
Abstract
Abstract
Objective:
Female pelvic organ prolapse (POP) is one of the main reasons for quality-of-life impairment in women. Urinary incontinence and sexual disorders are among the most frequent complaints. Several kinds of procedures in different surgical approaches exist but none has been accepted as a “gold standard.” The goal of this research was to assess a new technique, laparoscopic retrovesical colpopectinopexy (LRC) for POP.
Materials and Methods:
LRC was assessed for safety and long-term outcomes ina retrospective review of medical records and telephone call interviews of 22 consecutive patients who underwent LRC for POP from December 2011 through September 2015. LRC with use of polypropylen meshes was performed in all cases, using three trocars. All procedures were performed in one clinic by 1 surgeon. Age, comorbidities, operation times, blood losses, recovery of bowel functions, length of postoperative hospital stays, wound infections, and intra- and postoperative complications were recorded. All women were followed-up with telephone call questionnaires at 3 months and at 1 year. All women were asked to come in for observation at 1 year.
Results:
The mean operative time was 72 minutes (range: 44–121 minutes). There were no conversions for open surgery nor any intraoperative or postoperative complications. First bowel movements were observed on the first postoperative day (POD) in all women. All women were discharged from the hospital on POD 4. The questions asked during the follow-ups were: (1) “Do you have any complaints that could be related to the operation?” (2) “Did your problems recur?” (3) “Are you satisfied with the procedure overall?” All of the women's answers were negative for questions 1 and 2 and positive for question 3. At 1 year, 16 women were seen and were assessed with the Pelvic Organ Prolapse Quantification System. Persistence of POP was not observed. One patient with stage 3 POP was downgraded to stage 1.
Conclusions:
LRC is a safe and effective method for all types of cystocele repairs. It produces no intra- or postoperative complications. The operative time is short, and the procedure is easy to learn.
Introduction
F
In a 2006 article, Wagner et al. 1 concluded that there were no ideal techniques for POP treatment yet. Despite laparoscopic sacrocolpopexy (LSC) having promising results, this operation is very controversial. First, it is a time-consuming procedure related to quite severe complications, such as damage to the hypogastric plexus nerves, sacral veins, iliac vessels, ureters, rectum, and even intervertebral discs. Moreover, being rather technically demanding, the operation has quite a long learning curve. All of these facts restrict LSC from being widespread among surgeons. Therefore, alternative techniques are desirable. In addition, there are patients with anatomical abnormalities in the sacral promontorium vessels. In this setting, laparoscopic retrovesical colpopectinopexy (LRC) could be an operation of choice.
Materials and Methods
Study population
A retrospective review of medical records and telephone-call questioning of 22 consecutive patients who underwent LRC for POP from December 2011 through September 2015 was performed.
Preoperative evaluations included medical histories, physical examinations, and laboratory testing in all patients. Urodynamic and magnetic resonance imaging studies were not performed. Patients' demographics, clinical characteristics, and symptoms are reported in Table 1. The indications for LRC were primary POP, including cystocele, hysterocele, enterocele, or any combination of these conditions (Table 2).
Patients' Demographic and Clinical Characteristics
yr, years; BMI, body mass index; ASA, American Society of Anesthesiologists; IQR, interquartile range.
Characteristics of Pelvic Organ Prolapse
The POP grades according to the Pelvic Organ Prolapse Quantification (POP-Q) System classification are shown in Table 3. LRC was indicated for grades 2–3.
POP-Q Score in Patients
POP-Q, Pelvic Organ Prolapse Quantification.
Surgical technique for each patient
Preoperative preparation and instrumentation
Bowel preparation was not performed.
Two 5-mm and 1 10-mm trocars as well as an atraumatic grasper, harmonic scalpel, needle holder, pair of scissors, and dissector were used. A uterine manipulator was placed before starting the procedure. Polypropylene mesh was cut to 15–3 cm sizes.
Patient position and port placement
Under general anesthesia, a urethral catheter was placed. The patient was set in a lithotomy position with both legs on Allen stirrups and the arms tucked beside the body.
The 10-mm trocar was placed in the umbilicus, then two 5-mm ports were inserted on the right in McBurny's point and on the left (anti-McBurny's point) under direct vision. Thirty-degree 10-mm optics were used.
