
Abstract
Abstract
Objective:
The aim of this study was to analyze indications, surgical routes, complications, and histopathologic correlations with preoperative diagnoses for all patients who underwent hysterectomies at a new teaching hospital over 5 years.
Materials and Methods:
This retrospective observational study included all women who underwent hysterectomy at a new medical college hospital in India from 2013 to 2017.
Results:
Hysterectomy was performed in 1.4% women attending the hospital's gynecologic outpatient department. Abdominal hysterectomy (72.7%) was the most-common surgical approach, followed by vaginal (18.6%) and laparoscopic (8.6%) approaches. The most-common indications for hysterectomy were symptomatic fibroid uteri (39.8%) and uterovaginal prolapse (17.6%). The overall complication rate was 7.1%. Preoperative diagnoses were confirmed by histopathology in 88.2% cases. The highest correlation (94%) was for fibroids and lowest correlation (70%) was for premalignant cervical lesions.
Conclusions:
Hysterectomy, as a definitive surgery in symptomatic women with benign pathologies, provides permanent relief. Patient satisfaction far outweighs short-term complications. Vaginal hysterectomy should be the default route. Prophylactic oophorectomy should be considered only after assessing the potential consequences of estrogen deficiency or subsequent ovarian malignancy. An audit of hysterectomies and major gynecologic surgeries is an indirect health indicator. The gynecologic work in the first 5 years of the new medical college hospital was almost on a par with major studies across countries. Shared decision making is definitely preferred when considering hysterectomy.
Introduction
Hysterectomy is the most common gynecologic surgical procedure in women across countries as a definitive treatment for benign conditions and can be a component of staging laparotomy. Concurrent salpingectomy and oophorectomy depends on each patient's age and indication for surgery.
An ideal decision for hysterectomy is made in consultation with the patient and is based on severity of functional impairment, availability and response to medical and conservative surgical therapies, future childbearing preferences, and presence of risk factors pertaining to either the patient's diagnosis or intended surgery.
Hysterectomy is performed abdominally, vaginally, or with a laparoscope. Surgical route depends on the surgeon's expertise, the medical indications, and the patient's condition. In the last 2 decades, laparoscopic hysterectomy (LH) has steadily replaced open surgery, irrespective of the indications and surgical options. 1 Reduced incisional morbidity and faster recovery are the main advantages in laparoscopy, whereas, learning curve and nonavailability of good equipment in remote areas are hindrances to LH. Thus, the conventional abdominal and the “no incision” vaginal approach (with the lowest complication rates and costs) are still in practice.
Hysterectomy is associated with physical and emotional complications as well as social and economic costs. 2 Women who have had hysterectomies enter menopause earlier, even with conserved ovaries. 3 Effective medical and conservative treatment for benign uterine pathologies has made some researchers question the use of hysterectomy for treating such pathologies and has caused major changes in management guidelines for abnormal uterine bleeding (AUB). Symptomatic women whose conditions do not respond to conservative management and who have no future fertility plans can benefit from hysterectomy. The effectiveness of hysterectomy for alleviating heavy menstrual bleeding, in terms of high satisfaction rates, is ∼95% for 3 years after surgery. 4 However, hysterectomy has a relatively high incidence of short-term complications, such as hemorrhage, infections, and wound-healing problems. 4
During the last decade, in India, there has been an increasing trend toward performing hysterectomies in younger women with benign pathologies.5,6 This has been attributed to the lack of a national registry of hysterectomies and nonavailability of baseline data for comparison, auditing, and future planning.5–7 This study was performed to analyze indications, surgical routes, and histopathologic correlations of preoperative diagnoses with all the hysterectomies performed at an Indian teaching hospital over a 5-year duration.
Materials and Methods
This retrospective study included all women who underwent hysterectomy at the Subbaiah Institute of Medical Sciences, in Shimoga, Karnataka, India, from 2013 to 2017. There were no exclusion criteria. All elective and emergency hysterectomies were included in the study.
