
Abstract
Abstract
Background:
Massive ovarian edema (MOE) is a rare benign condition causing enlargement of the ovaries by edema fluid. The risk for women suffering from MOE is that the ovaries are removed as they can be mistaken for tumors, which can then potentially result in premature menopause. However, wedge resection and/or ovaropexy is now the treatment of choice.
Case:
A 28-year-old nulliparous patient experienced 8 years of episodic abdominal pain due to intermittent ovarian torsion resulting in bilateral MOE.
Results:
The patient was treated successfully with conservative surgery involving ovarian detorsion and bilateral ovaropexy. Her symptoms resolved and follow-up ultrasound showed a dramatic reduction in bilateral ovarian sizes.
Conclusions:
MOE, due to chronic torsion, can be treated with a conservative laparoscopic approach, obviating the need for oophorectomy or wedge resection.
Introduction
F
Institutional review board/ethics committee approval and patient consent were obtained to prepare this case report.
Case
A 28-year-old nulligravida woman was referred with chronic intermittent lower abdominal pain and large adnexal masses. She had episodic intense pain lasting 4–5 days ∼2–3 times per year over 8 years and had been seen by physicians; however, no formal diagnosis was ever made apart from her having a slightly enlarged left ovary. Transvaginal ultrasound (TVUS) was performed at an outside institution; the TVUS showed a 10 cm left ovarian “cystic lesion” with a benign appearance. She was followed with serial TVUS until the left ovarian “cystic lesion” grew to 17 cm and a 5 cm right ovarian lesion was also seen. At this point, she was referred to gynecology for surgical exploration.
The patient was otherwise healthy and was not taking any medications apart from an oral contraceptive pill. Her menstrual cycles had always been irregular and her menstrual flow was light. Her body mass index was 24.5, and she did not have any signs of virilization.
On examination, it was noted that she had a palpable mass on the right side. Her follicle-stimulating hormone, luteinizing hormone, thyroid stimulating hormone, and dehydroepiandrosterone sulfate levels were normal. TVUS at the time of presentation showed a normal-size uterus and bilateral ovarian masses. The right ovary was located in the right hemipelvis; this ovary was diffusely hypoechogenic and markedly enlarged, measuring 7.4 × 5.8 × 5.3 cm (volume 227 cc) with multiple small peripheral follicles. The left ovary was situated in the right paraumbilical region, cranial to the uterus. This ovary was hypoechogenic and markedly enlarged, measuring 10.0 × 7.9 × 9.0 cm (volume 371 cc), and contained multiple peripheral follicles (Fig. 1A and B). Both ovaries had a solid tumorlike mass appearance. Blood flow was noted in both ovaries but was relatively reduced in the left ovary. Engorged gonadal vessels were noted bilaterally. There was a small amount of free fluid in the right side of the pelvis.

Transvaginal ultrasound shows markedly enlarged solid-appearing adnexal lesions that represent grossly enlarged ovaries with peripherally displaced follicles
The case was presented and discussed at the current authors' multidisciplinary case conference (MCC). A contrast-enhanced pelvic MRI scan performed prior to the referral was reevaluated confirming the current authors' US findings of bilateral massive ovarian enlargement with diffuse stromal T1 hypointensity, T2 hyperintensity, and multiple peripheral follicles (Fig. 2). The left ovary on the MRI study was even larger at that point, measuring 16.9 × 10.1 × 6.0 cm (volume 535 cc). There was delayed and decreased contrast enhancement of the ovarian parenchyma bilaterally with twisted and engorged vascular pedicles.
