
Abstract
Abstract
Objective:
Many familial and sporadic endometrial carcinomas have microsatellite instability (MSI) due to mutations in the DNA mismatch repair (MMR) genes. Immunohistochemistry (IHC) for MMR proteins is used to detect MSI in endometrial carcinomas (ECs) and to screen patients for Lynch syndrome (LS). The present study was conducted to evaluate MMR protein expression by using IHC in ECs and to determine the association of MSI-related EC with various clinicopathologic parameters.
Materials and Methods:
This was a retrospective study of 83 cases of primary EC. IHC was performed using tissue microarrays for MMR proteins. Loss of expression of these proteins was correlated with various clinicopathologic features.
Results:
Loss of expression of at least one of the MMR proteins was seen in 62.7% cases. Loss of PMS2 (54.2%) expression was most frequent, followed by MLH1 (49.4%) and MSH2 (31.3%). Of the patients age <50 (n = 25), 76% had loss of MMR expression. Loss of MSH6 expression alone as well as in combination with MSH2, was significantly more frequent among these younger patients, compared to older ones (p = 0.03). Loss of expression was significantly (p < 0.001) more frequent (78.8%) in low-grade endometrioid carcinomas.
Conclusions:
The present study showed loss of MMR expression in 62.7% ECs. Lower tumor grade was the most significant predictor of MMR loss. A proportion of these cases might be associated with LS. Screening these patients for MMR deficiency and subsequent confirmation by mutation testing is essential for early identification of such cases.
Introduction
Endometrial carcinoma (EC) is one of the most-common tumors in the genitourinary tracts of females, with an overall incidence of 12.9/100000 women in developed countries and 5.9/100000 in developing countries.1,2 Conventionally, ECs are divided into type 1 and type 2 carcinomas. Type 1 or endometrioid carcinomas are low-grade tumors associated with estrogen excess, favorable outcomes, and mutations in the PTEN, β-catenin, KRAS, or PIK3CA genes. Type 2 or serous carcinomas are high-grade aggressive tumors with poor clinical outcomes and mutations in the TP53, PIK3CA, or PPP2R1A genes.
Tumors associated with hereditary, nonpolyposis colorectal cancer or Lynch syndrome (LS) are commonly associated with genetic instability of microsatellite repeat sequences, also known as microsatellite instability (MSI). This occurs as a result of germline mutations in any of the DNA mismatch repair (MMR) genes, most commonly being the MLH1, MSH2, MSH6, and PMS2 genes. The hallmark cancers for LS include colorectal adenocarcinoma and EC, with the latter being more common in females.3–5
About 2% of females with newly detected EC have LS. 6 Females with LS have an ∼40%–60% lifetime risk of developing EC and an ∼50%–85% lifetime risk of developing colorectal cancer. 7 The lifetime risk of LS-associated EC is also related to age and specific MMR gene mutations. The frequencies of different MMR gene mutations are: ∼50%–66% in MSH2; ∼ 20%–40% in MLH1; ∼ 10%–13% in MSH6; and ∼ < 5% in PMS2. 8 Women with MSH6 mutations and younger age are at a higher risk (64%–71%) of developing EC followed by women with MSH2 and MLH1 mutations.9,10 Clinically, a low body mass index (BMI), young age at onset, and a family history of LS or LS-associated tumors should raise a suspicion of LS-associated EC. 11 Pathologically, LS-associated EC includes both endometrioid and nonendometrioid histologic types of tumors. Certain distinct microscopic features have been, reportedly, seen in LS-associated ECs.8,12
In an ideal scenario, endometrial and colorectal cancers should be screened routinely for a mismatch repair defect; however, definite screening guidelines are not available for ECs. The present study was performed to evaluate MMR protein expression using immunohistochemistry (IHC) in ECs and to determine whether or not certain clinical parameters and morphologic patterns correlated with MSI-associated ECs.
