
Abstract
Abstract
Background:
Cervical diverticulum is a rare clinical malformation. The most-common clinical manifestation of such diverticula is menometrorrhagia, because a pouch develops for collecting menstrual blood.
Case:
A 37-year-old, gravida 1 para 1 woman was referred for menometrorrhagia and secondary infertility. Hysterosalpingography (HSG) showed irregularity in the uterine cavity without contrast agent spillage from the uterine tubes and indicated that she had Asherman's syndrome. She had a history of primary and secondary infertility, polycystic ovaries, three unsuccessful intrauterine inseminations (IU1s), and three unsuccessful intracycloplasmic sperm injections (ICSIs). All of these procedures had failed, and she finally conceived spontaneously. She was examined, via hysteroscopy and laparoscopy. A large diverticulum was noted between the internal and external os of her cervix that created obstacles to accessing the uterine cavity and led to the false report of Asherman's syndrome on the HSG.
Results:
Two days after the hysteroscopy and laparoscopy, transvaginal ultrasound evaluation of this patient showed the same findings as in the first ultrasound report. Therefore, the current authors assume that this space is a large diverticulum that is an obstacle to accessing the uterine cavity.
Conclusions:
In infertile patients who have HSGs indicating Asherman's syndrome and who complain of menometrorrhagia, cervical diverticulum could be the etiology. IUI and transfer of the embryo to the uterus guided by ultrasound is the recommended procedure for helping these patients achieve pregnancy.
Introduction
Cervical diverticulum is a rare clinical malformation.1,2,3 The most-common clinical manifestation of such diverticula is menometrorrhagia due to a pouch that has developed for collecting menstrual blood.1,4 This article is a case report of a patient who had menometrorrhagia and secondary infertility, and for whom hysterosonography (HSG) indicated Asherman's syndrome.
Case
The patient was a 37-year-old gravida 1, para 1 woman referred with menometrorrhagia for 2 years and secondary infertility for 4 years. HSG showed irregularity in the uterine cavity without contrast agent spillage from the uterine tubes; this was suspicious for Asherman's syndrome.
This patient had polycystic ovary syndrome (PCOS), primary infertility, three unsuccessful intrauterine inseminations (IUIs), and three unsuccessful intracycloplasmic sperm injections (ICSIs) prior to her first pregnancy. All of these procedures had failed, and she finally conceived spontaneously and had given birth by cesarean section 9 years ago. She developed oligomenorrhea that lasted until 2 years prior to the current referral. She also had experienced menometrorrhagia 2 years prior and went to a physician to address this. She underwent hysteroscopy and polypectomy, but her menometrorrhagia did not cease. The patient returned to her physician, who prescribed danazol for 6 months. The patient's menometrorrhagia as well as her menstruation ceased. Six months after stopping danazol administration, her menstruation returned to normal, although she complained of an occasional brown discharge.
Two months prior to the current referral, the patient's menometrorrhagia recurred, and her volume of bleeding increased and became irregular. Her transvaginal ultrasound report read:
A large echogenic lesion with a cystic component without vascularity measured as 35 x 22 mm in the cervix, which is mostly compatible with the retracted clot in this region due to the accumulation of blood in this region [Fig. 1]. Endometrial thickness was measured as 2 mm. The uterus was measured as 95 × 50 × 42 mm with a heterogeneous myometrial echo pattern. Both ovaries had an appearance resembling PCOS.
