
Abstract
Abstract
Objective:
The goal of this research was to assess diagnosis and laparoscopic management of deep-infiltrating endometriosis after formation of a specialized unit in the Clínica Santa María, Santiago, Chile. Outcomes were compared with the current authors' results prior to the new unit.
Materials and Methods:
This retrospective study used prospectively collected data of 137 patients with pathology-proven deep-infiltrating endometriosis. The patients were divided into 2 groups: A had patients operated on prior to the unit's formation (n = 39) and B had patients operated on after the unit's formation (n = 98). Surgical and fertility outcomes were compared.
Results:
All procedures were performed laparoscopically without conversions. A significant increase in use of preoperative imaging (p < 0.001) and revised American Fertility Society staging (p = 0.01) occurred after the unit's formation. Bowel involvement was significantly higher in Group B (12.8% versus 38.8%; p < 0.004). There were also fewer incomplete resections (28.2% versus 2%; p < 0.001), lower recurrence rates (20.5% versus 6.1%; p = 0.02), and fewer reoperations (10.3% versus 1%; p < 0.02) since the unit's formation. Complication rates were similar in both groups. One-year pregnancy rates were similar, but time-to-pregnancy was shorter in Group B (12 versus 6.2 months; p = 0.02). Median follow-up was 49.3 versus 14.4 months for Groups A and B, respectively (p < 0.001). In Group A, 79% of the patients experienced relevant symptom reductions versus 94% in Group B (p = 0.02).
Conclusions:
Surgical management of deep-infiltrating endometriosis in specialized units improves perioperative outcomes significantly.
Introduction
L
Materials and Methods
Medical records of all patients operated for deep-infiltrating endometriosis in the Clinica Santa Maria from January 2010 to December 2017 were reviewed retrospectively. Only cases with pathology-proven deep-infiltrating endometriosis were included. The specialized endometriosis unit was created in 2014; since then, all patients with suspected or diagnosed deep-infiltrating endometriosis were evaluated at that unit and collection of prospective data began. All women operated on prior to 2014 were included in 1 group (A). All patients operated in at the new unit were included another group (B). Before the unit had been created, both preoperative work-ups and surgical techniques varied according to individual surgeon'a discretion. Since 2014, all patients underwent structured preoperative workups, including preoperative imaging and estimation of ovarian reserves (Fig. 1).

Clinical approach to the new endometriosis unit. Logo used with permission.
All procedures were performed by laparoscopy, following a standardized technique. 3 After adhesiolysis, deep-infiltrating endometriosis nodules were dissected, isolated and, removed. Dissection was carried out until the loose areolar tissue of the retroperitoneal space was reached. Ureterolysis and dissection of pararectal spaces were carried out, if necessary. Ureters were always identified before the dissection of deep-infiltrating endometriosis involving the uterosacral ligaments. Deep-infiltrating endometriosis infiltrating the vagina required partial colpectomy combined with rectovaginal septum dissection. In patients with bowel endometriosis, any woman with 1 isolated rectosigmoid deep-infiltrating endometriosis lesion, ≤30 mm in diameter and affecting <40% of the intestinal circumference underwent conservative surgery (either rectal shaving or discoid excision). Women with multiple intestinal deep-infiltrating endometriosis lesions, >30 mm in diameter, affecting >40% of bowel circumference or bowel stenosis, underwent segmental bowel resection and anastomosis. 4 In cases of ultra-low rectal anastomoses (< 6 cm from the anal verge), a protective ileostomy was performed. All cases were staged according to the revised American Fertility Society (rAFS) classification of endometriosis. 5
Institutional review board approval was obtained from the institutional ethics committee, and informed consent was obtained from each patient. Data collected included each patient's age, parity, symptoms, previous surgeries for endometriosis, operative time, conversion to laparotomy (if this occurred), deep-infiltrating endometriosis location(s), completeness of deep-infiltrating endometriosis removal, complications, time of follow-up, pregnancies, symptom recurrence(s) and satisfaction with surgery. Complications were designated according to the Clavien–Dindo classification. 6
Each postoperative follow-up was performed at the surgeon's office and by telephone, asking the patient which of the following best described the effect of surgery on the pain she experienced: no more pain; significant reduction; slight reduction; or no reduction—this has been described previously. 7 Recurrences were defined as pain recurrence, pain persistence, slight reduction, or no reduction of at least 1 pain symptom, and/or the need for a new operation. Surgical completeness was evaluated by reviewing the surgical videos and analyzing pathologic results.