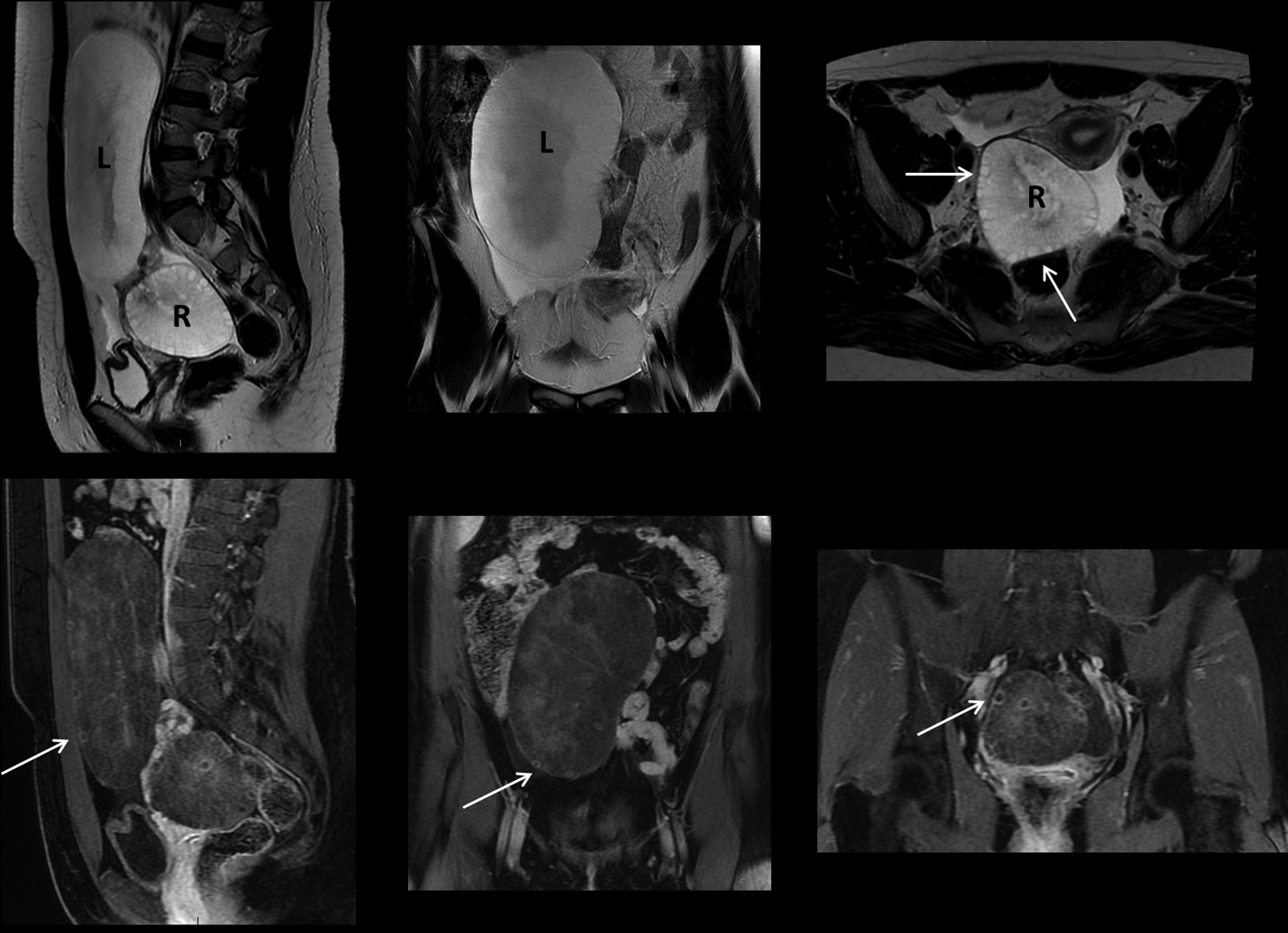
Pelvic magnetic resonance imaging. T2-weighted images (top row) and T1-weighted fat saturated post gadolinium images (bottom row) show grossly enlarged T2 hyperintense ovaries suggesting severe edema. Both ovaries appear diffusely hypo-enhancing with peripherally displaced follicles (arrows). R, right; L, left.
The MCC review identified the potential diagnosis of MOE, and the patient was scheduled for laparoscopic surgery. During the surgery, bilateral ovarian torsion was noted. The left utero-ovarian ligament was torted 3 times and the right utero-ovarian ligament was torted 2 times. After detorsion, significant elongation of the utero-ovarian ligaments was noted (∼ 6 cm on the right side and ∼10 cm on the left side). A tubal dye test showed a patent right tube and a blocked left tube. The left tube was ∼20 cm long and appeared to be significantly damaged and scarred. Due to the features on imaging, the patient's age, and no suspicious features of malignancy, it was decided to conserve both ovaries. Bilateral ovaropexy and left salpingectomy were performed.
Due to the size and weight of the ovaries, classic ovaropexy with fixation of the ovaries to the abdominal wall or pelvic sidewall was not possible. On the right side, the utero-ovarian ligament was sutured to the round ligament, using 4 PDS® sutures. This fixed the ovary, thereby preventing any future episodes of artificial torsion. On the left side, a salpingectomy was initially performed to remove the damaged fallopian tube and prevent a possible tubal pregnancy. Due to the extreme length of the utero-ovarian ligament on this side the ovaropexy technique used on the right side was insufficient because it still allowed torsion of the ovary. It was therefore decided to fold the utero-ovarian ligament in the middle—which, due to its length, was possible without kinking the vessels—and then suture it to the left-sided round ligament (at its insertion into the uterus) and to the peritoneum of the left pelvic sidewall, using 5 PDS sutures.
Pelvic washings and ovarian biopsies were taken and were negative for malignant cells. The ovarian biopsies contained ovarian stroma without epithelial elements.
Results
The patient's postoperative course was uneventful. She was seen 8 weeks postoperatively, and was free of symptoms and having regular menstrual cycles. On TVUS, both ovaries were significantly noted to be smaller. The right ovary fluid volume was 24 cc (from 227 cc) and the left ovary fluid volume was 67 cc (from 371 cc). On MRI, it was noted that both ovaries were well-positioned and had normal T1 and T2 weighted signals (Fig. 3). Repeat TVUS 18 months after surgery showed further reduction in the fluid volume of the left ovary to 50 cc. The right ovary showed further mild reduction in fluid volume to 22 cc (Figure 1C and D). Both ovaries had numerous peripheral follicles, and normal arterial and venous Doppler flows.

