
Abstract
Abstract
Background:
Malignant mesothelioma (MM) is an aggressive neoplasm whose pathogenesis is conventionally associated with occupational and environmental respiratory exposure to asbestos. MM affects derivatives of the embryologic coelomic epithelium, the: pleura; peritoneum; pericardium; and tunica vaginalis testis. Primary peritoneal mesothelioma generally presents with vague abdominal symptoms and usually presents late in the disease's course. Frequently, patients are diagnosed in advanced stages, and the prognosis is very poor.
Case:
A 40-year-old premenopausal woman, gravida 3, para 1, presented for an abdominal myomectomy to address her history of a symptomatic fibroid uterus. Exploration of the pelvis revealed diffuse suspected metastatic cancer of an unknown origin; therefore, pelvic washings and biopsies of the lesions were performed.
Results:
Pathology testing showed that this patient had biphasic peritoneal mesothelioma. Ultimately, the patient refused all conventional treatments and decided to seek alternative medicine options.
Conclusions:
Biphasic peritoneal mesothelioma is a rare malignancy with a poor prognosis and requires aggressive management with the current “gold standard” of cytoreductive surgery followed by hyperthermic intraperitoneal chemotherapy. Despite extensive research survival has not improved in recent decades. (J GYNECOL SURG 34:214)
Introduction
M
Case
A 40-year-old woman, gravida 3, para 1, premenopausal woman, who worked as a university lecturer, presented for an abdominal myomectomy secondary to now having a symptomatic fibroid uterus. The patient had a 3-year history of progressive chronic pelvic pain, menorrhagia, and abdominal distention. An initial examination revealed a multiple fibroid uterus of 26 weeks' gestational size. Secondary to the uterine size, she was not a candidate for minimally invasive surgery and underwent a laparotomy via a Pfannenstiel skin incision. This procedure was performed in a standard fashion. An anteverted uterus of 26 weeks' gestational size, grossly deformed secondary to multiple fibroids, was exteriorized from the abdomen.
Upon routine inspection of this patient's peritoneal organs, a 4-cm mass was noted on the sigmoid colon. This mass did not appear to obstruct the colonic lumen; yet, the mass was on the serosa. This prompted further investigation, and smaller implants of masses were noted on the posterior uterus, bilateral ovaries, and anterior bladder peritoneum. The anterior abdominal wall peritoneum appeared to be speckled with similar lesions. Intraoperative consults to general surgery and gynecologic oncology were made and both specialties recommended biopsies of the lesions and pelvic washings. The initial frozen pathology sections for the biopsies all showed papillary lesions with origins to be determined. In order to return the uterus to the abdominal cavity, it was necessary to remove the bulky mass of fibroids. An endometrial cavity-entering abdominal myomectomy was performed with a total removal of 43 fibroids. Then, the uterus was returned to the abdominal cavity. The patient tolerated the procedure well; however, her postoperative course was complicated by ileus, which resolved via supportive measures. The main differential diagnosis at the time of surgery was of metastatic ovarian versus colonic malignancy.
Results
The patient was discharged to go home on postoperative day 3 prior to the pathology results. Her tumor markers were: cancer antigen (CA)–125 and carcinoembryonic antigen were 161 and 0.7, respectively.
Microscopically, the lesions from the posterior uterus, bladder, and sigmoid colon showed a proliferation of atypical mesothelial cells arranged in a tubulopapillary growth pattern infiltrating into the underlying parenchyma with associated desmoplastic stromal reactions. The neoplastic cells were predominantly epithelioid in morphology, but focal areas with spindled cells merging with the epithelioid component were also seen. See Figures 1 and 2.
