
Abstract
Abstract
Background:
Immune thrombocytopenic purpura (ITP) is characterized by a low platelet count with severe bleeding risks. ITP has a complex pathogenesis of platelet destruction due to autoantibodies binding on platelet antigens and sometimes to their precursors. In adults, ITP is mostly a chronic disease. This report describes the recovery of a patient with ITP after cystectomy of a dermoid cyst.
Case:
A 21-year-old woman complained of progressive petechia and minor bleeding. Laboratory evaluation showed isolated deep thrombocytopenia. She was diagnosed with primary ITP and treated with prednisone and later with intravenous immunoglobulins (IVIgs). There was a good response to the IVIgs and her platelet count increased, but, in between two courses of IVIg, her platelets decreased again. Meanwhile, because of dyspepsia, an abdominal ultrasound was performed, on which an ovarian cyst was seen. Cystectomy was performed on the cyst.
Results:
After the cystectomy, the thrombocytopenia resolved spontaneously, and treatment with IVIg was discontinued. A literature search on
Conclusions:
Complete spontaneous remission of ITP after dermoid cystectomy has not been described before. Diagnostic imaging and treatment of dermoid cysts can be considered in patients with chronic ITP.
Introduction
I
Symptoms can vary from just a few petechia to major gastrointestinal (GI) or intracranial bleeding. There are many causes of thrombocytopenia; in diagnostic work-ups, these causes should be excluded. Low platelets can be caused by reduced production in cases of drugs being used, lymphoproliferative diseases, thyroid dysfunctions, or vitamin deficiencies. Thrombocytopenia may also arise from high consumption or degradation of platelets, as seen in systemic autoimmune diseases (e.g., systemic lupus erythematosus), infections (e.g., Epstein–Barr virus), use of heparin, hypersplenism, or coagulation disorders (e.g., von Willebrand's disease). In case of an underlying disease, treatment of the disease is indicated to treat ITP.
ITP treatment is focused on prevention of serious bleeding. In general, treatment is started if the platelet count is below 30 × 109/L or in cases of bleeding complications. The first-line treatment is corticosteroid therapy. In cases of therapy failure, other regimens can be considered. Second-line treatments are a thrombopoietin(TPO)-receptor agonist, a splenectomy, and rituximab, which is an anti-CD 20 antibody. In cases of therapy failure, other immunosuppressive drugs are used with variable results. In cases of severe life-threatening bleeding, intravenous immunoglobulin (IVIg) is used. In cases of low immunoglobulin(Ig)G levels, such as in common variable immune deficiency (CVID), IVIg is used.
The disease can resolve spontaneously in 6 months, which is more common in children. It is called chronic ITP when the disease exists for more than 12 months, which is more common in adults. In summary, ITP is a chronic autoimmune disease with an increased bleeding risk with—although rare—life-threatening bleeding events requiring treatment and anticipation to stop severe bleeding.
Case
A 21-year-old woman complained of having progressive petechia on the extremities and gingival bleedings for 1 year. There was no hematuria, epistaxis, or GI bleeding. She had no remarkable medical history. A laboratory evaluation showed isolated deep thrombocytopenia (a platelet count of 15 × 109/L). Viral serology and antinuclear-antibodies were negative; there was no other explanation for her thrombocytopenia. She was diagnosed with primary ITP, which was treated with 60 mg/kg of prednisone. At first, her platelet count increased to 159 × 109/L, but, in a few weeks, it decreased to 70 × 109/L. Because of this relapse during treatment, she was referred to a tertiary center. Here, the relapse was interpreted as being caused by phasing out the prednisone too early, so the prednisone was started again. Her platelet count decreased further to 6 × 109/L and, because of the combination with low IgG (due to prednisone use), treatment with IVIg was started. The presence of CVID was excluded. She had a good response to the IVIg and her platelet count increased. In between two courses of IVIg, her platelet count decreased again. Treatment with IVIg was continued.
Meanwhile, this patient developed of dyspepsia and stomach pain. She had a diagnostic gastroscopy, which revealed no explanation for her symptoms. The presence of Helicobacter pylori was excluded. An abdominal ultrasound was performed, on which a 60-mm heterogeneous polycystic abnormality in the lower abdomen was seen.
A gynecologic ultrasound showed a multilocular cyst in the pouch of Douglas that was 64 × 55 mm, with lucid content and without flow, which was most likely to be a dermoid cyst. The patient was informed about the possibilities and risks of treatment, and a decision was made to perform a laparoscopic cystectomy. Two days before surgery, the patient's platelet count was 149 × 109/l (she was still undergoing IVIg treatment). She underwent laparoscopic cystectomy, during which bilateral cysts were seen and resected (Fig. 1). Histology testing showed characteristics of dermoid cysts.
