
Abstract
Abstract
Objective:
Pelvic organ prolapse (POP) is common and has a high incidence of recurrence. Thus, there is a need for procedures that have higher rates of first-time success and attractive safety profiles. The aim of this study was to assess how well the Exair® (Coloplast, Humlebæk, Denmark) transvaginal mesh system corrected POP.
Materials and Methods:
This was a prospective analysis of patients who received Exair transvaginal mesh between June 2013 and August 2015 for POP. Patients with uterine prolapse underwent vaginal mesh hysteropexy. A composite score that included subjective criteria of absence of a bothersome bulge, no prolapse below the hymen, and no retreatment was used to assess success.
Results:
Transvaginal mesh was inserted in 80 patients (age 67 ± 9.2 years; body mass index 28.56 ± 5.18 kg/m2). Four patients (5%) received anterior mesh, 14 received (17.5%) posterior mesh, 61 (76.25%) received both anterior and posterior mesh—all via the Exair system—and 1 patient had a modified Exair surgery. Stage II prolapse was noted in 3 (3.75%) patients, 26 (32.5%) had stage III prolapse, and 51 (63.75%) had stage IV prolapse. The composite success score was 93% at a 1-year follow-up. Hysteropexy success was 93.5%. Mean operative time was 156.75 ± 47.35 minutes. Mean intraoperative blood loss was 181.89 ± 138.77 mL. There were 3 (4.2%) cases of mesh exposure in the vagina. There were no visceral injuries, and no cases of de novo dyspareunia, vaginal-wall retraction, voiding dysfunction, or de novo incontinence.
Conclusions:
Exair mesh is a good option for managing POP.
Introduction
P
In the United States alone, more than 300,000 surgeries for pelvic organ prolapse are performed each year, of which anterior colporrhaphy for prolapse of the anterior vaginal wall (cystocele) is the single most common operation.
Native tissue repairs, especially of the anterior wall, are associated with a high risk of recurrence of almost 70%. 3 Whiteside et al. also noted that 58% of such patients had recurrent prolapses 1 year after this kind of surgery. 4 Therefore, synthetic material has been incorporated into these repairs to improve surgical outcomes.5,6
Although mesh surgery can result in good anatomical success, this might not necessarily imply better functional outcome,7,8 and, therefore, the focus is shifting from anatomical success to functional improvement and patient satisfaction following a surgical intervention.
This article reports on the Exair® (Coloplast, Humlebæk, Denmark) transvaginal mesh system for repairing POP. Exair is lightweight Novasilk® Mesh (Coloplast), a knitted, monofilament, macroporous polypropylene mesh with a weight of 23 g/m2 and a pore size >600 μ.
The primary objective of this study was to assess success based upon both subjective and objective criteria at 1 year after Exair vaginal-mesh surgery was performed to correct POP, and then specifically for patients who had uterine prolapse and underwent hysteropexy. Secondary objectives were to assess complications and the impact of surgery on urinary incontinence, vaginal healing, and sexual function.
Materials and Methods
This was a prospective study involving 80 patients who underwent Exair transvaginal mesh surgery from June 2013 to August 2015. The patients were followed at 4 weeks, 6 months, and 12 months postoperatively.
The study was approved by the western institutional review board. Informed consent was obtained from all patients. Funding for this study was provided through an investigator-initiated research grant from Coloplast, the manufacturer of the Exair mesh. Coloplast, however, had no role in the design, implementation, analysis of data, or in the writing of this article.
