
Abstract
Abstract
Objective:
Injury of the vessels of the anterior abdominal wall occurs in 0.2%–2% of laparoscopic surgeries, most commonly in the inferior epigastric artery (IEA). The objective of this study was to use surface landmarks on the abdominal walls of cadaver models to map areas of safe trocar placement to avoid injury to the inferior and superior epigastric arteries.
Materials and Methods:
This was a prospective, noncomparative study conducted at an anatomy laboratory in an academic university hospital. Twenty formalin-fixed cadavers were obtained by the anatomy laboratory from May 2017 to August 2017. The inferior and superior epigastric arteries were dissected bilaterally in all cadavers. The rectus sheath was divided for adequate exposure of the entire length of the arteries from the pubic bone to the costal margin. Two reference points were defined. Point A was halfway between the umbilicus and the anterior superior iliac spine. Point B was 3 cm below the costal margin on the midclavicular line (known as Palmer's point on the left side). The distance from Point A and Point B to the inferior epigastric artery and superior epigastric artery, respectively, were measured bilaterally.
Results:
Twenty formalin-fixed cadavers were dissected, for a total of forty epigastric arteries. Twelve female and 8 male cadavers were included. The mean distance from Point A to the IEA was 1.6 ± 1.0 cm. The artery was always on or medial to Point A. The mean distance from Point B to the superior epigastric artery (SEA) was 1.1 ± 0.6 cm. The SEA was always on or medial to Point B.
Conclusions:
In trocar placement during laparoscopic surgery, staying lateral to a vertical line drawn from Point A to Point B can avoid the inferior and superior epigastric arteries.
Introduction
V
There have been several studies on mapping the course of the epigastric arteries via computed tomography (CT) scanning.5–8 However, studies using cadaver models to trace the epigastric arteries have been limited. Several articles have focused on the IEA only.9–12 The IEA was found to be within 4–6 cm from the midline in most cadavers,9–11 or >66% from the midline to the anterior superior iliac spine (ASIS). 12 Only 2 cadaver studies dissected the SEA along with the IEA.13,14
None of the cadaver dissection studies identified clear surface landmarks that could be easily and reliably used in the clinical setting without a ruler to avoid the arteries during laparoscopy. Furthermore, very few studies included the SEA, which is also relevant to gynecologic surgery. The goal of this study was to identify areas on the anterior abdominal wall based on surface landmarks that are safe zones for trocar placement to avoid both the IEA and SEA.
Materials and Methods
Study design and participants
This study included 20 formalin-fixed cadavers acquired by the Surgical Science Laboratory (anatomy laboratory) at the University of California, Los Angeles, from May 2017 to August 2017. Cadavers are obtained by the university from the Donated Body Program for dissection, and simulated surgeries are done for training purposes. There was no change in the typical protocol for obtaining cadavers for this study. No living patients were involved; thus, this study was institutional review board–exempt. Inclusion criteria included both male and female cadavers that were already previously acquired by the university and had been used for teaching by the University's department of surgery. Exclusion criteria were cadavers that had been dissected extensively, such that the course of the epigastric arteries could not be identified.
Technique
Detailed dissections were performed on 20 cadavers to expose the anterior abdominal wall. Midline vertical incisions from sternum to pubic bone were made as well as transverse incisions at the level of the umbilicus to above the iliac crests bilaterally. The entire length of the IEA was dissected bilaterally from its origin from the external iliac artery. The SEA was also dissected bilaterally from its anastomosis with the IEA to the costal margin. The rectus sheath was divided carefully in order the expose the course of the artery.
Two reference points were identified bilaterally. Point A was defined as midway between the umbilicus and the ASIS. Point B was defined as 3 cm below the costal margin on the midclavicular line. This point is known as Palmer's point on the left side. 15 These points were marked with a pin traversing the full thickness of the anterior abdominal wall in a perpendicular manner. These points were thus clearly visualized on the underside of the abdominal wall where the epigastric arteries were dissected and visualized. Figure 1 shows Point A and Point B, with lines drawn from Point A to Point B bilaterally.