Abdominal hysterectomy included subtotal hysterectomy, total abdominal hysterectomy (TAH), and TAH with unilateral (TAH + USO) or bilateral salpingo-ovariotomy/oophorectomy (TAH + BSO). Also included were hysterectomies performed as part of staging laparotomies or radical hysterectomies. Vaginal hysterectomies (VHs) included those performed with pelvic-floor repair and nondescent vaginal hysterectomies (NDVH). A third group consisted of LHs.
Baseline data regarding patients' characteristics, indications for surgery, routes of surgery and histopathologic reports were collected from case records and reviewed. Analysis was performed, using SPSS 16.0 Statistics 2007.
Results
From 2013 to 2017, a total of 17,576 women attended the Institute's outpatient department (OPD) for gynecologic complaints. Of these, 348 women underwent major gynecologic surgeries. Hysterectomy was performed in 256 women, which comprised 73% of the major gynecologic surgeries and 1.4% of total symptomatic women seen in the gynecologic OPD.
TAH was the most common surgery (n = 186 [72.7%]). This included 4 radical hysterectomies for early stage 1 carcinomas of the cervix and 3 peripartum hysterectomies performed as life-saving procedures for refractory postpartum hemorrhage. VH was performed in 48 women (18.6%) and LH was performed in 22 women (8.6%). See Table 1.
Routes of Hysterectomy and Indications
DUB, dysfunctional uterine bleeding; LAVH, laparoscopic-assisted vaginal hysterectomy; CIN, cervical intraepithelial neoplasia; NA, not applicable.
Symptomatic fibroid uterus (39.8%) was the most-common indication for hysterectomy, followed by prolapsed uterus (17.6%) and dysfunctional uterine bleeding (DUB; 14.8%). Other indications included adenomyosis (4.3%), ovarian cysts (5.9%), endometrial hyperplasia (6.7%), premalignant carcinoma of the cervix (7.8%), early carcinoma of the cervix (1.6%), benign recurrent postmenopausal bleeding (0.4%), and refractory postpartum hemorrhage (1.1%) See Table 1.
A total of 98.5% of the hysterectomies were performed as elective procedures. In 4 women who had emergency hysterectomies, 3 women had obstetric indications and the other patient was an older woman with a large twisted ovarian cyst.
The mean age of women undergoing hysterectomy was 46.6 ± 8.3 years (abdominal: 44.9 ± 6.7; vaginal: 54.4 ± 10.8; laparoscopic: 43.6 ± 3.9). The older age in the vaginal group might have been because of the increased incidence of uterine descent in postmenopausal women. Four women younger than age 30 underwent hysterectomy; of these women, 3 had obstetric indications, and 1 patient had DUB that was refractory to medical management with severe anemia and insisted on having a hysterectomy. Twenty-three women between ages 37 and 40 had completed their families and were not willing to undergo conservative treatment. Two women, age 34, underwent hysterectomy, due to severe symptomatic endometriosis with large endometriotic cysts, and another woman had third-degree uterine prolapse requiring definitive surgery.
Bilateral salpingo-oophorectomy (BSO) was performed in 64.1% of the women, with 90% between ages 40–60. Unilateral oophorectomy was performed in 4.7% of the women, most of whom were younger women ages <40. Only hysterectomy was performed in 31.3% of the women, most of who were in extremes of ages and who had normal ovaries.
Two women in this study were nulliparous. One was postmenopausal with a large 20-weeks–size fibroid uterus and the other was a 36-year-old with severe endometriosis and debilitating pain in her abdomen. All of the other patients were multiparous with completed families.
The most common symptoms in postmenopausal women (21.1%) were uterine prolapse and postmenopausal bleeding, whereas in perimenopausal women, it was AUB and pain in the abdomen (Table 2).
