versus No Contact Group
Values are presented as mean ± standard deviation, median (minimum, maximum) or N (%).
Drains/lines included Foley catheter, JP drain, peripherally inserted central catheter line, ostomy, percutaneous nephrostomy tube, Medi-port,® and central line.
Nonroutine discharge prescriptions included antibiotics/antifungals, antiemetics, hormonal medications, psychiatric medications, antidiarrheals, and muscle relaxants.
p-Values: *analysis of variance; †Fisher's exact test; ‡Pearson's χ2test; §Kruskal–Wallis test.
MAC, monitored anesthesia care; PACU, post anesthesia care unit.
Surgical characteristics with no significant differences between the two groups included elective surgery status and estimated blood loss. The Contact group patients had significantly higher rates of readmission within 30 days, surgical-site infections, and ileus or small-bowel obstructions. The Contact group also had higher rates of reoperation, accidental punctures or lacerations, intraoperative blood losses >1 L, blood transfusions greater than 4 units, unplanned intensive care unit admissions, anastomotic leaks, and acute kidney injuries; however, these were all rare events and none of these comparisons achieved statistical significance (data not shown).
The number of unscheduled postoperative encounters per patient is shown in Figure 1. A total of 216 patients made no unscheduled postoperative contact (39%), while 137 patients (25%) had 1 unscheduled postoperative encounter and 158 patients (29%) had between 2 and 4 unscheduled encounters. There were 36 patients (7%) with 5 or more unscheduled encounters. A total of 797 unscheduled postoperative contact encounters were documented, and 628 of these were analyzed in detail (the remaining 169 encounters were excluded from those patients with more than 3 encounters). Of these unscheduled provider contacts, 81%were telephone calls, 14% were secure e-messaging, 3% were office visits, and 3% were emergency room visits.
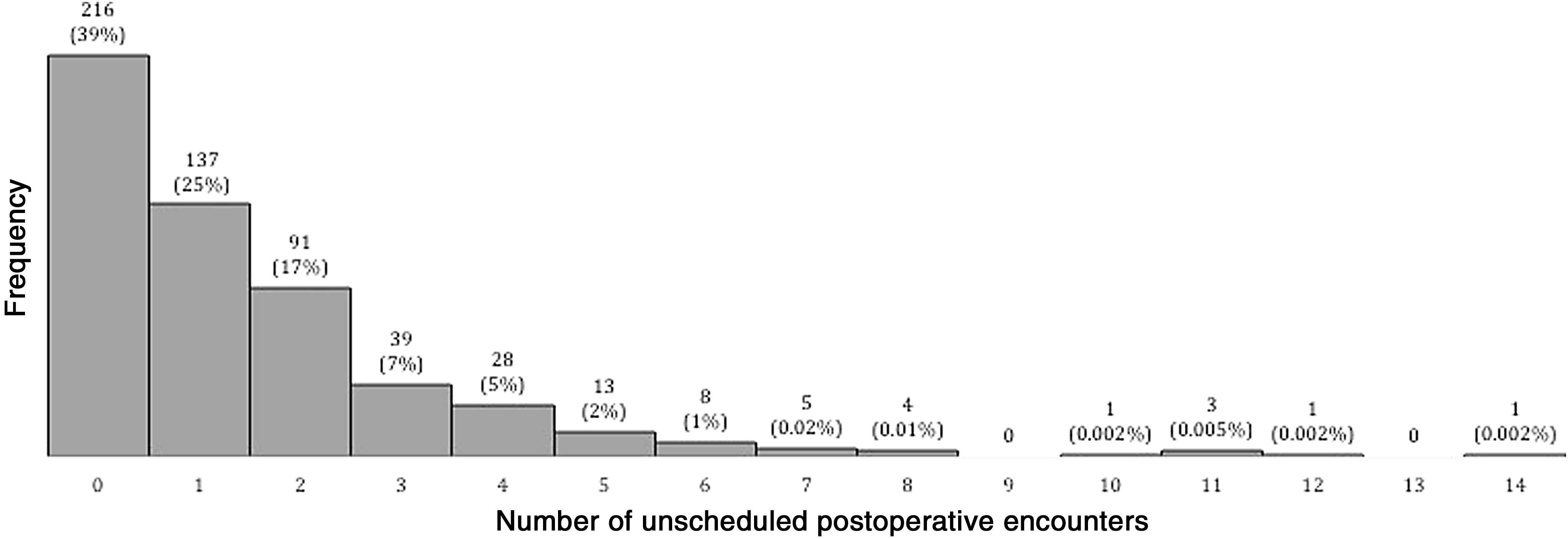
Distribution of number of unscheduled postoperative encounters.