Materials and Methods
This was a retrospective study carried out over a period of 10 years (2006–2016) in the Department of Cytology and Gynecological Pathology, of the Postgraduate Institute of Medical Education and Research, in Chandigarh, India. The departmental archives were searched for cases that were reported histopathologically as type 1 ECs based on hysterectomy specimens, per the World Health Organisation 2014 classification of uterine tumors. 1 Information on all of these cases was retrieved and all of the relevant clinical details, including personal and family histories, were recorded. Cases of patients who had received any form of treatment, such as radiotherapy or neoadjuvant chemotherapy, prior to resection of their tumors were excluded from the present study. All of the stained slides were reviewed independently by 2 experienced gynecologic pathologists, and different histopathologic parameters were recorded (Table 1).
Histopathologic Features Evaluated in the Present Study
hpf, high-power fields; LUS, lower uterine segment; MELF, microcystic, elongated & fragmented.
Tissue microarrays (TMAs) were prepared for evaluating mismatch repair protein expression with two cores from each case. Hematoxylin and eosin–stained slides of the selected cases were screened and representative paraffin blocks were retrieved. Subsequent mapping of slides was done by marking each area of interest with a marker on a scanning view. The corresponding area on the paraffin block was marked with a white ink. The marked tissue was extracted using automated Quickray™ and embedded in a recipient block.
Subsequently, IHC for mismatch proteins—MLH1 (G-168-728, Cell Marque, 1:40 dilution), MSH2 (G-219-1129, Cell Marque, 1:80 dilution), MSH6 (44, Cell Marque, 1:80 dilution), and PMS2 (MRQ-28, Cell Marque, 1:40 dilution)—was performed on four corresponding sections of 3–4 μm thickness obtained from the recipient block. Appropriate controls were used simultaneously. The slides were evaluated independently by 2 gynecologic pathologists. IHC was evaluated for retained or loss of nuclear expression of MMR proteins. Only cases that had identifiable internal controls were included for subsequent analysis. Any case of a patient with loss of expression of any one of the MMR proteins was grouped in the MMR loss/deficient category. Relationships of MMR loss, obesity, age, family history, and histomorphology were compared with loss of expression of any of the MMR proteins as a group as well as with individual losses of expression of MLH1, PMS2, MSH2 and MSH6.
Statistical analysis
Categorical variables were reported as counts and percentages. Group comparisons were made using a χ2 test or Fisher's exact test. Age was presented as mean and standard deviation. A Student's t-test was applied to compare any 2 groups. A p-value <0.05 was considered to be significant. All statistical analyses were conducted using IBM SPSS Statistics (version 22.0).
Results
A total of 83 cases of type 1 EC of the endometrioid-type diagnosed on hysterectomy specimens were included for the present study. The ages of the cases ranged from 30 to 74, with a mean of 54.9 years. There were 25 cases (30.1%) in the present study with patients' ages <50. Data for obesity were available in 60/83 cases, of which 50% were obese. Family histories of malignancy were present in 4 cases (4.8%), of which 1 patient had a history of gallbladder carcinoma in her parents; another patient had a history of carcinomas of the endometrium, breast, and stomach among her siblings. One patient had a previous personal history of breast cancer, and another patient had a personal history of anal cancer.
Evaluation of MMR protein accomplished was done by IHC performed on TMAs. Of the total 83 cases, loss of expression of any one of the MMR proteins was seen in 52 cases (62.7%) with the remaining cases showing retained expression of all the MMR proteins (Fig. 1). Among the four MMR proteins, loss of PMS2 expression was the most frequent loss, seen in 45 cases (54.2%), followed by loss of MLH1 expression in 41 cases (49.4%; Fig. 2) and loss of MSH2 expression in 26 cases (31.3%; Fig. 3).

Hematoxylin and eosin scanner (top left) 2 × and (top right) 10 × views of a case of endometrioid carcinoma showing retained nuclear expression of MLH1, PMS2, MSH2, and MSH6 (20 × ).