Data were analyzed using descriptive statistics. Categorical variables were summarized using frequency (percentage), and Fisher's exact test was used to compare differences between the 2 groups. The Shapiro–Wilk test was used to test the presence of normal distribution in quantitative variables. Non–normally distributed variables were expressed as median (range), and a Mann–Whitney-U test was used for comparison between the 2 groups. Normally distributed variables were expressed as mean (± standard deviation), and a t-test was used for comparison between the 2 groups. Statistical analysis was performed with SPSS statistical software 20.0 version (IBM Corp., Armonk, NY). Statistical significance was established at p < 0.05.
Results
During the study, 137 consecutive patients with pathology-proven deep-infiltrating endometriosis were operated on at the Clinica Santa Maria. All surgeries were completed by laparoscopy without any conversions. Demographic data for both groups are summarized in Table 1. There were no differences between groups; however, dyschezia was more frequent in Group B (p = 0.004). Preoperative workups are shown in Table 2. There was a significant increase in the use of magnetic resonance imaging (MRI) and extended transvaginal ultrasonography (TVUS) since 2014. Anatomical locations of the patients' deep-infiltrating endometriosis are listed in Table 3. Bowel involvement was more frequent in Group B (p < 0.001).
Demographic Data of 137 Patients with Deep-Infiltrating Endometriosis
Values given as mean ± standard deviation.
Values given as median (range).
Bold value indicates significant correlation.
Preoperative Work-Ups
Bold values indicate significant correlations.
Anatomical locations of Deep-Infiltrating Endometriosis a
Most patients had several locations.
Bold value indicates significant correlation.
Operative data and surgical procedures are shown in Table 4. Median operative time was similar in both groups; however, it was longer in cases requiring bowel surgery (127 [55–279] versus 177 [124–300] minutes; p < 0.0001 in Group A and 123 [50–357] versus 190 [68–463] minutes; p < 0.0001 in Group B). There was also a significantly higher number of patients with advanced disease (rAFS stages III–IV) in Group B (p = 0.013). Furthermore, the median size of the endometriotic nodules was bigger in Group B (17 versus 22 mm; p = 0.02). Moreover, a significant increase of patients undergoing resective bowel surgery (disc excision or segmental resection) was noted in Group B; this also occurred in patients undergoing hysterectomy and salpingectomy. Surgical completeness was significantly higher after the creation of the unit, leading to a significant decrease in both recurrence rate (20.5% in Group A versus 6.1% in Group B; p = 0.024) and necessity for reoperation (10.3% in Group A versus 1% in Group B; p = 0.023) during that time period.
Operative Data & Surgical Procedures a
Several patients underwent multiple surgical procedures.
Values given as median (range).
Bold values indicate significant correlations.
rAFS, revised American Fertility Society.
Complication rates were similar in both groups (Table 5).
Complications by Clavien–Dindo Grade
In Group A, 4 patients (10.2%) had grade III complications. Two patients presented with ureteral fistulae: 1 patient managed with extensive ureterolysis had an ureterovaginal fistula on postoperative day 12 and 1 patient presented with uroperitoneum on postoperative day 4. Each patient was managed conservatively by drainage of the uroperitoneum, and placement of a urinary catheter and double-J stent for 6 weeks. Another patient who underwent hysterectomy presented with vaginal bleeding on postoperative day 4 due to partial vault dehiscence. She underwent vaginal suture and antibiotics. Another woman presented with an abdominal-wall hematoma due to an accidental puncture of her epigastric vessels during ovarian suspension. Her condition was managed intraoperatively with a compression suture.
In Group B, grade III complications were seen in 7 patients (7.1%). Two patients who underwent segmental bowel resection, in whom the bowel was exteriorized through enlarged umbilical ports, presented with umbilical hernias. Two patients had ureteral lesions. One patient, who required unilateral parametrectomy, presented with a ureterovaginal fistula on postoperative day 12; this was managed by laparoscopic ureteral reimplantation. The other case was a patient who underwent extensive ureterolysis and prophylactic double-J stent placement and presented with a ureteral fistula on postoperative day 9 with the catheter still in place. She also underwent laparoscopic ureteral reimplantation. Two patients had bowel lesions. One patient managed with bowel endometriosis had a rectal perforation during shaving; this perforation was repaired with a primary suture. The other patient had a delayed diagnosis and presented with acute peritonitis on postoperative day 3 requiring laparotomy and colostomy. One patient had a bladder injury that was repaired during the surgery.
