
Abstract
Abstract
Objective:
The aim of this research was to assess the 1-year success of the Dynamic Intraoperative Standing Sling Technique™ (DISST™) for the management of stress urinary incontinence (SUI).
Materials and Methods:
For this prospective cohort analysis, 85 subjects with SUI underwent the DISST. Success of the DISST was assessed in most of these subjects at 1 year.
Results:
Seventy-eight subjects (91.8%) were followed at least 1 year after they had the procedure. Subjective success was 97.4%, and no subject needed retreatment for persistent SUI. The mean operative time was 43.1 ± 9 minutes. There was significant improvement in the Medical Epidemiologic and Social Aspects of Aging URGE subscore as well. Sexual function was also influenced favorably by the DISST, with reductions noted in fear of incontinence, actual incontinence during intercourse, and pain during intercourse. There were no injuries to the bladder or the urethra, and there were no cases of vaginal-sling erosions. There were also no cases of voiding dysfunction, no need for sling release, nor frequent urinary-tract infections.
Conclusions:
The DISST showed good success for the management of SUI. Long-term results are awaited.
Introduction
Tension-free vaginal tape (TVT) and transobturator (TOT) sling procedures have stood the test of time, 1 and several studies have shown them to be effective and similar with respect to success. 2 However, due to the complications of these procedures, the single incision midurethral sling (SIMUS) procedure was devised with the aim of mitigating these complications while maintaining the success of the previous procedures. Several studies showed that SIMUS was inferior to conventional long slings.3–6
A systematic review in 2011 of all mini-sling randomized clinical trials (RCTs) showed inferior objective cure rates, compared with those of the conventional midurethral sling (MUS). 7 In fact, an updated systematic review of mini-sling RCTs showed that, despite the exclusion of TVT–Secur,® SIMUS still had a trend, albeit insignificant, toward higher rates of repeat continence surgery. 8 Even the U.S. Food and Drug Administration's revised statement of January 2016 noted that SIMUS still needed further evaluation; only the long slings were not controversial. 9
The premise of the Dynamic Intraoperative Standing Sling Technique™ (DISST™) involves an office analysis of a comparison between the supine and upright cough tests in patients with empty bladders during the patients' initial evaluations for stress urinary incontinence (SUI) complaints. In 48% or nearly half of these patients, the standing cough test was positive for leakage although the supine cough test was negative. Thus, a negative cough test result in the supine position may be falsely negative. Patients who complain of SUI do so mainly in the standing position. In addition, for most studies, objective success of a sling procedure is determined by a negative standing cough test at bladder fullness.
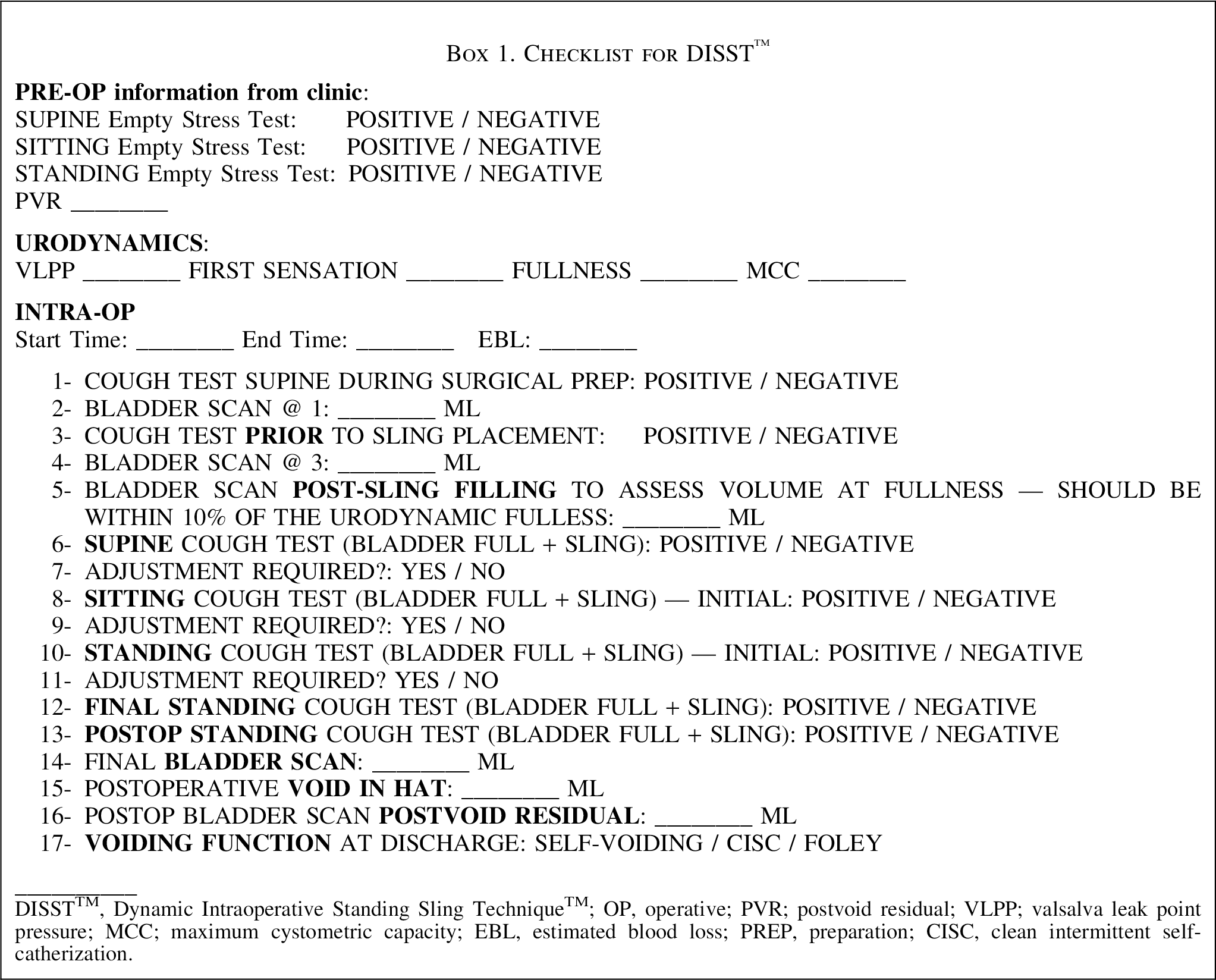
The current author has been performing SIMUS under local anesthesia for the past 6 years with good patient acceptance. 10 Given that the patients are awake during the SIMUS, it was decided to perform an intraoperative standing cough test at subjective bladder fullness per the DISST protocol (see Box 1). DISST success is defined as a negative intraoperative standing cough test in a patient with a full bladder. Bladder fullness is defined as the patient's subjective fullness that has to be within 10% of fullness on urodynamic testing (strong desire) or per voiding diaries (typical voided volume).