Pelvic magnetic resonance imaging. T2-weighted axial image 8 weeks following surgery shows marked reduction in the volumes of both ovaries, which are now in normal position and have improved morphologies.
Discussion
MOE is a relatively rare condition consisting of unilateral or bilateral enlargement of the ovaries, with fewer than 200 cases described in the literature. 3 MOE has been reported to occur in females ranging in age from 6 months to 60 but most commonly affects women of childbearing age. 5
Bilateral MOE is rare, as 85% of cases are unilateral, usually involving the right ovary (75%). 6 Crowding of the left lower pelvis by the sigmoid colon and a different drainage pattern of the right ovarian vein resulting in increased pressure have been thought to play roles.6,7
MOE may be primary or secondary. Primary MOE occurs when there is no underlying ovarian pathology, and secondary MOE occurs in ovaries with a preexisting condition, including an ovarian mass, fibromatosis, polycystic ovaries, or following ovulation-induction drugs. 3
The etiology and pathogenesis of MOE remains controversial. It is still unclear whether MOE is a result of partial intermittent ovarian torsion, or if it is related to ovarian fibromatosis or stromal hyperthecosis with subsequent torsion due to increasing ovarian weight. 6
The most common presenting symptom is abdominal pain accompanied by a palpable adnexal mass. 7 Virilization is seen in 25% of cases. 6 It has been hypothesized that the lymphedema triggers proliferation of stromal cells and stromal-cell luteinization, which results in increased ovarian androgen and estrogen production, leading to virilization and potentially precocious or early puberty. 5
Although MOE has many overlapping features with ovarian tumors making a definitive preoperative diagnosis difficult, there are a few clinical and imaging findings that can be used to differentiate MOE from an ovarian tumor. Differential diagnosis for MOE based on imaging is broad and includes ovarian fibroma, metastatic carcinoma, lymphoma, polycystic ovary, or ovarian hyperstimulation syndrome. 4 MOE often presents with acute or intermittent abdominal pain, whereas ovarian tumors are often asymptomatic and, in the case of ovarian malignancy, symptoms even in late-stage disease are often nonspecific. Biochemical analysis of tumor markers, such as serum ß–human chorionic gonadotropin, lactic dehydrogenase, cancer antigen–125, and α-fetoprotein can be helpful, as these markers are usually normal in patients who have MOE. 3
A very important indicator of MOE is diffuse ovarian enlargement with displacement of the follicles to the periphery of the ovarian cortex, both visible on US and MRI scanning; this enlargement with displacement is a feature not typically seen in ovarian tumors. In MOE, the masslike edematous central ovarian stroma are not usually as hypoechoic as they are in some solid tumors, such as ovarian fibromas, which actually attenuate the US beam. On the contrary, in MOE, there is often enhanced transmission due to the high fluid content of the ovary, a sign typically absent in other solid ovarian tumors. Lack of Doppler US flow in the twisted ovary might be seen in MOE as opposed to in solid tumors, although, in cases of incomplete vascular obstruction, Doppler flow can still be present. Having said that, US findings can be nonspecific and similar to tumors, such as primary ovarian lymphomas and metastases, which can also be bilateral. However, MOE can usually be differentiated on MRI due to the distinctly hyperintense stroma on T2-weighted imaging in addition to the peripherally displaced follicles.4,8
Malignant epithelial neoplasms are distinguished easily from MOE because they typically contain both cystic and vascular solid components. Intratumoral hemorrhage and necrosis are suggestive of ovarian malignancy and are atypical features of MOE. Finally, presence of ancillary features—such as infiltration of pelvic organs or sidewall, lymphadenopathy, and peritoneal implants—can help distinguish malignant ovarian tumors from MOE. On histopathology, MOE is characterized by ovarian stromal cells separated by copious edema fluid.3,5
Various approaches to managing MOE have been reported in the literature. Most cases (82%) of MOE are overtreated with salpingo-oophorectomy, as they are often mistaken for ovarian tumors. 3 However, many researchers believe that fertility-preserving treatment for these nonneoplastic lesions is wedge resection, often removing 30% or more of the ovary to rule secondary causes out.3,5 Postoperative adhesions leading to fertility issues is a cited argument against this treatment modality. 3 Clear guidelines regarding long-term follow-up and monitoring recommendations have not been established yet.
Conclusions
The current case shows the value of MCCs to evaluate the findings and options, striving for thorough preoperative assessment, resulting in successful conservative surgical management with ovaropexy and obviating the need for oophorectomy or wedge resection, hence preserving hormonal function and fertility.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.