
Abstract
Abstract
Background:
The recommended treatment for patients with locally advanced cervical cancer is primary chemoradiation, which consists of platinum-based chemotherapy, external-beam radiation therapy (EBRT) to the pelvis, and cervical brachytherapy.
Case:
The patient was a 50-year-old woman had a large, fungating cervical mass. Pathology testing showed that it was a poorly differentiated squamous carcinoma. Computed tomography (CT) and magnetic resonance imaging showed a 14-cm, complex, central endometrial mass that perforated the superior uterine fundus and extended into a 13 × 10.4–cm abscess. An examination under anesthesia with diagnostic laparoscopy revealed a 5-cm cervical mass with extension to the left parametria but not extending to the side wall. There were also significant adhesions in the pelvis, making evaluation of it or drainage of the collection impossible. Definitive chemoradiation was considered. It was proceeded by CT-guided drainage of the abdominal abscess. She underwent EBRT with concurrent cisplatin. A repeat CT scan showed resolution of the cervical mass, but the anterior wall of the uterus was still perforated. Standard tandem/ring cervical brachytherapy for definitive chemoradiation was not safe in the presence of the uterine perforation. The patient underwent a total abdominal hysterectomy and bilateral salpingo-oophorectomy 1 month after completion of her EBRT. Following surgery, the vaginal cuff was treated with intracavitary brachytherapy.
Results:
Repeat CT scans and surveillance examinations have shown no evidence of recurrence.
Conclusions:
For locally advanced cervical cancer, EBRT with concurrent chemotherapy, followed by surgery and vaginal-cuff brachytherapy is a reasonable option for patients in whom tandem and ring intracavitary brachytherapy is not possible.
Introduction
C
The objective of this report is to present a case of a stage IIB squamous-cell carcinoma (SCC) of the cervix, which was associated with uterine rupture and an intra-abdominal abscess at the time of diagnosis, and review the use of an alternative treatment regimen for a patient in whom intracavitary tandem/ring brachytherapy was deemed to be unsafe.
Case
The patient was a 50-year-old previously healthy woman who presented to her gynecologist reporting malaise and pelvic pain. She was diagnosed with a tubo-ovarian abscess, and treated with a 3-week course of intravenous antibiotics. A pelvic ultrasound (US) performed 1 month after that initial diagnosis showed an enlarged 18-cm uterus with a 6.4-cm heterogeneous, endometrial, complex cervical mass. The adnexa were normal and there was no free fluid in her pelvis. In order to assess these US findings further, the patient was examined under anesthesia, which revealed a large endophytic, fungating cervical mass with extension to the left parametria. The uterine cavity was not entered. Biopsies taken were consistent with moderately differentiated squamous carcinoma of the cervix.