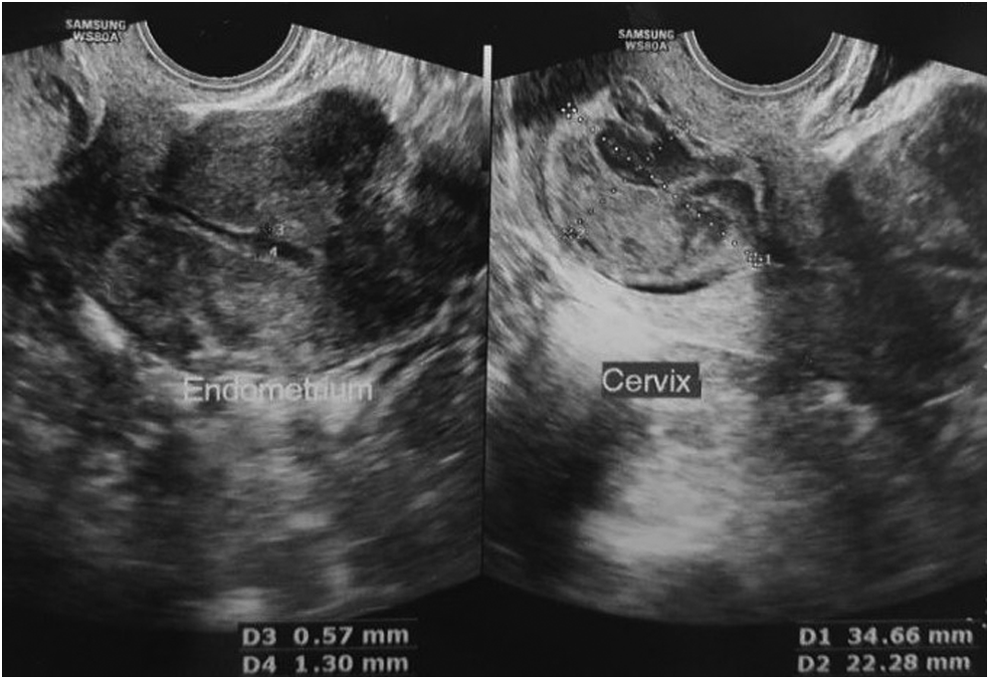
Transvaginal sonography showed a large echogenic lesion with a cystic component that did not have vascularity. The lesion was 35 × 22mm and was in the cervix.
Magnetic resonance imaging showed a 29 × 24 × 33–mm cystic lesion (T1 high/T2iso) without restriction and enhancement in the endometrial cavity. HSG showed irregularity in the uterine cavity without contrast agent spillage from the uterine tubes; this was suspicious for Asherman's syndrome (Fig. 2).
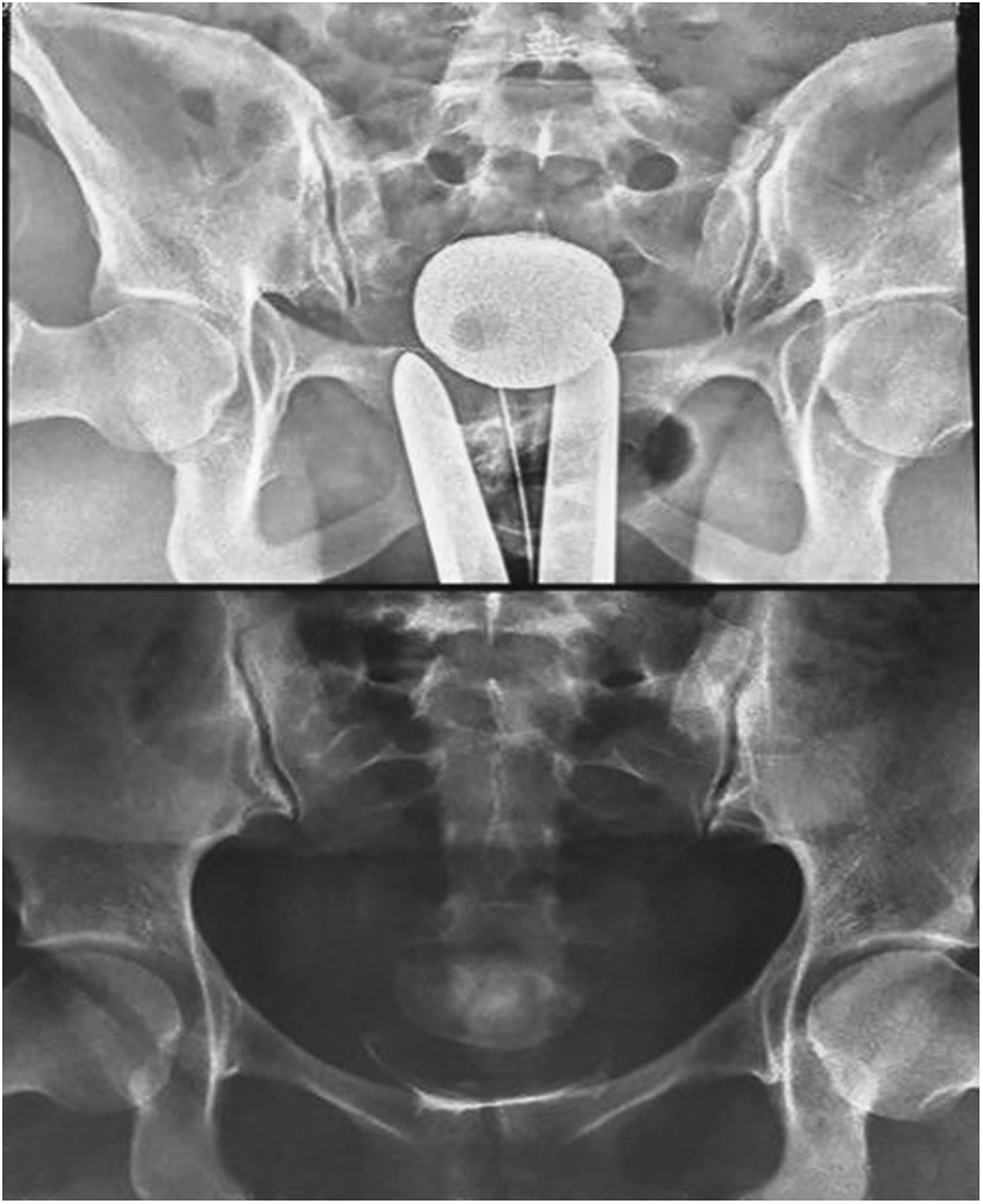
The hysterosalpingography finding was that there was irregularity in the endometrial cavity without spillage from the uterine tubes.
This patient underwent hysteroscopy and laparoscopy. During laparoscopy, her uterus was found to be myomatous, and there was some degree of adhesion of the omentum to the anterior abdominal wall. Both uterine tubes had normal spillage and were open, and the ovaries were polycystic.
At the beginning of this hysteroscopy and after dilatation of the cervix, ∼10 cc of a brownish fluid was extracted from the uterus. A large space was found between the internal and external os of the cervix during the hysteroscopy, and a clot of ∼20 × 30 mm was found in this space (Fig. 3). After leaving this space and passing through the cervical os, the uterine cavity was reached. The size of the uterine cavity was normal. See Supplementary Video to see how the uterine cavity was reached.
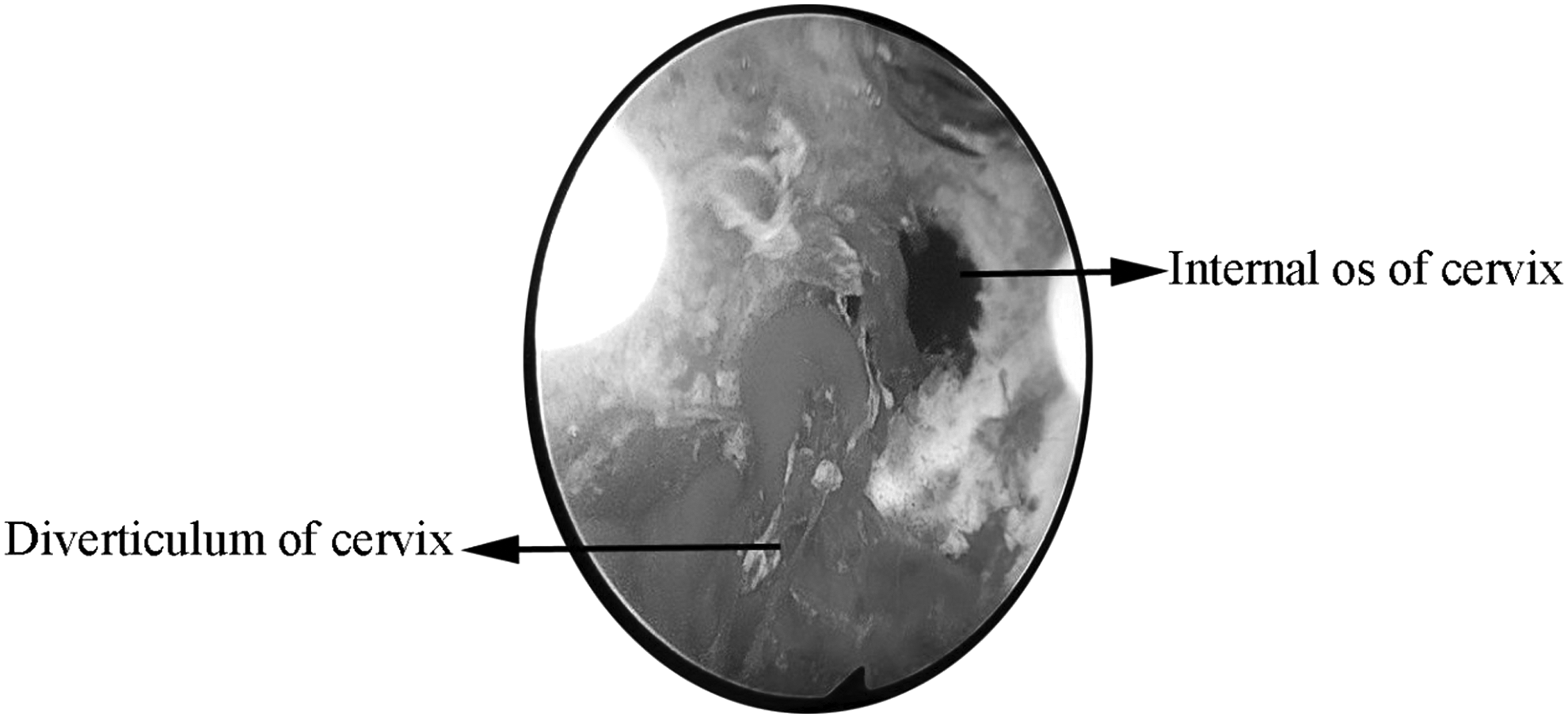