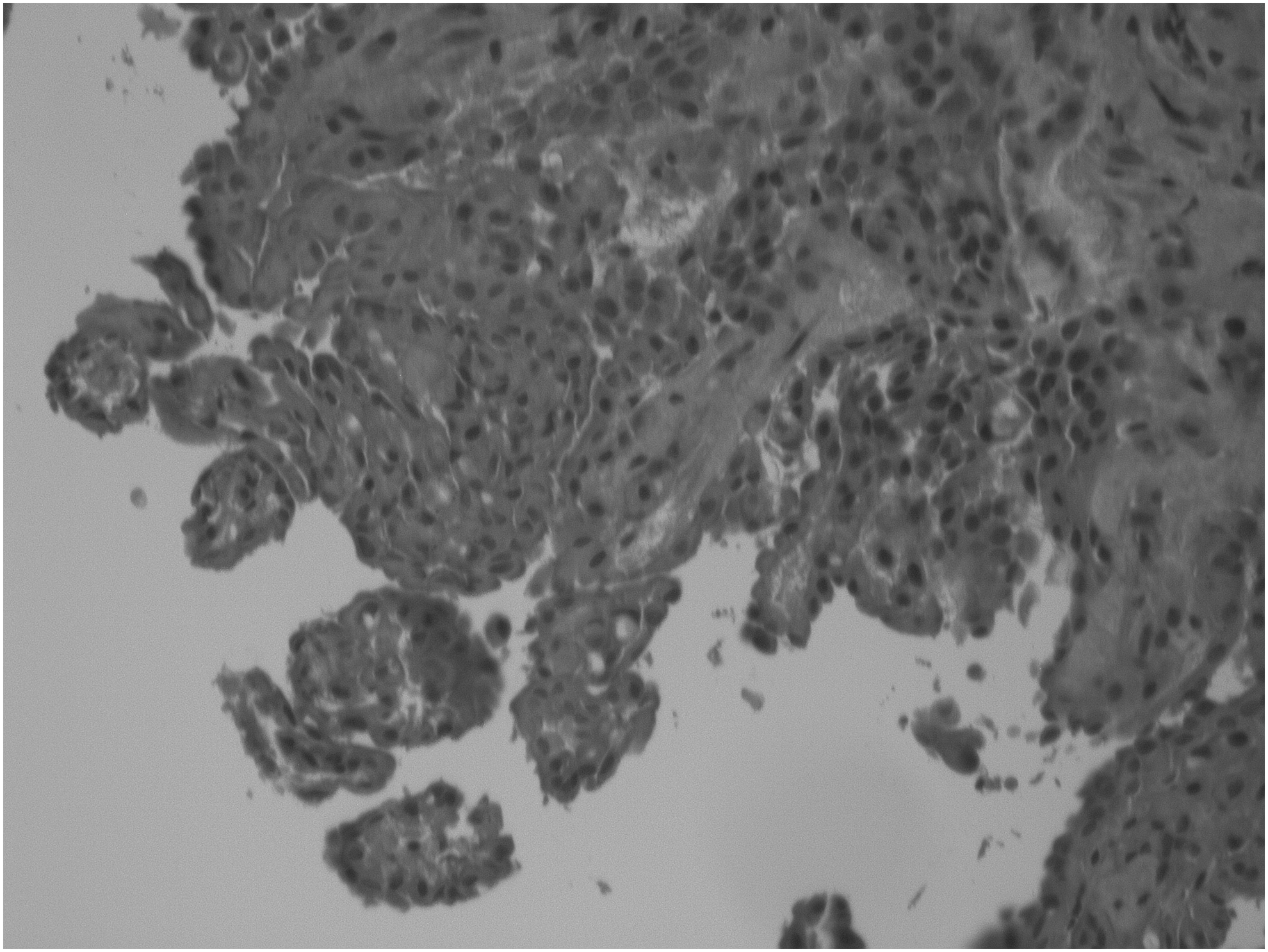
Hemotoxylin and eosin stain of posterior uterine biopsy at 20 × magnification.

Calretinin stain of right ovarian biopsy at 2 × magnification.
Immunohistochemically, the neoplastic cells were immunoreactive for calretinin and Wilms tumor (WT)–1 and lacked reactivity for Ber-EP4 and MOC-31. MIB1 (Ki67) were highlighted in 30%–40% of the neoplastic cells (a high proliferative index). The morphologic and immunophenotypic features were most consistent with MM, favoring a biphasic (mixed) type. Other lesions found in the ovaries also showed histologic features consistent with MM. The uterus weighed 1052 g in total and consisted of multiple leiomyomata ranging from 0.8 cm to 9.5 cm. The endometrium was histologically unremarkable with benign proliferative endometrium.