The aim of this study was to assess the 1-year outcome of subjects with SUI who underwent the DISST.
Materials and Methods
This was a prospective cohort study of 85 patients who underwent a MiniArc SIMUS procedure including DISST from August 2013 to September 2015.
This clinical trial was approved by the institutional review board at the Wayne State School of Medicine, in Dearborn, MI. Informed consent was obtained and documented from all 85 patients. This study was not funded by the manufacturer of the MiniArc sling, American Medical Systems/Astora, or any other source.
Participants
Inclusion criteria included women who: had SUI or SUI-dominant mixed incontinence in urodynamic studies; had hypermobility of the urethrovesical junction, defined as a Q-tip straining angle ≥30°; desired surgical correction of incontinence; had behavioral therapy that failed; and had a negative intraoperative cough test at bladder fullness in the standing position (i.e., they were DISST success).
Patients were excluded if they: had not completed childbearing; needed concomitant surgery; or were considered to be poor candidates for the DISST (e.g., had a narrow genital hiatus, were unable to have the procedure conducted under local anesthesia due to severe anxiety, were unable to stand during the procedure due to morbid obesity, or had mobility restrictions or anesthesia issues). Prior anti-incontinence surgery was not an exclusion for this study.
The DISST
A special height-adjustable patient standing platform and a movable harness bar were devised by the current author so a patient could hold onto the bar in front of her when standing fully erect. The height-adjustable platform enabled the patient's pelvis to be brought up to the eye level of the sitting surgeon, who could then visualize the urethra clearly during the standing cough test without risk of contamination. Sterility of the field was still maintained with the patient in the standing position (see Fig. 1). The surgical procedure was performed with the patient completely awake and responsive.

Special height-adjustable patient standing platform and a movable harness bar that the patient can hold onto in front of her when she is standing fully erect.
It is important to confirm a positive cough test prior to sling placement. The sling arm on one side is placed, and, on the other side, the needle is left attached to the self-fixating tip of the sling for further tightening, if required. After the sling is placed under the mid-urethra, cystourethroscopy is performed to not only confirm bladder/urethral integrity but also to fill the bladder up to the patient's subjective fullness corresponding to the urodynamic volume result. This is confirmed by a bladder scanner that is frequently used intraoperatively. The patient is then asked to cough three times in the lithotomy position (see Fig. 2). If there is no leakage, the same cough test is repeated with the patient in the sitting position and then in the standing position (see Figs. 3 and 4). The harness bar is lowered so that it is at the patient's abdomen level and she is holding onto it comfortably when she is standing on the platform. The bar also gives the patient leverage to stand erect.

Cough test performed lying down. The patient is asked to cough three times in a supine position once subjective bladder fullness is confirmed with a bladder scan.