Reasons for encounters included new symptoms (50% [n = 316]), existing symptoms (17% [n = 104]), questions about medications (7% [n = 46]), requests for medication refills (4% [n = 27]), and requests for appointments (4% [n = 27]). The specific symptoms reported were pain (29% [n = 123]), wound concern (19% [n = 81]), urinary complaint (16% [n = 68]), vaginal bleeding (12% [n = 50]), constipation (8% [n = 32]), nausea/vomiting (6% [n = 27]), swelling (4% [n = 18]), and fever (4% [n = 17]). Other reported symptoms included numbness/tingling, fatigue, shortness of breath, problem with drain/line, loss of appetite, or other vaginal complaint (all <1%).
The outcome of these encounters was most often reassurance (37% [n = 232]), followed by new prescription (11% [n = 68]), expedited office evaluation (10% [n = 60]), medication adjustment (9% [n = 58]), recommendation to present to the emergency department (6% [n = 38]), new laboratory testing or imaging (4% [n = 27]), referral to other specialist (4% [n = 23]), and admission (2% [n = 11]). When examining outcomes for specific symptoms, urinary complaints, most often voiding dysfunction, were most likely to result in emergency department recommendation (21% [n = 7]) or expedited office evaluation (21% [n = 7]). Constipation was most likely to result in medication adjustment (73% [n = 11]). Reassurance was the most common action for complaints of vaginal bleeding (75% [n = 22]), pain (40% [n = 15]), and wound concerns (63% [n = 22]). Patients who had inpatient surgery were more likely to contact their providers with complaints of fever, compared to patients with outpatient surgery (4% [n = 16] vs. 0.5% [n = 1]; p = 0.010). Patients who had inpatient surgery were also more likely to be admitted as a result of an unscheduled encounter (3% [n = 11] versus 0% [n = 0]; p = 0.010).
The majority of unscheduled postoperative encounters (80%) took place during normal office hours, with the remainder of encounters taking place after hours. Patients who called after hours were most likely to call with a new symptom (70% [n = 72]) compared to patients who called during office hours (51% [n = 202]; p < 0.001). Patients calling after hours with new symptoms were more likely to report fever (8% [n = 7] versus 3% [n = 8]; p = 0.019). Patients who called after hours were also more likely to have been discharged with indwelling transurethral catheters (20% [n = 17] versus 9% [n = 22]; p = 0.009). There were no significant differences between other symptoms. Compared to office-hours encounters, after-hours encounters were more likely to result in reassurance (50% [n = 51] versus 35% [n = 138]; p = 0.005) or recommendation to present to the emergency department (22% [n = 23] versus 4% [n = 15]; p < 0.001). In contrast, unscheduled encounters during office hours were more likely to result in expedited office evaluation (12% [n = 49] versus 3% [n = 3]; p = 0.005).