Median follow-up was 49.7 (range: 1–99) and 14.4 (range: 1–46) months for Groups A and B, respectively (p < 0.001). In Group A, 79.5% experienced improvement that was considered relevant (no more pain or significant reduction of pain), compared with 94% in Group B (p = 0.002).
Fertility outcomes and type of pregnancies among patients who wished to become pregnant are summarized in Table 6.
Fertility Outcomes Among 74 Patients Who Wished to achieve Pregnancy
Values given as median (range).
Bold values indicate significant correlations.
Discussion
Endometriosis is a complex disease affecting many aspects of patients' quality of life 8 ; however, adequate and evidence-based surgical treatment remains the limiting factor in obtaining favorable long-term outcomes.9,10 The problem with the performance of advanced laparoscopic procedures, such as deep-infiltrating endometriosis resection in developing countries, is that hospitals provide limited or no training in laparoscopic surgery. Surgeons often teach themselves and embark on the practice of minimally invasive surgery with limited or absent formal training. The latter determines the number of partial resections, disease persistence, or recurrences, leading to a high reoperation rate among patients with endometriosis.10,11 In the current authors' experience, 23% of the treated patients had had at least 1 previous surgery for endometriosis. For that reason, current concepts in the management of endometriosis agree that the disease must be approached in specialized units that are mainly focused on optimal surgical therapy.1,9
To the current authors' knowledge, this was the first study to compare surgical outcomes before and after the creation of a specialized endometriosis unit in a developing country, and the study results supported the aforementioned concepts. In the current study, although demographics were similar between the 2 groups, dyschezia was more frequent in Group B. Perhaps, this only reflects the fact that, after the unit formation, patients with suspected endometriosis underwent more-directed evaluations, including history-taking focused on the presence of deep disease, such as the presence of dyschezia. 12 Preoperative imaging is a critical component in the work-up of deep-infiltrating endometriosis. Preoperative knowledge of a deep-infiltrating endometriosis location can enable the surgeon to optimize the surgical plan, including budgeting sufficient operative time, ensuring availability of instruments, counseling a patient adequately about risk, and coordinating the assistance of other surgeons, thereby enhancing the patient's safety and reducing the risk of reoperation. 13 Unfortunately, despite many different and effective options available to detect and characterize deep-infiltrating endometriosis preoperatively, in Chile, the condition is still frequently a surprise finding on laparoscopy.
There was a significant increase in the use of adequate preoperative imaging after the creation of the unit. Although it has been stated that TVUS is the first-line imaging modality for deep-infiltrating endometriosis assessment, 14 the current authors prefer MRI because is less operator-dependent and can be used to assess more of the pelvis. In that sense, the raise in number of patients having bowel involvement after 2014 only reflects better diagnostic technology. Therefore, with better surgical planning, the current authors were able to perform operations on patients with more-complex cases while increasing the completeness of the surgeries. This demonstrated that surgical management of deep-infiltrating endometriosis was performed better after the creation of the unit, probably due to the availability of a multidisciplinary team, including a gynecologist, an urologist, and a colorectal surgeon.
Interestingly, complication rates were similar in both groups, despite the performance of more advanced procedures in Group B, such as bowel surgeries. However, some specific complications noted were due to exteriorization of the bowel in each of the patients with an umbilical port to prepare the anastomosis (Fig. 2). Since then, in such a case, the authors exteriorize the bowel through a mini-Pfannenstiel incision or through the vagina (if the vagina needs to be open due to the patient's endometriosis), therefore, avoiding umbilical-port enlargement (Fig. 3).