Dissection of plica vesicouterina
The harmonic scalpel in the surgeon's right hand was used to open the peritoneum between the vagina and urinary bladder (Fig 1A). (Filling the urinary bladder with 100–150 mL of normal saline can be helpful for visualizing obscure anatomy.) The retrovesical space was identified. Dissection proceeded downward along the anterior vagina wall until 2–3 cm of the vagina was completely free from the bladder (Fig 1B). The peritoneum was dissected along the round ligaments to the pubic bones (Fig 1C).

Dissection toward the pubic bone from the right side
Dissection of the peritoneum went laterally, crossing obliterated umbilical vessels toward the pubic bone. (Fig 1D). (Instrumental palpation of the bone could be helpful).
Dissection toward the pubic bone from the left side
Then, contralateral side dissection along the left round ligament as a border toward the pubic bone was performed (Fig 2A). There was no need to cut the umbilical vessels.
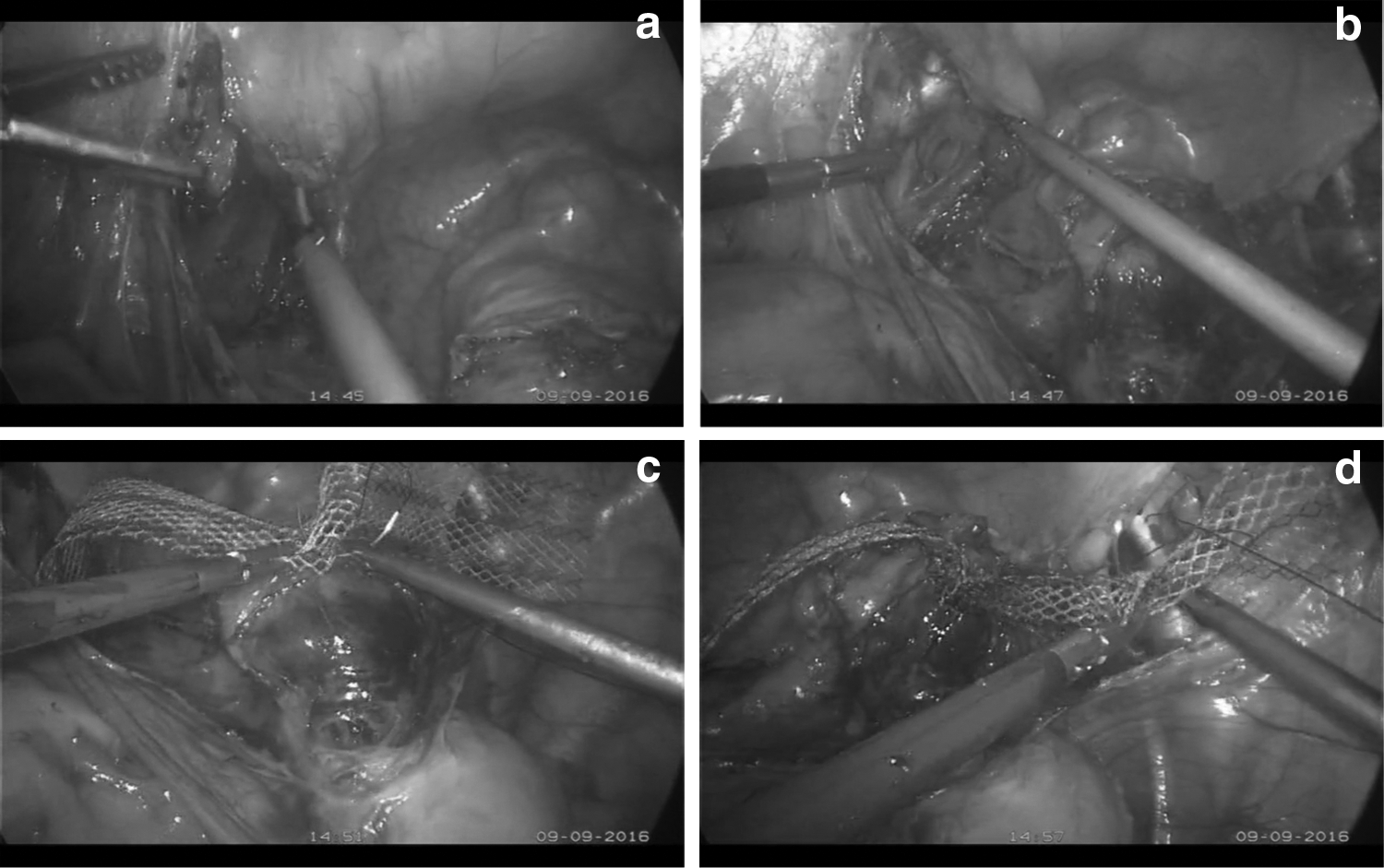
Complete dissection
A full dissection was considered when the anterior vaginal wall and both pubic bones were reached (Fig 2B).