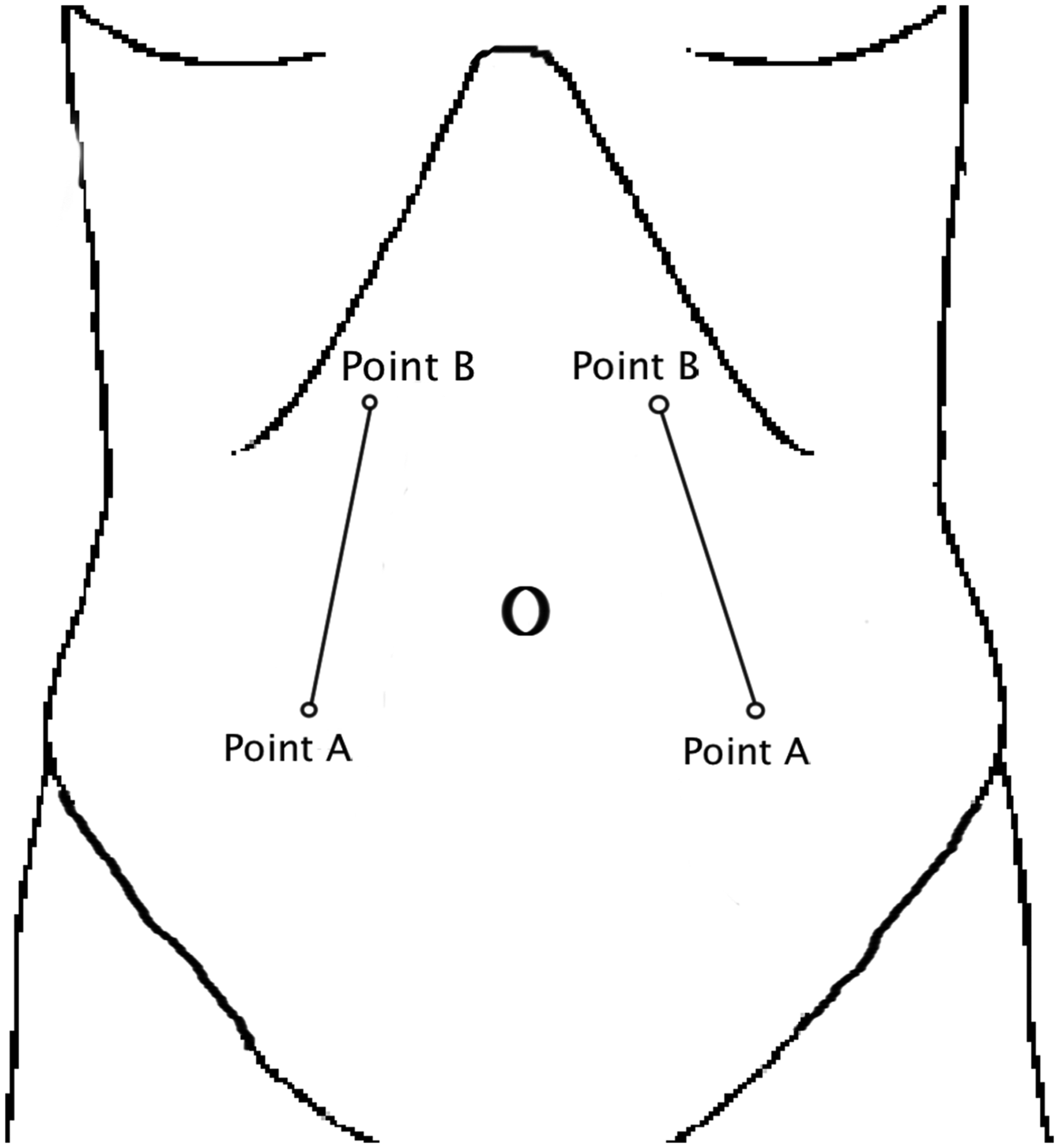
Safe zones for entry. Points A and B of the anterior abdominal wall, with lines drawn from Points A to B on each side.
Outcome measures
The primary outcome measures included the mean horizontal distance from Point A to the IEA (in cm), and the mean horizontal distance from Point B to the SEA (in cm). These dimensions were taken bilaterally from the posterior surface of the anterior abdominal wall, for a total of four measurements per cadaver. All measurements were taken twice, and rounded to the nearest tenth of a cm. Median distances were also calculated, along with standard deviations.
Results
The IEAs and SEAs were dissected bilaterally in 20 cadavers, for a total of forty epigastric arteries. Twelve female and 8 male cadavers were included. Table 1 includes all detailed individual measurements from Point A to the IEA and from Point B to the SEA for all twenty cadavers. Positive numbers indicated that the epigastric artery was medial to the reference points. Negative numbers would have indicated that the artery was lateral to the reference points; however, there were no negative numbers. Interestingly, Point A was always on or lateral to the IEA. Point B was also always on or lateral to the SEA.
These positive numbers indicate that the epigastric artery was medial to the reference points.
IEA, inferior epigastric artery; SEA, superior epigastric artery; F, female; M, male.