A huge space was found between the internal and external os of cervix, and a clot of ∼20 × 30 mm was found in this space (cervical diverticulum).
Results
Two days after the hysteroscopy and laparoscopy, transvaginal evaluation of the patient showed the same findings as the prior ultrasound report. The current authors, therefore, assume that this space was a large diverticulum that was an obstacle to accessing the uterine cavity.
Discussion
Cervical diverticulum is a rare clinical malformation. The most-common clinical manifestation of such diverticula is menometrorrhagia due to a pouch that develops for collecting menstrual blood. Few published articles about previous cases are available on this condition in Medline.®
Seoud et al. reported on a 31-year-old woman with menometrorrhagia and primary infertility who had an isolated cervical diverticulum that had caused prolonged postmenstrual spotting. 5 The patient became pregnant after controlled ovarian stimulation and ultrasound (US)-guided intrauterine insemination. 5 Turan et al. reported on a 30-year-old woman with a history of one cesarean section, secondary infertility, and an asymptomatic diverticulum with a diameter of 2–3 cm on the upper one-third of the cervix. 6 Stamtopoulos et al. reported on a 37-year-old woman with a known unicornuate uterus with a left rudimentary horn and recurrent hematometra. 1 On that patient's hysteroscopy, three cavities were identified, including two pertaining to the uterine horns and another to a cervical diverticulum. 