All eligible patients underwent a detailed urogynecologic history taking and examination, including a Pelvic Organ Prolapse Quantification system assessment (POP-Q). 9 All definitions and descriptions conformed to the International Continence Society standards. 9 The patients completed validated questionnaires at preoperative and postoperative visits. The Pelvic Floor Distress Inventory–short form 20 (PFDI-20) was used as a symptom-specific questionnaire for POP. 10 The Urogenital Distress Inventory–short form 6 (UDI-6) and the Medical Epidemiological and Social aspects of Aging (MESA) 11 forms were used to assess associated urinary-incontinence symptoms. The Prolapse/Urinary Incontinence Sexual Questionnaire–short form-12 (PISQ-12) 12 was used to assess sexual function. Scores of the PFDI-20 were calculated in a simple additive fashion in which a higher score indicates more distressful symptoms. 13 The Dindo Classification for reporting complications was also used in this study. 14
Success was defined by a composite score that comprised the following:
The leading edge of the prolapse was above the hymen, AND On the PFDI question number 3 (“Do you usually have a bulge or something falling out that you can see or feel in the vaginal area?”), the patient answered “No,” or, if “Yes,” “Not at all bothersome,” AND No reintervention (surgery or pessary) for POP.
To be a success, a patient's case had to meet all the above criteria.
The inclusion criteria were patients desiring surgery for stage II or greater prolapse and symptoms of a bothersome vaginal bulge. The exclusion criteria included any physical or mental limitation that precluded a patient's participation or inability to give informed consent. All patients with anterior vaginal wall prolapse, symptoms of urinary incontinence, or voiding dysfunction underwent urodynamic testing that was performed in a standardized fashion. Occult stress urinary incontinence was assessed via urodynamics by elevating the prolapsed anterior vaginal wall to simulate postsurgical repair. Intraoperative cystoscopy was performed in all patients with anterior or total mesh surgeries or in patients undergoing concomitant sling procedures.
The anterior Exair procedure was performed through an anterior vaginal-wall incision with dissection into the paravaginal space and attachment of the distal arm of the mesh to the anteromedial portion of the obturator muscles with an exit through the groin and the proximal mesh arm to the sacrospinous ligament with an exit through the buttocks. The posterior Exair procedure involved a posterior vaginal wall incision with dissection into the pararectal spaces, attachment of the Exair arms to the sacrospinous ligaments, and an exit through the buttocks via the ischioanal fossa. The main purpose of the posterior Exair procedure was for apical support more than for rectocele management. If the procedure was done for a rectocele, then the procedure was performed in cases wherein the rectovaginal fascia was noted to be significantly attenuated at the time of the repair. Total Exair surgery was essentially the anterior Exair and the posterior Exair performed simultaneously. If the uterus was present and was prolapsing (C > −1), the apical portions of the anterior and posterior Exair mesh were attached to the front and back of the cervix, respectively, with at least two 2–0 Prolene® sutures. This was performed to correct the uterine prolapse (this procedure is termed hysteropexy in this article).
For any patient with posthysterectomy vaginal vault prolapse, the anterior and posterior Exair mesh were stitched together in to form one continuous mesh. This apical portion of the combined mesh was sutured to the remnants of the uterosacral ligaments on each side with a 2–0 Prolene suture in order to prevent recurrence of an enterocele. The mesh was appropriately trimmed to ensure that it lay flat. After the vaginal incisions were closed, the mesh arms were pulled to remove any slack, and then the arms were cut flush with the buttock and the groin incisions. A rectal examination ensured that the mesh arms were not too tight.
In 1 patient who was scheduled for a total Exair procedure, the anterior Exair procedure could not be performed due to abnormal vascularity of the paravaginal space; the mesh arms were cut and the mesh was sutured to the obturator internus. The posterior mesh procedure was performed in the usual fashion. This patient was referred to as undergoing a modified Exair procedure. None of the patients in this study underwent hysterectomy. The information for use of Exair helped as a guide; however, some modifications—such as attaching the apical portion of the mesh to the cervix, laterally to the pubococcygeus muscle, and appropriately trimming the mesh to conform to each patient's vagina—were performed by the author.
For the secondary-outcome analysis, bothersome de novo incontinence was defined as new-onset incontinence that required intervention. Mesh retraction, banding, or tenderness was determined by a vaginal examination and total vaginal length (TVL) measurements via POP-Q during the postoperative visits. Vaginal examination was performed to assess for any banding or constriction of the vagina.