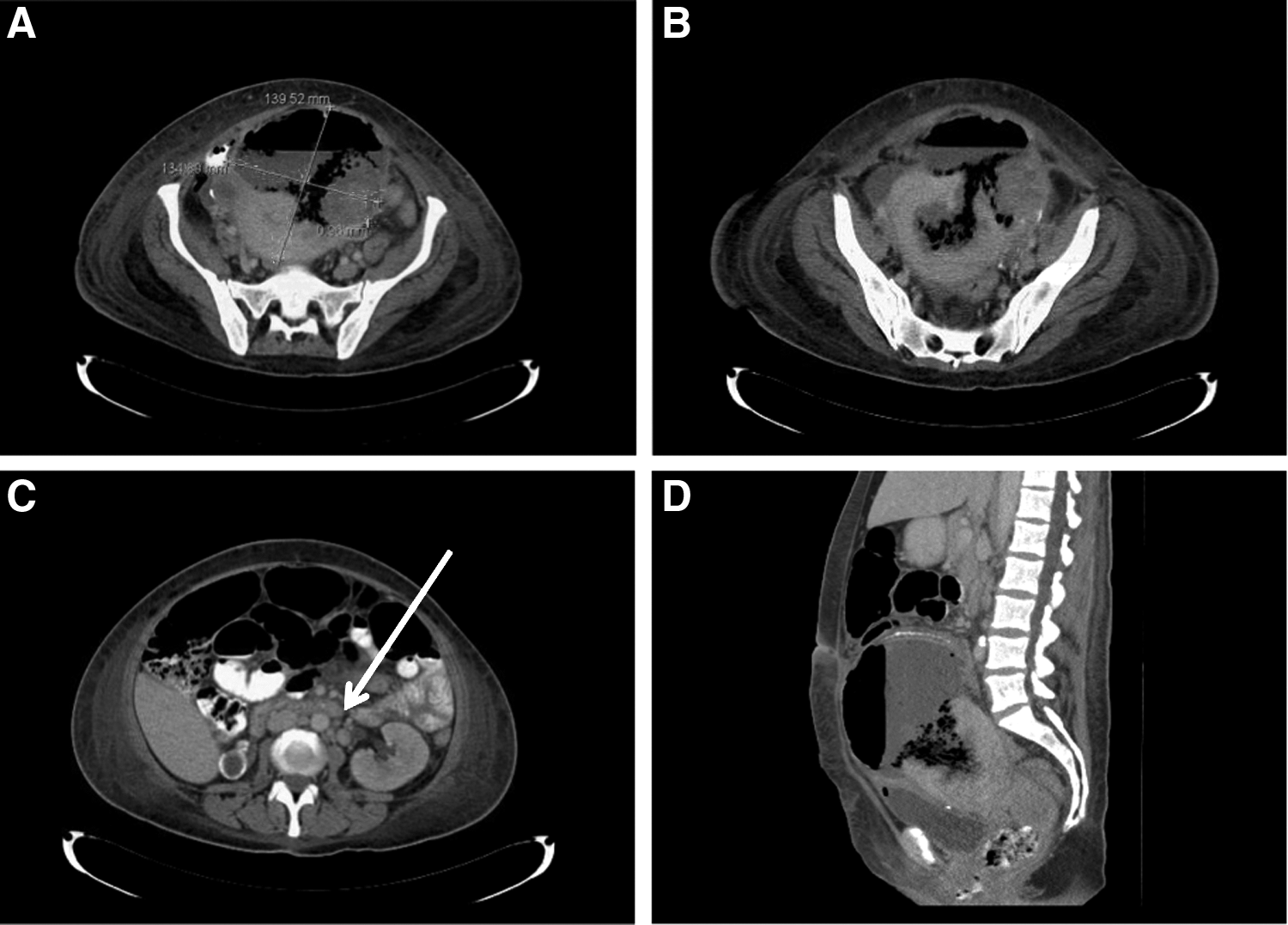
Two days following the cervical biopsies, the patient returned to the hospital with heavy vaginal bleeding, which was stabilized with ferric subsulfate solution and vaginal packing. Her admission laboratory values were significant for acute blood-loss anemia and acute kidney injury (AKI) with a creatinine level of 1.82 mg/dL. A markedly elevated white blood–cell count of 36.9 K/mcL was also noted. She was transfused with a total of 4 units of red blood cells while her vaginal bleeding stabilized. The AKI was likely prerenal in the setting of acute blood-loss anemia and resolved with hydration; the AKI was not directly due to the cervical tumor extension and, therefore, the patient's stage was not altered by this finding. Computerized tomography (CT) scan findings included a 5.2-cm cervical mass and an enlarged para-aortic lymph node just inferior to the renal vessels (Fig. 1). Also noted on CT was an area of uterine perforation at the uterine fundus, communicating with a 14.5-cm intra-abdominal abscess (Fig. 1). Given the complexity of this patient's presentation, and her known cervical malignancy, she was transferred to a tertiary center for care by a gynecologic oncologist.
After transfer, this patient was taken to the operating room for examination under anesthesia and diagnostic laparoscopy. Operative findings included a 4-cm aborting fibroid mass arising from the endocervix, and an endophytic cervical mass with extension to the left parametria but not extending to the pelvic side wall. On laparoscopy, there were significant large and small-bowel adhesions, making evaluation of the pelvis or drainage of the collection impossible. Findings were discussed at a divisional tumor conference and the decision was made to offer definitive chemoradiation to her. Prior to initiation of chemoradiation, she underwent CT-guided drainage of the abdominal abscess and was treated with a 2-week course of antibiotics.
Radiation therapy was initiated urgently to prevent further vaginal bleeding, which had been reduced with packing. Her initial EBRT plan was an AP/PA 2-field plan to the pelvis and para-aortic lymph nodes. Twelve Gy in 3 fractions were administered with this plan. After these 3 fractions, a 4-field three-dimensional plan was designed to encompass the pelvis and para-aortic lymph nodes. An additional 32.4 Gy in 1.8 Gy per fraction was delivered with this plan. She received 2 doses of weekly concurrent cisplatin at a dose of 40mg/m2.