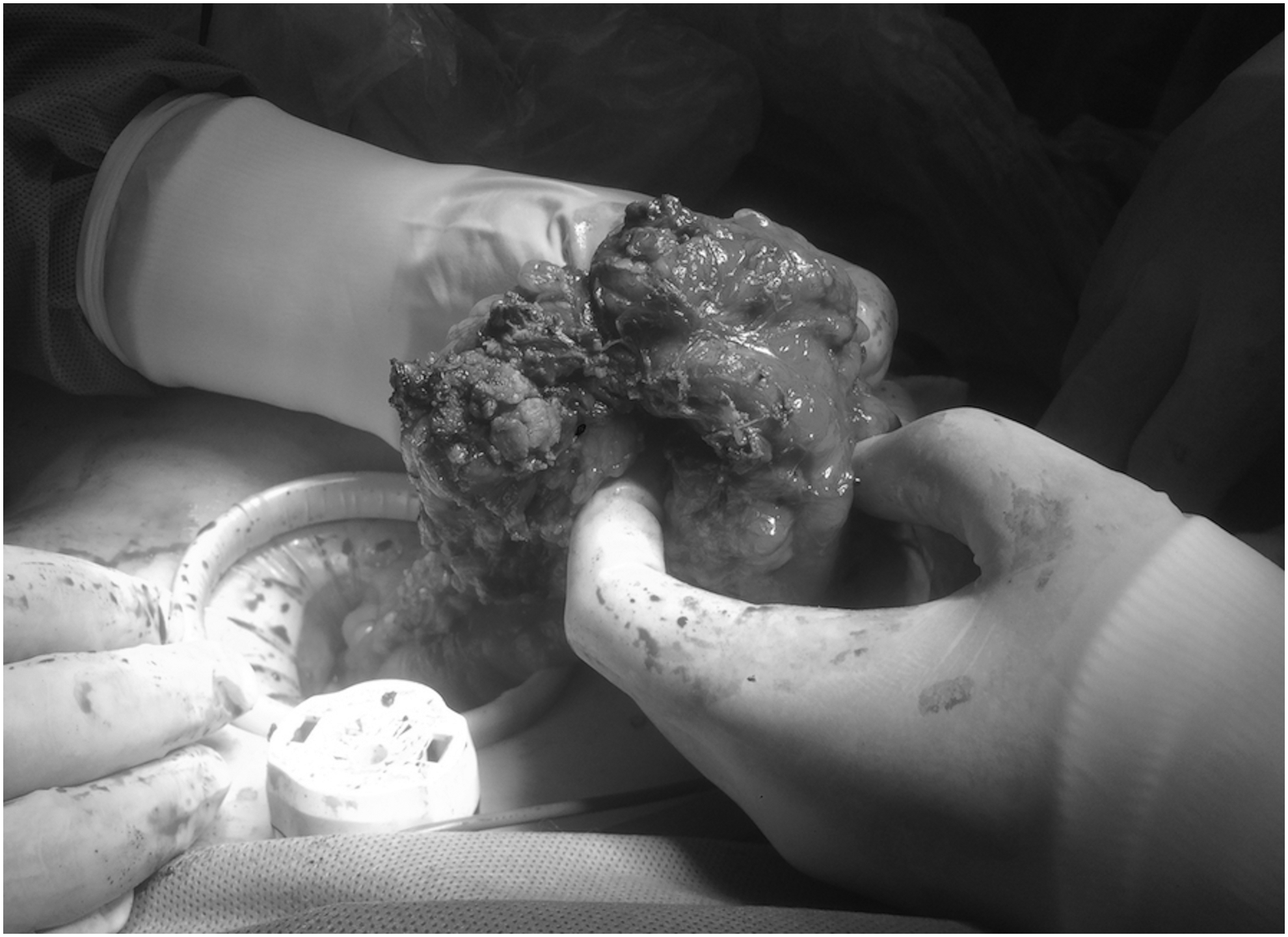
Transumbilical bowel exteriorization prior to segmental resection. Note the enlarged umbilical port.

Vaginal exteriorization of deep-infiltrating endometriosis with both bowel and vaginal involvement. Note the affected vagina and mucosa are attached to the anterior rectal wall (arrow).