Data on patients and surgical characteristics are presented as numbers with corresponding percentages or means ± standard deviations with ranges. A repeated-measures analysis of variance and a Wilcoxon signed-rank test were used for analysis. A p-value of <0.05 was considered to be statistically significant. The Statistical Package for the Social Sciences, version 18, was used (SPSS Inc., Chicago, IL).
Results
Transvaginal Exair mesh surgery was performed in 80 patients to correct POP from June 2013 to August 2015. Of these patients, 71 (88.8%) were seen at a 12-month visit. Total (anterior + posterior) Exair was performed in 61 (76.3%) patients, 14 (17.5%) underwent posterior Exair, 4 (5%) underwent anterior Exair, and 1 (1.25%) underwent a modified Exair procedure. Stage II prolapse was noted in 3 (3.75%) patients, 26 (32.5%) had stage III prolapse, and 51 (63.75%) had stage IV prolapse. Fifty patients had uteri. Exair hysteropexy was performed in 46 of 50 (92%) patients, as they had uterine prolapse (C> −1). The remaining 4 patients did not have uterine prolapse. Of the patients who underwent hysteropexy, none had stage II uterine prolapse, 11 (24%) had stage III uterine prolapse, and 35 (76%) had stage IV uterine prolapse. The mean preoperative C value for the hysteropexy patients was +5.05. Detailed demographics and surgical characteristics for the study patients are presented in Table 1.
Patient Demographics and Surgical Characteristics
Coloplast, Humlebæk, Denmark.
Mean ± standard deviations (range).
Number of patients (%).
BMI, body mass index; min, minutes; TVT-O, tension-free vaginal tape, transobturator approach
The composite success score was 93% (66 of 71 patients). When assessed by preoperative POP-Q stage of prolapse, the composite success scores were as follows: stage II, 1 of 2 (50%); stage III, 21 of 23 (91%); and stage IV, 43 of 46 (93.5%). When assessed by the type of Exair procedure, the breakdown of the composite success scores were: total Exair, 52 of 54 (96.3%); posterior Exair, 9 of 12 (75%); anterior Exair, 4 of 4 (100%); and modified Exair, 1 of 1 (100%).
Specifically, for Exair hysteropexy, the success rate was 43 of 46 (93.5%). The preoperative and postoperative POP-Q stages are listed in Table 2. Distributions of preoperative and postoperative POP-Q values are listed in Table 3.
Stages of Prolapse and Type of Exair a Surgery
Coloplast, Denmark.
Distribution of POP-Q Values Preoperatively and Postoperatively (at 12 months)
Coloplast, Denmark.
Stages: Aa, anterior vaginal wall 3 cm proximal to hymen; Ba, most distal point of anterior vaginal wall prolapse; C, cervix or cuff; D, posterior fornix; Ap, posterior vaginal wall 3 cm proximal to hymen; Bp, most distal point of posterior vaginal wall prolapse; GH, genital hiatus; PB, perineal body; TVL, total vaginal length.
Mean (± standard deviation).
p-Values were calculated using repeated measures analysis of variance and compared preoperative and postoperative results for all patients.
POP-Q, Pelvic Organ Prolapse Quantification; op, operative; N/A, Not applicable.
Failures were mainly of the contralateral untreated compartment (3 of 5, 66%). All 3 patients had undergone posterior Exair procedures and then developed prolapses of the untreated anterior vaginal walls.
There was significant improvement in all the parameters and subscores of the PFDI-20 in the postoperative period, compared to the preoperative period. Moreover, there was no statistically significant difference in these scores between the 6 and 12-month postoperative periods (Table 4). There was also statistically significant improvement in the MESA total score and the MESA stress subscale score. The mean preoperative MESA score was 13.13 and the mean postoperative score was 9.42 (p < 0.008). The mean preoperative MESA stress subscale score was 8.38 ± 7.15 and the postoperative subscale score was 5.52 ± 5.64 (p = 0.002).