Cough test performed in the sitting position. The back of the operating room table is raised so that the patient is in a sitting position when she is asked to cough three times to confirm that no leakage occurs.

Cough test performed with patient in a standing position. The patient is asked to stand and cough three times to confirm that no leakage occurs.
If, at any point in time, the patient's bladder leaks, then the sling is tightened further until the leaking stops. If a significant leakage has occurred then the bladder might have to be rescanned to ensure that it did not empty substantially; if this is the situation, the bladder is refilled. If the patient's bladder leaks when she is in the standing position, it is imperative to return her to the horizontal position prior to tightening the sling. This should never be done with the patient in the standing position as the pelvic configuration is different and the angle of needle penetration would be completely different. In addition, if the patient experiences pain, she might move or fall back onto the table; this occurrence could lead to injury.
Once the standing cough test with individual bladder fullness is successful, then the patient is asked to sit down slowly on the operating room (OR) table while the surgeon is cradling the needle inserter carefully. The back of the table is flattened, and the patient's legs are put back in the lithotomy position. The inserter is then removed under direct vision to ensure that the sling does not loosen. Finally, the vaginal incision is closed.
The patient is made to stand up for the final cough test prior to walking her to the stretcher beside the OR table. This confirms that the sling did not loosen during the removal of the inserter and “what-you-see-is-what-you-get.” A patient with a negative final cough test at individual fullness is considered to have DISST success.
Study design
At baseline, all participants underwent a standardized evaluation, which included a detailed urogynecologic history, a pelvic examination, pertinent validated questionnaires, and urodynamic testing. Follow-up visits were scheduled for 2 weeks, 6 weeks, 3 months, 6 months, 12 months, and yearly thereafter for 3 years.
The primary outcome of this study was the subjective success of SUI correction in subjects who had undergone DISST at least 12 months prior. This was based on: “From the point of view of stress urinary incontinence (that is leaking if you sneeze, cough, laugh, or do any strenuous activities), are you satisfied with the outcome of the surgery?” Answered “Yes” or “No,” AND, “On a scale of 0–10: If 0 is really bad and you are leaking like you were before the surgery and 10 is no leak at all, how would you rate your urinary symptoms today?” AND no retreatment for SUI.
The secondary outcome was objective success determined by a negative provocative standing stress test at fullness based upon the patient's urodynamic fullness; the test is performed by an independent observer. The other factors assessed were de novo urgency incontinence, based upon the Medical Epidemiologic and Social Aspects of Aging (MESA) 11 questionnaire, and voiding dysfunction. Sexual function was assessed by the Prolapse/Urinary Incontinence Sexual Questionnaire–Short Form-12 (PISQ-12). 12 In addition, surgical time, intraoperative blood loss, hematomas, injuries, and mesh exposures/erosions were assessed.
Statistics
The SAS System for Windows version 9.3 (Cary, NC) was used for the majority of the statistical analyses. Cytel Studio 11 was used for the marginal homogeneity tests for the individual PISQ-12 questions (Cytel, Inc., Cambridge, MA).
Results
Eighty-five women were enrolled in the study from August 2013 to September 2015 and met the criteria for the DISST study. Baseline demographics of all 85 patients and surgical information are listed in Table 1. Seventy-eight patients (91.7%) were available for the primary outcome analysis.
Demographics and Surgical Information (n = 85)
Mean ± standard deviation (range).
†Number of subjects (%).
BMI, body mass index; UDT; urodynamic testing; ASA, American Society of Anesthesiologists; min, minutes; EBL, estimated blood loss.
The success of DISST to correct SUI was 97.4%. The satisfaction score was 9.04 of 10. No subject required retreatment for SUI. Sixty-three of 64 (98.4%) patients had negative standing cough tests at fullness. The 1 subject who had a positive cough test at fullness stated that she was improved but not cured and that she did not want to undergo any further intervention. The mean operative time was 43.1 ± 9 minutes.
There was strong evidence of a difference in mean MESA total scores, stress scores, and urge scores among the 3 time periods: presurgery, and 6 and 12 months postoperatively (p < 0.0001). Tukey multiple-comparison procedures indicated that the mean scores were lower at 6 and 12 months than they were presurgery; with the same mean score at 6 months and 12 months. This indicates that the improvement that was noted at 6 months was sustained at the 12-month postoperative visit (Table 2).
Comparison of Mean MESA Scores Using Tukey–Kramer Adjustments
MESA, Medical Epidemiologic and Social Aspects of Aging questionnaire; SE, standard error; CI, confidence interval.