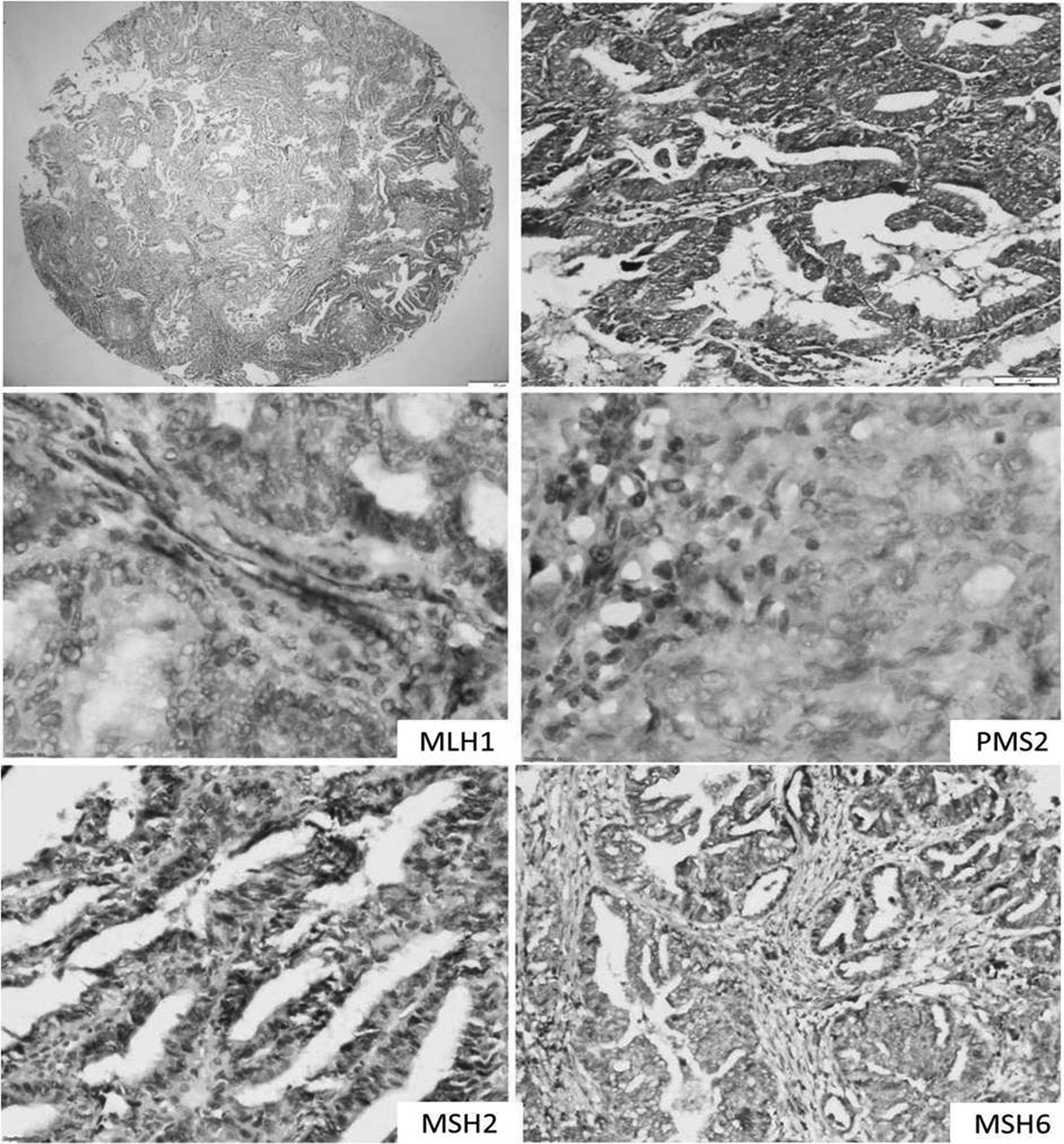
Hematoxylin and eosin scanner (top left) 2 × and (top right) 10 × views of a case of endometrioid carcinoma showing loss of expression of MLH1 and PMS2 in the tumor-cell nuclei with retained nuclear expression of MSH2 and MSH6 (20 × ).

Hematoxylin and eosin scanner (top left) 2 × and (top right) 10 × views of a case of endometrioid carcinoma showing loss of expression of MSH2 and MSH6 in the tumor-cell nuclei with retained nuclear expression of MLH1 and PMS2 (20 × ).