The mean distance from Point A to the IEA was 1.6 ± 1.0 cm, and the mean distance from Point B to the SEA was 1.1 cm ±0.6 cm. The median distances from Point A and Point B to the epigastric artery were 1.5 cm and 1.0 cm, respectively. Table 2 shows a summary of the primary outcome measures.
SD, standard deviation; IEA, inferior epigastric artery; SEA, superior epigastric artery.
The IEA and SEA were always on or medial to reference Point A or B. Thus, if a line is drawn from Point A to Point B, the epigastric artery was found to always be medial to this line (Fig. 1). Using this principle, placing trocars lateral to this line and above a line drawn from the umbilicus and the ASIS was very likely to avoid both the IEA and SEA during laparoscopic surgery.
Discussion
Palmer's point and the ASIS can be identified easily during laparoscopic surgery. Thus, these surface anatomical locations can be used reliably to guide surgeons in avoiding the epigastric arteries. The study was conducted to demarcate safe zones for avoiding arterial injury based on these simple landmarks. To accomplish this, careful dissection of the IEA and SEA was performed on cadavers to understand the full course of the vessels through the anterior abdominal wall.
Several cadaver studies have mapped the course of the IEA. Rao et al. described the dissection of 50 formalin-fixed cadavers, and measured distances from the IEA to 5 midline reference points: (1) the pubic symphysis; (2) the umbilicus, (3–5) and 3 points in between. 9 Distances from the IEA to the midline ranged from 1.2 cm to 6.9 cm. A recent study of 30 cadavers also measured the distances of multiple midline points to the IEA, and concluded that the artery is greater than a mean of 5.5 cm from the midline. 10 Epstein et al. similarly found that the IEA is 38% from the midline to the ASIS, and 40% from the midline to the midinguinal point. 11 A smaller study found that nerve and vessel injury is likely to be avoided if trocars are placed superior to the ASIS and more than 6 cm from the midline. 12
The two main limitations of the prior cadaver studies were: (1) only the IEA was mapped to the level of the umbilicus; and (2) the location of the IEA was given as the mean distances from arbitrary points, making it impractical to reproduce during surgery. In other words, the prior studies reported multiple mean measurements from the artery to the midline, but did not offer easily identifiable surface landmarks to make them clinically useful.
With advances in gynecologic laparoscopy, insertion of trocars in the upper abdominal quadrants is increasingly more common. Therefore, knowledge of the course of the SEA is increasingly important. 16 Often adhesions from prior abdominal surgery, large pelvic masses, numerous fibroids, or large uteri make it necessary to utilize the upper abdomen for laparoscopic entry rather than umbilical or subumbilical entry points. 17 Palmer's point is often underutilized due to lack of familiarity of many gynecologists with the anatomy of the upper anterior abdominal wall. 16 There have been limited cadaver studies on the course of the SEA, and these have been mainly in the general surgery literature.13,14 Again, these studies mapped the course of the SEA based on distances from multiple midline points, but did not offer guidelines based on surface landmarks to avoid the SEA.13,14
The main strength of the current study was that the entire IEA and SEA were dissected bilaterally in each cadaver. The reference Points A and B were used to create a safe zone where trocars can be placed to avoid both arteries. Point A, which is midway between the ASIS and umbilicus, can be estimated easily on the patient's abdomen. Point B is also readily identifiable at 3 cm below the costal margin on the midclavicular line (known as Palmer's point on the left side). Rather than measuring multiple mean distances from the midline, easily identifiable surface landmarks were used to demarcate safe areas for entry. Given that the IEA was always on or medial to Point A, and the SEA was always on or medial to Point B, placing trocars lateral to a line drawn from Point A to Point B is likely to avoid the epigastric arteries.
Note that caution should be used when applying these findings clinically. With an improper trocar placement technique, the trocar can skive medially and still injure the epigastric arteries. Hence, even if the trocars are placed in the safe zone on the skin, medial deviation of the trocar's trajectory can cause vessel injury. Thus, it is imperative that surgeons place trocars carefully, perpendicular to the skin and fascia. Another limitation is that the cadaver abdomens were not insufflated as they are in laparoscopic surgery, which might change the position of the epigastric arteries.
Conclusions
The results of this research suggest relative safe zones for laparoscopic entry that are clinically applicable. Safe zones were demarcated for both the lower and the upper abdominal quadrants.
Footnotes
Acknowledgments
The authors would like to acknowledge the kind people who participated in the Donated Body Program for academic advancement, research, and education.
Author Disclosure Statement
The authors report no conflicts of interest.