Preoperative Versus Postoperative Total & Subscales of PFDI-20 and MESA
Mean ± standard deviation.
p values were calculated using repeated measures analysis of variance and compared preoperative and 6-month and 12-month postoperative results.
PFDI-20, Pelvic Floor Distress Inventory–short form 20; MESA, Medical Epidemiological and Social Aspects of Aging; POPDI, pelvic organ distress inventory; CRADI, colorectal–anal distress inventory; UDI-6, Urogenital Distress Inventory–short form 6.
There were no intraoperative complications. There were no visceral injuries. Cystoscopy was normal without any injuries. The average hospital stay was 1.7 days. The mean blood loss was 181.89 ± 141.85 mL, and no patients received blood transfusions. There were no cases of postoperative hematomas. Three of 71 (4.2%) patients had mesh exposure in the vagina. Of these patients, 2 underwent excision of the exposed vaginal mesh in the operating room, whereas 1 had only a 1-mm exposure and was managed expectantly. There were no cases of mesh erosions into the urethra, bladder, or rectum.
In this study, only 19 of the 71 patients were sexually active and none of these patients developed de novo dyspareunia. The details of sexual activity and dyspareunia are shown in Figure 1. Patients who were sexually active and did not have dyspareunia preoperatively, did not develop de novo postoperative dyspareunia. In those who had preoperative dyspareunia, 2 of the 6 patients had resolution. Of the 9 patients became sexually active postoperatively, 7 had no dyspareunia, while 2 complained of having dyspareunia.
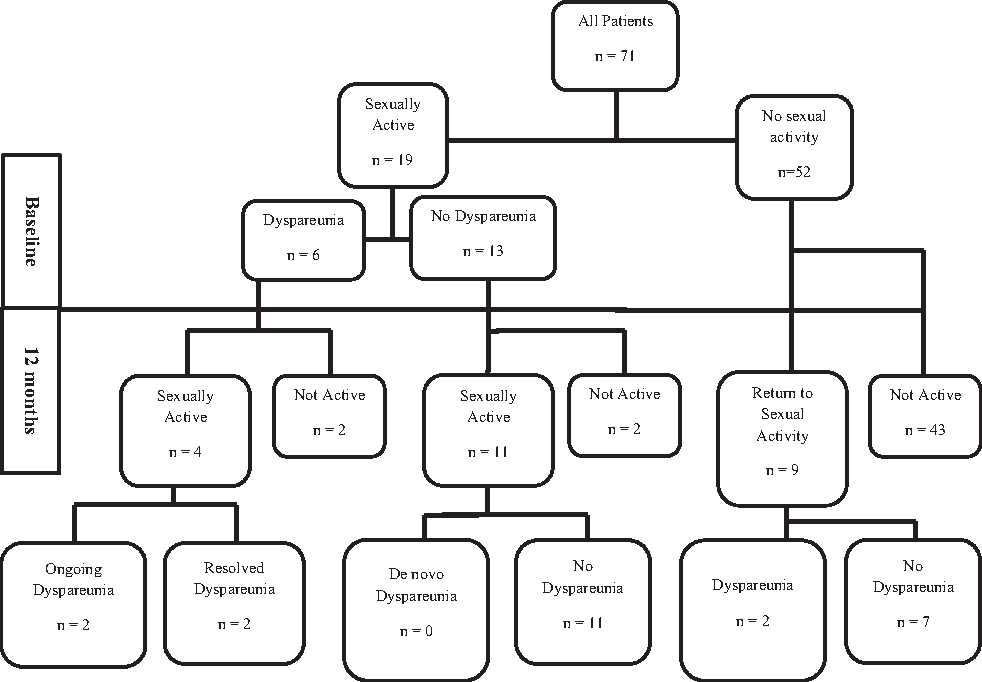
Sexual activity and dyspareunia shown at baseline and at 12 months.
None of the patients had voiding dysfunction nor de novo urinary incontinence.