Discussion
The results of the current study indicated that 3 of 5 gynecologic surgical patients sought unscheduled medical advice postoperatively. In addition, the majority of the patients in the current study who contacted their providers postoperatively did so on more than 1 occasion. The study also identified several key factors associated with contacting a healthcare provider postoperatively, including preoperative diagnoses of anxiety, depression, and chronic pelvic pain. These factors are significant because they can be used to target educational interventions toward patients at greatest risk. These findings are consistent with prior literature, which has shown higher healthcare utilization among patients with psychiatric comorbidities 12 and women with chronic pelvic pain. 13 While the Contact group scored significantly higher on the ORT, narcotic prescription usage did not differ significantly between the groups. This is in contrast to research from an inflammatory bowel disease clinic in which increased telephone encounters were associated with higher levels of narcotic prescriptions. 14
The current study showed that patients who made unscheduled medical contact postoperatively had significantly longer surgeries, longer hospitalizations, and greater perioperative complications, which likely reflected differences in surgical complexity between the 2 study groups. However, the current authors were unable to test this hypothesis directly, because the myriad procedures performed across the very different subspecialties included made it not feasible to rank procedures by level of complexity. It is plausible, however, that women in the Contact group underwent more complex procedures, experienced more issues after discharge, and thus had more encounters postoperatively.
The finding that patients in the Contact group were more likely to be discharged with drains or lines, particularly indwelling transurethral catheters, supports this concept and has been reported previously in the literature. 15 While catheters can play a role in the development of postoperative UTIs, catheters are also are a potential cause of patient discomfort and anxiety. Interestingly, patients from the Urogynecology service—who conventionally are most commonly discharged to go home with catheters—were also significantly more likely to contact their providers postoperatively. It is likely that many postoperative encounters could be prevented if patients are adequately educated by the nursing staff and provided with sufficient drain instructions upon hospital discharge. Furthermore, improved office counseling preoperatively might help to mitigate the volume of postoperative calls received. Patients who are discharged without adequate information are more likely to access a healthcare facility following discharge, if even just for reassurance.16,17
The primary limitation of this study was its retrospective design, as the information collected relied on the accuracy of what was recorded in the EMR. While it is possible that clinical information and details about each encounter were documented in the EMR incompletely, the Cleveland Clinic has utilized a comprehensive EMR system for almost 15 years, which enables accuracy and consistency of information over time and across specialties. The study was also limited in that it only included patients from a single institution. As a tertiary referral center, the Cleveland Clinic cares for a disproportionately high percentage of patients with complex presentations and advanced disease, compared to many general gynecology practices. Nevertheless, the Cleveland Clinic cares for a high volume of patients with a broad range of presentations that represent all major clinical aspects of gynecology.
The majority of unscheduled postoperative encounters were in regard to a new symptom, with pain and wound issues being the two most commonly reported symptoms. Management of pain relief and wound care have repeatedly been found to be top concerns of postoperative patients after discharge.4,16,18–22 While many of the postoperative encounters were for legitimate postoperative problems, more than one third of the patients calling did not require further medical management. The finding that a significant portion of patients calling with vaginal bleeding, pain, and wound concerns did not require any further intervention, identifies key areas where preoperative patient education should be improved.
One-half of after-hours callers did not require further intervention beyond reassurance, which was consistent with prior research from several different specialties.1,23–26 In 1 study of after-hours calls made to a general obstetrics and gynecology clinic, physicians rated 36% of these calls to be inappropriate. Among nonpregnant callers, only 9% required immediate evaluation. When asked what action they would have taken had they been unable to contact an on-call physician, only 19% of respondents said that they would have presented to the hospital for evaluation and 53% of respondents said that they would have called the office in the morning. 27
Conclusions
The significant discrepancy in perception of urgency among callers emphasizes further need for physicians to educate patients and provide guidance on the appropriate usage of services and to include education interventions preoperatively that can reduce patients' anxiety or concern about common postoperative symptoms. Given the finite amount of time and resources available, preventing inappropriate healthcare utilization enables physicians to care better for their patients with the most need. On a more global level, appropriate utilization allows healthcare systems to reduce unnecessary expenditures. Substantial savings could result if even a fraction of inappropriate utilization was prevented.
Footnotes
Acknowledgment
The authors thank Lin Mei, MS, for her assistance with data collection.
Author Disclosure Statement
The authors report no conflicts of interest.