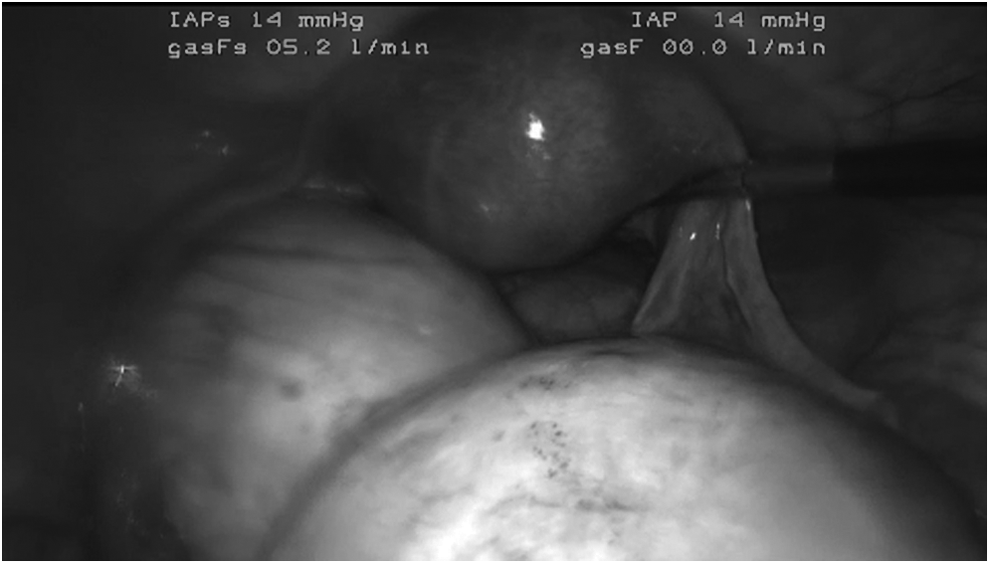
Dermoid cysts during laparoscopy.
Results
Three weeks after surgery, before a new IVIg course was planned, a routine estimation of the platelet count appeared to be 421 × 109/L. The IVIg infusion was canceled. Since then, this patient's platelet count remained normal and stabilized at ∼300 × 109/l. There were no signs of hemorrhage any more, and the patient was discharged.
Discussion
In the case described above, there was a complete remission of ITP after cystectomy of bilateral dermoid cysts. Dermoid cysts are common in young or middle-age women; the exact prevalence is unknown. Of all ovarian neoplastic masses, 10%–25% are mature cystic teratomas, which is nearly 70% of all benign masses. 2 The current patient had bilateral cysts, which occur in 10%–20% of all cases. A dermoid cyst arises from pluripotent ovarian cells; thus, this cyst is categorized as a germ-cell tumor. Perhaps genetic predisposition plays a role in the pathogenesis of these cysts. 3 The tissue is well-differentiated; contains sebum; and, in the tumor, structures such as thyroid tissue, bones, or hair can be found. The risk of malignant degeneration is very low, ∼1%–2%. Detection of tumor markers (i.e., cancer antigen–125, with a specificity of 86%), in serum can be part of the differentiation between a malign or benign mass.
Possible symptoms consist of abdominal pain and the consequences of growth, such as constipation, when the cyst obstructs parts of the intestine. Although, 20%–60% of all patients with dermoid cysts do not have any symptoms, any symptoms related to the cyst are an indication for surgery. As in the current case, the cysts are mostly found incidentally on imaging for nongynecologic indications. 4
The main point of discussion in the current case is the question about the cause of the remission of ITP. Was the dermoid cyst the cause of the ITP or are there other explanations?
At first, it could be a coincidental spontaneous remission. As mentioned above, in adults ITP is mostly a chronic disease. When there is resolution of the ITP, this is usual within the first 6 or 12 months. In the current case, the disease was already chronic. In a retrospective cohort study in 1996, 208 patients with chronic ITP were analyzed to define their response to therapy and the overall outcome of the disease. 5 There were 3 groups: (1) wait-and-see; (2) prednisone; or (3) splenectomy when prednisone failed. The researchers found a relatively high rate (8 of 87 patients; 9.2%) of spontaneous resolutions of the ITP. However, there were no spontaneous remissions reported in the patients with indications for treatment. The same results were seen in elderly patients as reported in a study in 2013. 6 There are only 3 cases described of late “spontaneous” remissions after intensive treatment—1 case with romiplostim (a TPO-agonist) and 2 cases with corticosteroids—of severe refractory chronic ITP.7,8 In the current patient with chronic ITP, there was a good response to IVIg. Based on the duration of disease, a spontaneous remission was not expected.
Based on the current patient's response after cystectomy. a relationship between her ITP and dermoid cysts was suggested. A literature search on
Conclusions
There was a complete remission of ITP after cystectomy of bilateral dermoid cysts in a patient with chronic therapy-dependent ITP. This type of case and resolution has never been described before, and there is no shared pathophysiology known for ITP and dermoid cysts. More cases or pathophysiologic knowledge are needed to justify diagnostic imaging to search for dermoid cysts and to initiate treatment of these cysts in patients with chronic ITP.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.