Of the patients who were <50 years old, 19/25 (76%) had loss of MMR expression. Among these patients, loss of MLH1 was most frequent, seen in 16 cases (64%), followed by PMS2 in 15 cases (60%). There were 6 cases with loss of expression of all four MMR proteins. However, it was found that loss of MSH6 expression alone as well as in association with MSH2, was significantly more frequent among these younger patients, compared to those >50 years old (p = 0.03). A single patient with a personal history of malignancy showed losses of MSH2 and MSH6 together (p = 0.331).
Obesity was not found to be significantly associated with loss of MMR expression (p = 0.592). Of the patients with family histories of malignancies, 2 (50%) had loss of MMR expression (p = 0.627) with 1 patient having loss of expression of MSH2 and another had loss of expression of MLH1/PMS2.
Tumor grade was the most significant predictor of MMR protein expression in endometrioid adenocarcinomas. Of the 83 cases in this study, 52 (62.7%) were low-grade endometrioid carcinomas, including both International Federation of Gynecology and Obstetrics grades 1 and 2 endometrioid carcinomas (Tables 2–4). Loss of expression of MMR proteins was significantly (p < 0.001) more frequent in the low-grade endometrioid carcinomas, with 41/52 cases (78.8%) having loss of expression of any one of the MMR proteins, compared to high-grade endometrial carcinomas, wherein only 11/31 cases (21.2%) had loss of MMR expression. Loss of expression of PMS2 was most frequent among the low-grade endometrioid carcinomas (n = 36; p < 0.001), followed by MLH1 (n = 33; p < 0.00). See Tables 2–4.
Comparison of Clinical Features of Patients with Deficient MMR Expression and Those with Retained MMR Expression
MMR, mismatch repair.
Comparison of Histopathologic Features of Patients with Deficient & with Retained MMR Expression
Bolding indicates significant result.
MMR, mismatch repair; TILs, tumor infiltrating lymphocytes; MELF, microcystic, elongated & fragmented; LUS, lower uterine segment; G, grade.
Comparison of Individual MMR Protein Expression with Histopathologic Features
Bolding indicates significant results.
MMR, mismatch repair; TILs, tumor-infiltrating lymphocytes; MELF, microcystic, elongated & fragmented; LUS, lower uterine segment.
Among the other morphologic features, higher density of tumor-infiltrating lymphocytes (TILs) was seen in 28 cases (53.8%) with loss of MMR expression; however, the association was not statistically significant. The cases with loss of MMR expression were found to have lesser degrees of myoinvasion, compared to the cases with retained MMR expression. In addition, the cases with MMR loss had less-frequent involvement of the lower uterine segment (LUS); lower tumor heterogeneity; infrequent microcystic, elongated, and fragmented (MELF) patterns of invasion; and less frequent lymph-node involvement. However, none of these morphologic parameters showed a statistically significant association with MMR status (Tables 2–4).
Discussion
Identification of an MMR gene defect in EC is important, as this has a role in prognostication and helps in choosing the appropriate adjuvant therapy for patients.13,14 Moreover, accurate assessment of MMR gene defects is fundamental for recognizing patients with EC who have LS.
In the present study, loss of expression of any one of the MMR proteins was seen in 52/83 cases (62.7%). This was higher, compared to previous studies. The majority of the reported data regarding MMR expression is from the developed countries of the world; thus, the current authors hypothesize that the higher rate of loss of expression in the current study might represent a higher loss in the developing countries of the world. However, this needs to be validated by larger studies. Alternatively, although the IHC was performed strictly according to the standardized protocol, theoretically, a loss of staining in a few cases might be attributed to factors related to tissue fixation. Genetic testing for germline mutations was not performed in the cases with loss of MMR expression. This was mainly due to the nonavailability of this function in the department and financial constraints associated with outsourcing such testing.