1 Umezaki reported on a 41-year-old woman with fever and lower abdominal pain. 7 An extrauterine mass was detected in the woman, and hysterectomy was performed. Pathologic examination showed a cystic uterine diverticulum lined with cervical glands and myometrium arising from the cervix. 7
The current patient's greatest complaint was menometrorrhagia. She had a history of primary and secondary infertility and Asherman's syndrome was suspected per her HSG report. She had PCOS. Although PCOS is a cause of infertility, her three IUI failures, three ICSI failures, and then spontaneous pregnancy might have been due to a congenital diverticulum that obstructed the proper transfer of sperm and embryo to the uterine cavity.
Conclusions
In infertile patients with Asherman's syndrome indicated on HSG and who have menometrorrhagia, cervical diverticulum could be the etiology and might create obstacles to accessing the uterine cavity. IUI and transfer of the embryo to the uterus guided by US is the recommended procedure for helping these patients achieve pregnancy.
Footnotes
Acknowledgments
The authors wish to express their gratitude to the patient and the Infertility Department of Tehran University of Medical Sciences for their assistance in preparing this case report.
Approval of the ethics committee of the university for preparing this case report was obtained under the code IR.TUMS.MEDICINE.REC.1396.4109.
Author Disclosure Statement
No conflicts of interest exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.