Recurrent urinary tract infections (UTIs) were noted in 3 (4.2%) patients. All 3 underwent postoperative cystoscopies, which yielded normal results and did not show any evidence of mesh erosion into the bladder. Thus, the postoperative Dindo 14 classifications were 2 patients Class IIIb (intervention under anesthesia for mesh exposure) and 3 patients Class IIIa (office cystoscopy for UTI).
Discussion
Definition of treatment success that includes improvement of vaginal bulge perception and absence of any new untoward side-effects is more meaningful than just anatomical cure. 15 The current study looked at functional improvement, not the anatomical (POP-Q) improvement that has been examined conventionally for prolapse surgical studies.
It has been suggested that mesh can result in scarring and vaginal wall retraction that could result in pelvic pain, especially during intercourse.16,17 There were no cases of clinical mesh retraction in the current study. There was also no statistically significant decrease in TVL from presurgery to the 12-month postoperative visit, as noted on the POP-Q.
There was no deterioration in success from 6 months to 12 months. This was different from the decrease in success from 3 months to 12 months noted by Milani et al. 18 with the Prolift + M system. However, longer-term follow-up is very important to address this issue. There was also no difference in success among the stages of prolapse. This is different from what has been suggested by Lin et al., 19 that native-tissue surgeries for larger stage III or IV prolapses are associated with as much as a 75% risk of recurrence.
Exair hysteropexy findings in this study are very promising, even for large uterine prolapses. Although the 2 failures had very large uterine descensus, there were others in this cohort with similar degrees of prolapse who had good postoperative support.
Moreover, as most of the failures (66%) in the current study were those of the untreated compartment, it is important to scrutinize the contralateral seemingly intact vaginal wall carefully to assess for weaknesses that could become clinically relevant once the ipsilateral wall has been corrected.
The validated questionnaires on urinary, bowel, and prolapse symptoms showed significant improvements (Table 4). All of the questionnaires were self-administered; the majority of the postoperative POP-Q assessments were performed by the principal investigator, introducing some element of bias.
The current study's composite score of 93% was similar to the anatomical success noted by Fatton et al. 20
There were no cases of de novo dyspareunia. Milani et al. 18 also reported a dyspareunia rate of only 2% with the lightweight Prolift + M system. It should, however, be noted that, in the current series, only 23% patients were sexually active preoperatively.
The incidence of mesh exposure in this series of 4.2% was lower than the 8%–15% quoted in the literature.21,22 This could be due to the properties of the lightweight Novasilk mesh. In addition, only 2 of the 3 patients with mesh exposure needed surgical correction.
The strengths of this study were the prospective data collection, the adequate sample size, good compliance with follow-up, restriction to a single mesh kit, use of validated outcome measures, and, finally, the definition of success based upon function rather than anatomical (POP-Q) outcome alone.
The limitations were those inherent to a cohort study and the lack of a control group. Cohort studies are exposed to selection bias. The other limitation is that this particular study group was followed-up to only 12 months and therefore had a short-term follow-up. This was also a single-center experience, where the anatomical success (POP-Q assessment) was determined by the investigator and not by an independent observer.
Conclusions
Although the Exair mesh system is no longer available, this study still provides support for the placement of transvaginal mesh for POP. The current study, along with those of others, 17 showed that, when vaginal mesh surgery is performed for the correct indications by experienced surgeons, complications are mitigated.
This prospective case series provides support that the Exair transvaginal mesh procedure resulted in improvement in both function and anatomy at 1 year in patients with both uterine and posthysterectomy vaginal prolapse. Exair transvaginal mesh surgery was a safe and effective procedure for the management of vaginal wall prolapse, with a low incidence of complications and high satisfaction with this kind of surgery.
Footnotes
Author Disclosure Statement
Funding was provided by Coloplast, Inc., the maker of the Exair mesh system as part of an investigator-initiated study. Dr. Khandwala is also a consultant for Coloplast.