This diagnosis was confirmed via consultation from Memorial Sloan Kettering. The patient had a follow-up with her obstetrics/gynecology practitioner and a medical oncologist. Reportedly asymptomatic, she denied weight loss, changes in bowel function, abdominal pain, distention, anorexia, or night sweats. Furthermore, she expressed an understanding of her diagnosis and treatment recommendations. However, she refused all conventional treatment options offered and decided upon alternative medical treatments.
Discussion
As noted in the Introduction, MM is an aggressive neoplasm whose pathogenesis is conventionally associated with occupational and environmental respiratory exposure to asbestos and affects derivatives of the embryologic coelomic epithelium: the pleura; peritoneum; pericardium; and tunica vaginalis testis.1–3 The affected organs are primarily pleural (80%–90%) and peritoneal (10%–20%), pericardial (< 1%), and tunica vaginalis testis.3–5
The peritoneal cavity is the second most common site of primary mesothelioma, with an estimated incidence of 300–500 new cases per year in the United States, affecting men more than women, and presenting in the fifth decade of life. 6 Secondary to the latency period, from exposure to disease presentation and ranging between 20 and 40 years, identifying exposure can be complicated in patients without evidence of occupational exposure.2,7,8
Primary peritoneal MM conventionally presents with vague complaints of abdominal pain, increased girth, early satiety, ascites, night sweats, weight loss, and/or bowel obstruction.2,8,9–13 Secondary to the prolonged latency between exposure to asbestos and mesothelioma, linking nonpulmonary mesothelioma to asbestos exposure directly can be difficult—if not impossible. Authors of case reports have posited multiple routes of environmental exposure, including via ingestion of contaminated food and water with the asbestos fibers being transported across the intestinal tract mucosa.2,9,14
Due to the vague symptoms, patients generally present late, are diagnosed with advanced stages, and have very poor prognoses. 2,5,8,15 The overall 5-year survival for localized peritoneal mesothelioma was estimated at 26%. 16 Improved life expectancy has been demonstrated when patients undergo cytoreductive surgery (CRS) followed by adjuvant hyperthermic intraperitoneal chemotherapy (HIPEC).5,8,17–19 This treatment approach is widely considered to be the current standard of care. There is currently no evidence that single-treatment modalities (surgery, chemotherapy, or radiation) alone increase life expectancy.5,17–19 Of patients who undergo CRS followed by HIPEC, favorable prognostic factors are female gender, epithelioid histology, absence of lymph-node metastases, and complete cytoreduction.11,18,20
There is no universal staging system for primary peritoneal MM, although staging systems have been proposed.18,21 Computed tomography imaging generally reveals nonspecific diffuse sheetlike thickening and nodular irregularity of the peritoneum with ascites.22–23 Ascitic fluid obtained via paracentesis is often inconclusive; therefore, a tissue sample for histologic and immunochemical evaluation is required for diagnosis. Due to the MM's peritoneal origin, the tumor markers CA-125 and mesothelin-related protein are often elevated. As in the case we present, the gold standard for diagnosis is tissue biopsy, immunohistochemical staining for calretinin, WT-1 antigen, mesothelin, and cytokeratin 5/6. 6 Histologic types include epithelioid (60% of cases), sarcomatoid (25% of cases), and mixed or biphasic (15% of cases).2,16 The mixed or biphasic histologic type contains both epithelial and fibrous sarcomatoid components and has a less favorable treatment response. 16
Conclusions
Biphasic peritoneal mesothelioma is a rare malignancy with a poor prognosis and requires aggressive management with the current gold standard of CRS followed by HIPEC. Despite extensive research, survival has not improved in recent decades. 16
Footnotes
Acknowledgment
The authors would like to thank Tatiana Holway, PhD, for editing this case report.
Author Disclosure Statement
The authors of this article have no financial or commercial interests associated with this publication.