From the perspective of sexual function, answers to the three key questions (questions 5, 6, and 7) of the PISQ-12 that pertained to the sling procedures were compared. These questions concerned: (5) pain during intercourse; (6) incontinence during intercourse; and (7) fear of incontinence during intercourse. There was no statistically significant difference (p = 0.58) in pain with intercourse between preoperative assessment and 12 months after surgery in patients who were sexually active at both times. There was statistically a significant difference (p < 0.0001) in urinary incontinence with sexual activity between the preoperative assessment and the assessment 12 months after surgery in patients who were sexually active at both times, with the direction of the effect indicating improvement in the reporting of this symptom. No patient indicated a higher frequency of fear of incontinence restricting sexual activity at 12 months than preoperatively. There was a statistically significant difference (p < 0.0001) in frequency of the fear of incontinence restricting sexual activity response between preoperative assessment and 12 months after surgery in patients who were sexually active at both times, with the direction of the effect indicating improvement in the reporting of this symptom (see Table 3). These results indicated a positive overall impact of the DISST MiniArc sling procedure on sexual function.
Comparison of PISQ-12 Preoperative & Postoperative at 12 Months
PISQ-12, Prolapse/Urinary Incontinence Sexual Questionnaire–Short Form-12; op, operative.
There was no voiding dysfunction in this group. All but 1 patient went home spontaneously voiding. The remaining subject was taught self-catheterization that she discontinued 4 days postoperatively. No sling had to be loosened or revised due to voiding dysfunction. Although this study did not set out to assess postoperative pain, no subject needed any prescription pain medications in the immediate or delayed postoperative periods. There were no injuries to the bladder, urethra, or vaginal epithelium in any patient. There were no cases of mesh erosions into the urethra. There were no cases of mesh exposures in the vagina. There were no cases of recurrent urinary-tract infections. This is probably aided by the fact that an intraoperative catheter was not used.
Discussion
The key factors that predict patient satisfaction after an incontinence procedure include pain, voiding function, and de novo urgency. 13 There were no cases of voiding dysfunction or de novo urgency incontinence. In fact, several subjects with overactive bladder symptoms noted reductions in their symptoms. This is similar to a multivariate analysis that was performed to determine risks for the development of persistent urgency after MUS, wherein a TOT sling was identified as an independent favorable factor. 14
The success of DISST (97.4%) and the degree of satisfaction (9.04 of 10) were very satisfactory in this study.
The surgical time (43.1 ± 9 minutes) noted in this study was much longer than some other MiniArc sling procedures that were performed under general/spinal anesthesia (10 minutes),14,15 as the DISST technique is very elaborate, and all criteria (Box 1) need to be fulfilled for the procedure to be considered a DISST success. The surgical time noted in this study was from “time out” to the completion of the postoperative standing cough test.
The literature on SIMUS mainly indicates poor outcomes. Although this was thought to be mainly due to a specific SIMUS—the TVT–Secur—poor results have also been seen with the other slings, such as the MiniArc or the Ajust. Tensioning under the urethra with SIMUS has always been challenging. The single-incision sling differs from its long-sling predecessors in that the intrinsic tensioning that occurs in the TOT/TVT sling during the upward pull of the plastic sheath is never seen with the SIMUS. In fact, the backward release of the SIMUS needle passers means that the sling will loosen, if anything. Therefore, when it comes to the SIMUS procedure, most surgeons have given up the term tension-free placement and are favoring terms, such as pillowing of the suburethral tissue, wherein the sling is snug under the urethra so that the fascial tissue bulges through the pores of the sling mesh. 10
DISST is an attempt to remove the tensioning variability out of the procedure.
Every individual patient presents a unique scenario in terms of body mass index, cough intensity, pelvic forces exerted, urethrovesical junction mobility, and intrinsic urethral and pelvic floor architecture. Hence the tension required of the suburethral sling would depend upon these factors, thus, precluding a “one-size-fits-all concept.” A DISST success means that the sling is now positioned appropriately under the urethra for that particular patient.
This study was conducted using the MiniArc SIMUS, which has no longer been available as of April 2016. However, the principles stated in the DISST should apply to any SIMUS procedure, and the current author has continued to use DISST with the Solyx SIMUS and is noticing similar results.
This study reported only a 1-year outcome. Although the results were promising, it is too early to say if these results will sustain the test of time. Basu and Duckett 16 showed that women who underwent MiniArc SIMUS and who were continent at 6 months were nearly as likely to remain continent up to 3 years. They concluded that single-incision slings fail early in the postoperative time period and that the major difference in efficacy occurs at an earlier point, which supports the theory that initial fixation might be of importance.
The strength of this study was the high 12-month follow-up rate (91.7%). The limitations of this study were the short duration of follow-up, the lack of a control group, and a single-center experience.
Conclusions
This prospective study of 85 patients who underwent the DISST MiniArc sling procedure and were followed for at least 1 year had very good efficacy with minimal side-effects or complications. However, longer-term results are critical. The current author shall continue to follow these patients over the longer-term and looks forward to presenting that data.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.