MMR gene defects can be detected by MSI analysis and/or IHC by evaluating the expression of four MMR proteins. In the present study, MMR deficiency was seen more commonly among younger females with EC (76%); however, the difference was not statistically significant (p = 0.09). Matthews et al. found abnormal MMR IHC in 34% of cases, among younger (< 50 years old) females with ECs. 15 However, Joehlin-Price et al. and Grzankowski et al. documented MMR loss in 16.2% and 19.6% of patients <50 years old, respectively.16,17 Long et al. also observed that women with MMR loss tended to be younger. 10
Among the individual MMR proteins, loss of expression of PMS2 was found to be the most frequent, followed by MLH1 in the present study. However, in the younger-age group (< 50 years old), MSH6 loss was significantly (p = 0.03) more common, compared to other MMR protein losses. However, these observations were in contrast to those by Joehlin-Price et al. 16
According to the literature, the majority of women who have ECs associated with MMR deficiency are nonobese with low BMI, indicating obesity to be less fundamental in the pathogenesis of MSI-related EC. Lu et al. compared 9 EC patients with MMR mutations to 91 EC patients without MMR mutations. 18 The mean BMI was higher in the latter group (35 kg/m 2 versus 29.2 kg/m 2 ). 18 Similar findings were noted by Matthews et al. and Grzankowski et al.15,17 In the present study, obesity was calculated as BMI >30.0 kg/m 2 , and, of 30 obese cases evaluated for MMR loss, 18 cases (60%) showed loss of expression of one or more of the four proteins. Of the four MMR proteins, PMS2 was the commonest protein lost in 15 cases. However, there was no significant statistical correlation with MMR loss.
Family history of cancer is an important risk factor in females with EC and might also indicate an association with LS. 18 History of colorectal cancer in particular is associated with LS. MMR protein expression was lost in 2 cases, 1 that showed loss of MLH1/PMS2 and 1 that showed loss of MSH2. Only 1 family met the criteria of LS. Shih et al., in their study of 56 endometrial cancer cases, noted that 2 cases had family histories of LS with MMR losses, which was statistically significant (p = 0.01). 19
Personal histories of any other cancers were noted in only 2 patients in the present study, 1 with a previous history of breast carcinoma and 1 with a previous history of anal carcinoma. Of these 2 cases, only 1 showed loss of MMR expression. In the present study, there was a significant correlation of MMR deficiency with lower-grade of EC (p < 0.001). Many researchers have found low-grade EC to be associated with MSI-high (MSI-H) more frequently. 20 Conflicting results were shown by Hirasawa et al. in which MSI-H–associated ECs were more likely to be high-grade (grade 3 versus grades 1 and 2). 21
In the present study, TILs were seen in 28 cases (59.6%) with MMR loss and 19 cases (40.4%) with retained expression of MMR proteins. However, no significant statistical difference was noted. TILs were found to be associated with PMS2 loss (53.2%; p = 0.83), but the association was not statistically significant. However, Shia et al. found TIL counts to be the most significant predictor of MSI, with a median TIL count to be fairly sensitive in discriminating MSI-H cases. 20 However, similar to the present study, Honoré et al. found a nonsignificant correlation between the presence of TILs and MSI. 22
Deep myometrial invasion was noted in 5/81 cases in the present study. It had been reported that cases with MSI-H were associated with deep myoinvasion. 23 However, in the present study, there was no significant association of deep myoinvasion with loss of MMR expression (p = 0.524). Similar results were noted by Ruiz et al. when they assessed the relationship between MMR deficiency and myometrial invasion in a large group of 212 EC patients and found the relationship to be nonsignificant. 24 However, 2 previous studies showed a positive correlation with myoinvasion and MMR loss.14,22 The other histopathologic parameters, such as MELF pattern of invasion, tumor heterogeneity, LUS involvement, and lymph-node status, were not significantly associated with MMR loss in the present study.
Conclusions
The present study highlights that a good number of endometrioid ECs are associated with MMR loss. Some of these cases might be associated with LS. Early identification of such cases by screening for MMR expression, followed by confirmation via mutation testing, is imperative, as the morbidity and mortality in these cases can be significantly reduced by implementing intensive cancer surveillance.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.