After completion of EBRT and cisplatin, a repeat CT scan showed resolution of the cervical mass and a decrease in size of the fluid collection to 6.6 × 6.9 cm. Yet, there was a persistent defect in the anterior wall of the uterus. It was felt that standard tandem and ring cervical brachytherapy for definitive chemoradiation was not safe in the presence of a uterine perforation. Thus, a decision was made to proceed with a total abdominal hysterectomy and a bilateral salpingo-oophorectomy 1 month after completion of EBRT (Fig. 2). At the time of surgery, there was no gross disease and pathology testing revealed no residual carcinoma. Following surgery, the vaginal cuff was treated with intracavitary brachytherapy via vaginal cylinder to 12 Gy in 3 fractions.

Two gross surgical specimens at time of total abdominal hysterectomy showing uterine rupture at the left cornua.
Results
One year after completion of treatment, this patient continued to have no evidence of disease. Routine surveillance examinations and a 6-month vaginal Papanicolaou smear yielded negative results. Nine months post-treatment, the patient developed symptoms of chronic bowel obstruction. She underwent an exploratory laparotomy and resection of a portion of her small bowel for acute small-bowel obstruction. At that time, there was no gross or histologic evidence of disease.
Discussion
This case illustrates the use of an alternative treatment regimen for locally advanced cervical cancer. This was a unique case of cervical cancer in which uterine perforation and an intra-abdominal abscess were found at the time of diagnosis, using CT scanning. The abscess posed a challenge because definitive therapy with chemoradiation could not commence with an active intra-abdominal infection. Although the abscess could not be drained during the diagnostic laparoscopy, coordination with interventional radiology specialists led to successful CT-guided drainage and treatment with antibiotics. The uterine perforation limited the feasibility of conventional definitive chemoradiation with brachytherapy due to safety concerns regarding placement of a tandem in a perforated intrauterine cavity. The patient was treated successfully with an alternate approach: EBRT with concurrent cisplatin, then hysterectomy followed by vaginal cuff brachytherapy.
Completion hysterectomy after chemoradiation remains controversial. Results of small retrospective and prospective studies indicate possible reduction of local disease and decreased risk of recurrence with completion hysterectomy.6–8 However, a randomized controlled trial showed no change in event-free survival and overall survival in patients who have had complete clinical responses after primary treatment. 9 Furthermore, studies have shown a higher risk of complications in patients treated with completion surgery after CCRT. In particular, studies have reported a significant number of grade 2 or greater genitourinary or gastrointestinal complications, ranging from 9% to 26%. Bowel and bladder complications are among the complications described.10,11 It is notable that, in the current case, the patient had a major bowel complication requiring surgical intervention. Although, it is difficult to discern if her adhesive disease was a result of multimodal therapy or an inflammatory response to her large intra-abdominal abscess.
Completion hysterectomy has largely been reserved for situations with a higher risk for relapse, such as bulky disease, lower uterine-segment involvement, or evidence of post-treatment residual disease. A retrospective review showed that with every 1-cm increase in cervical diameter (3–9 cm) there was a threefold increase in the risk of recurrence. Therefore, a completion hysterectomy might be a reasonable treatment option in certain cases of bulky disease.8,12 Another important clinical scenario is when brachytherapy is unavailable, such as in developing countries, where there is often a lack of brachytherapy equipment and qualified professionals. 13 Researchers, conducting a randomized trial of more than 200 women, sought to demonstrate that radical hysterectomy results in improved survival, compared to brachytherapy following concurrent chemotherapy and EBRT. After a median follow-up time of 36 months, progression-free survival, overall survival rates, and complications were similar between the 2 study arms. 14 A retrospective analysis of patients with stage III cervical cancer confirmed noninferiority of hysterectomy, compared to brachytherapy, with no statistical difference in disease-free survival and overall survival in these more-advanced stage patients. 15 These studies provide compelling data to support offering a completion hysterectomy when brachytherapy is considered unsafe or unavailable for a patient.
Conclusions
For locally advanced cervical cancer, EBRT with concurrent chemotherapy followed by surgery and vaginal-cuff brachytherapy is a reasonable option for patients in whom tandem and ring intracavitary brachytherapy is not possible.
Footnotes
Acknowledgments
The authors extend thanks to the Department of Gynecology and Oncology of the Mount Sinai Health System, New York.
Author Disclosure Statement
Drs. Kelsey Murphy, Elena Pereira, Vishal Gupta, and Linus Chuang have no commercial associations, competing financial interests, or conflicts of interest to disclose.