Management of ovarian endometriomas deserves special mention. First, this is usually the first finding in a patient with suspected endometriosis, given that endometromas are diagnosed easily with TVUS. Second, an endometrioma is a reliable marker of disease severity, showing a good correlation with the presence of deep-infiltrating endometriosis. 15 Third, optimal management of these lesions is the cornerstone of fertility prognosis due to their potential deleterious impact on ovarian reserves, especially in women who have been operated on previously. 16 Since 2014, all patients with deep-infiltrating endometriosis and concomitant endometriomas wishing pregnancy underwent preoperative ovarian-reserve assessment to tailor operative management. Despite higher recurrence rates after ablation, compared to cystectomy, 17 in patients with low ovarian reserves desiring pregnancy, the current authors only perform drainage and ablation despite endometrioma size. Interestingly, this approach has not caused symptomatic recurrences requiring surgery.
Recurrence remains a major concern after surgical management of deep-infiltrating endometriosis. A recent systematic review of the literature reported 2%–43% recurrence rates after deep-infiltrating endometriosis excision, depending on the definition of recurrence and the length of follow-up. 18 In the current series, the recurrence rate was comparable with those of expert centers worldwide. 18 Furthermore, the rate was significantly lower after the unit formation, which was probably related to a higher percentage of complete surgeries. However, it is important to consider that the length of follow-up was also significantly shorter in that group (B). Considering that there has been a tendency of increased recurrence rates in studies with longer follow-ups, 18 this was a raise that could have been expected.
Several studies have reported that recurrence of deep-infiltrating endometriosis observed in a second operation often occurred in the same area of the pelvis that was involved in the first operation, 11 suggesting that incomplete surgical excision is an important risk factor for recurrence. However, the pathogenesis of the recurrence of endometriosis-associated symptoms could be different. 19 In the current study, although most of the patients had significant improvement after surgery, at least 30% of patients experienced some degree of pain after complete deep-infiltrating endometriosis excision, supporting the theory that recurrence of pain does not necessarily mean that a lesion has recurred at that site. 19 Furthermore, in agreement with previous studies, 20 recurrent deep-infiltrating endometriosis lesions did not show on imaging in most of the patients who were operated on, despite their persistent pain. The latter could be explained by the coexistence of different mechanisms involved in pelvic pain, such as myofascial pain or central sensitization. 21 Another explanation could be the concomitant presence of adenomyosis. 22 For that reason, since 2014, the current authors have been more flexible when considering indications for hysterectomy, which was reflected with the significant raise in hysterectomy rate in Group B.
The role of deep-infiltrating endometriosis excision in pregnancy rates is matter of debate, especially in asymptomatic patients. 21 A higher pregnancy rate was noted in Group A, which was probably due to the longer follow-up in that group and the fact that, after 2014, infertility alone was no longer a surgical indication. Based on observational studies that have suggested better pregnancy rates after surgery in patients with deep-infiltrating endometriosis, 23 the current authors recommend surgery to optimize fertility in young women with infertility if they have severe pain and/or large endometriomas and good ovarian reserves. Otherwise, in cases of older patients, low ovarian reserves, male factors, or any combination of these factors, the current authors consider immediate in-vitro fertilization (IVF) rather than surgery.
An increase in the use of IVF in Group B was noted, which was probably due to a more-systematic approach to the infertile patients with deep-infiltrating endometriosis. Moreover, it is noteworthy that, although the 1-year pregnancy rate was similar in both groups, patients in Group B achieved pregnancy significantly faster. The current authors suggest that this is a direct consequence of the growing use of IVF, because it not only raises the chances of pregnancy in patients with deep-infiltrating endometriosis, compared with more-conservative approaches, 24 but also could decrease emotional distress and minimize dropouts from infertility treatments.
The current study had some limitations: First, although data were prospectively collected since 2014, this research was still retrospective in nature. Second, the length of follow-up was significantly different between the 2 groups; therefore it was difficult to draw definitive conclusions about long-term outcomes. Third, the use of a verbal rating scale to assess pain reduction made it difficult to compare results because there of the wide variability of terms used to describe each pain category in the literature. 25
However, one of the strengths of the study was that it was able to show that the ability to perform a complete operation by a specialized team has significant influence on the outcome. This was accomplished by comparing the surgical results with those that the current authors had had previously.
Conclusions
This study demonstrated a significant improvement in diagnosis and quality of surgical management of deep-infiltrating endometriosis after the creation of a specialized unit in a developing country.
Footnotes
Acknowledgments
The current authors thank Andrea Canals for her valuable assistance in the statistical analysis.
Author Disclosure Statement
No financial conflicts of interest exist.