Mesh placement
A piece of 15–3 cm polypropylene mesh was sutured from its middle to the vaginal wall with two 2/0 polypropylene sutures (Fig 2C). The cervix was taken into the sutures in cases of hysterocele. The right and left mesh sleeves were fixed to the pectineal ligament on the right and on the left sides using the same polypropylene suture (Fig 2D).
Peritonization
The peritoneum was closed with a continuous monofilament absorbable suture 3\0.
Postoperative course
A standard postoperative protocol was used in all cases. Nonsteroidal analgesics were used to address all pain complaints. No opioids were used. Single, short preoperative antibiotic prophylaxis was given. A urethral catheter was removed on the first postoperative day (POD). Fluid oral intake was started 6 hours after operation. A normal diet was given on the second POD.
Postoperative follow-up
Follow-up evaluation by telephone calls to question the patients were scheduled for 3 months and 1 year postoperation. All patients were asked to come in for observation at 1 year. Patients with complaints of urinary problems, signs of recurrences, or pelvic pain were also asked to visit.
Data analysis
Demographic data, preoperative clinical information, and perioperative data were collected from medical documentation on the patients. Treatment effectiveness was considered as “good” when no patients made complaints during the telephone calls. Descriptive statistics were carried out for the available variables. Categorical variables were reported as frequencies and percentages. Continuous variables were reported as median and interquartile ranges (IQRs).
Results
The mean operative time was 72 minutes (IQR: 44–121 minutes). No conversions for open surgery were detected. There were no intraoperative or postoperative complications or significant blood losses.
The first bowel movement was seen on POD 1 in all women. All were discharged from the hospital on POD 4. All of these patients were questioned during telephone calls at 3 months and 1 year after their operations. There were 3 questions: (1) “Do you have any complaints that could be related to the operation?”; (2) “Did your problems recur?”; and (3) “Are you satisfied with the procedure overall?” All of the women's answers were negative for questions 1 and 2 and positive for question 3. At 1 year, 16 women were seen and assessed by the POP-Q System. Persistence of POP was not observed. One patient with stage 3 POP was downgraded to stage 1 POP.
Discussion
LSC is a preferred method for correcting POP. There are a lot of articles providing LSC results.2–8 Although this operation has been performed by surgeons for more than 10 years, its mean operative time is ∼182 minutes.9,10 There are complications that are precisely related to LSC, such as rectal and ureter injuries, spondylitis, and bleeding of middle sacral veins or iliac vessels. Obstructed defecation, constipation, and even fecal incontinence after LSC are rare but serious complications as a result of hypogastric-nerve injuries. These facts do not let us recommend LSC as a “gold standard” for POP treatment.
There is no need to dissect the sacral promontorium and peritoneum along the hypogastric plexus during LRC. Even first cases had a mean operative time of 72 minutes, which was nearly two times shorter than the operative time of LSC. Moreover, with LRC, there were fewer chances to injure the hypogastric nerves, rectum, sacral veins, sacral discs, and ureters. These results could be basic points in surgical decision-making. Although we need more statistical data to judge this new technique's safety and efficacy, these first preliminary results offer a good basis for surgeons adopting this method.
Conclusions
LRC is a safe and effective method for all kinds of cystocele corrections. This procedure has not produced any intra- or postoperative complications thus far. The operative time is short, and the procedure is easy to perform. Further investigations are needed to evaluate the outcomes and feasibility of LRC.
Now, three centers are using this procedure in accordance with an investigation protocol. The first long-term results will be available in 2019.
Footnotes
Author Disclosure Statement
No financial conflicts exist.