Symptoms & Percentages
The mean hospital stay was 6.78 ± 1.9 days. Women who underwent LH had shorter hospital stays, whereas women who had abdominal hysterectomy had average longer stays in the hospital.
The overall complication rate was 7.1% (Table 3). Intraoperative complications (3.5%) included hemorrhage and organ injury. Postoperative complications (3.6%) included wound infections, secondary hemorrhage, and debilitating systemic illnesses. These were classified by the Clavien–Dindo system, 8 in which grades 1 and 2 are minor complications, and grades 3 (requires surgical, endoscopic, or radiologic intervention) and 4 (life-threatening) are major complications. Most of the complications in this study were grade 3. Major wound infections (n = 7) were all in women who had TAH and required secondary suturing. All of these women had body mass indices in the obese range. Women who underwent obstetric hysterectomies required massive blood transfusions. In gynecologic hysterectomies, 12.1% women required postoperative blood transfusions.
Complications
UAE, uterine artery embolization; ICU, intensive care unit; DIC, disseminated intravascular coagulation.
One woman with a third-degree uterine prolapse had posterior-wall adhesions to the rectum and pouch of Douglas, thus could not be opened vaginally. Although laparotomy was performed, hysterectomy was abandoned (cervical amputation was performed) due to the dense adhesions and risk of major rectal injury. One woman who underwent NDVH presented 3 weeks later with symptoms of subacute intestinal obstruction (SAIO) that did not respond to conservative treatment; she had a laparotomy, ileal resection, and end-to-end anastomosis. A woman who had laparoscopically assisted VH (LAVH) had a laparotomy due to SAIO and appendicitis. Another LAVH woman had a bladder injury intraoperatively that was repaired immediately. One woman had a secondary hemorrhage that did not respond to medical management and was referred for uterine artery embolization (UAE). One woman, who was obese, hypertensive, and diabetic, had a myocardial infarction postoperatively and was admitted to the intensive care unit (ICU). One woman with postpartum hemorrhage had an amniotic-fluid embolism and disseminated intravascular coagulation, massive blood transfusions, a hysterectomy, and postoperative UAE and ICU care, but died after 3 weeks. Three women with primary Maylard incisions returned later with incisional hernias and had surgical repairs.
Preoperative diagnosis was confirmed by histopathologic examination in 88.2% of the cases (Table 4). The highest correlation (94%) was found with fibroid uteri (4% adenomyosis and 1% each for ovarian cysts and for endometrial polyps).
Correlation of Preoperative Diagnosis with Histopathologic Diagnosis
DUB, dysfunctional uterine bleeding; EH, endometrial hyperplasia; CIN, cervical intraepithelial hyperplasia; PMB, postmenopausal bleeding; PPH, postpartum hemorrhage.
In 42.7% of patients with fibroids, there were also concurrent pathologies. In women with mixed pathologies, endometrial hyperplasia was seen in 90.2% of women, adenomyosis in 7.3%, and ovarian cysts in 4%. There was a 100% correlation in patients diagnosed with cervical carcinoma. Only a 70% correlation was seen in women with premalignant cervical lesions diagnosed on Papanicolaou smears and colposcopic-guided biopsies. Two women with cervical intraepithelial neoplasia (CIN-3) had carcinoma in situ and 3 women with CIN 2 had normal cervices noted on histopathology. An interesting observation was that only 17.9% of women who had hysterectomies for DUB had normal uteri. Of the remaining cases, 56% of these women had endometrial pathology (endometrial hyperplasia in 90%, endometrial polyps, and endometritis) and 35% women had underlying adenomyosis. For hysterectomies for prolapses, pathologies, such as fibroids, adenomyosis, and CIN were noted in ∼17% women. Of 256 women who underwent hysterectomies, 51 had normal uteri (37 women with prolapse, 7 women with DUB, 3 women each with a preoperative diagnosis of endometrial hyperplasia and CIN, and 1 woman with recurrent postmenopausal bleeding).
Discussion
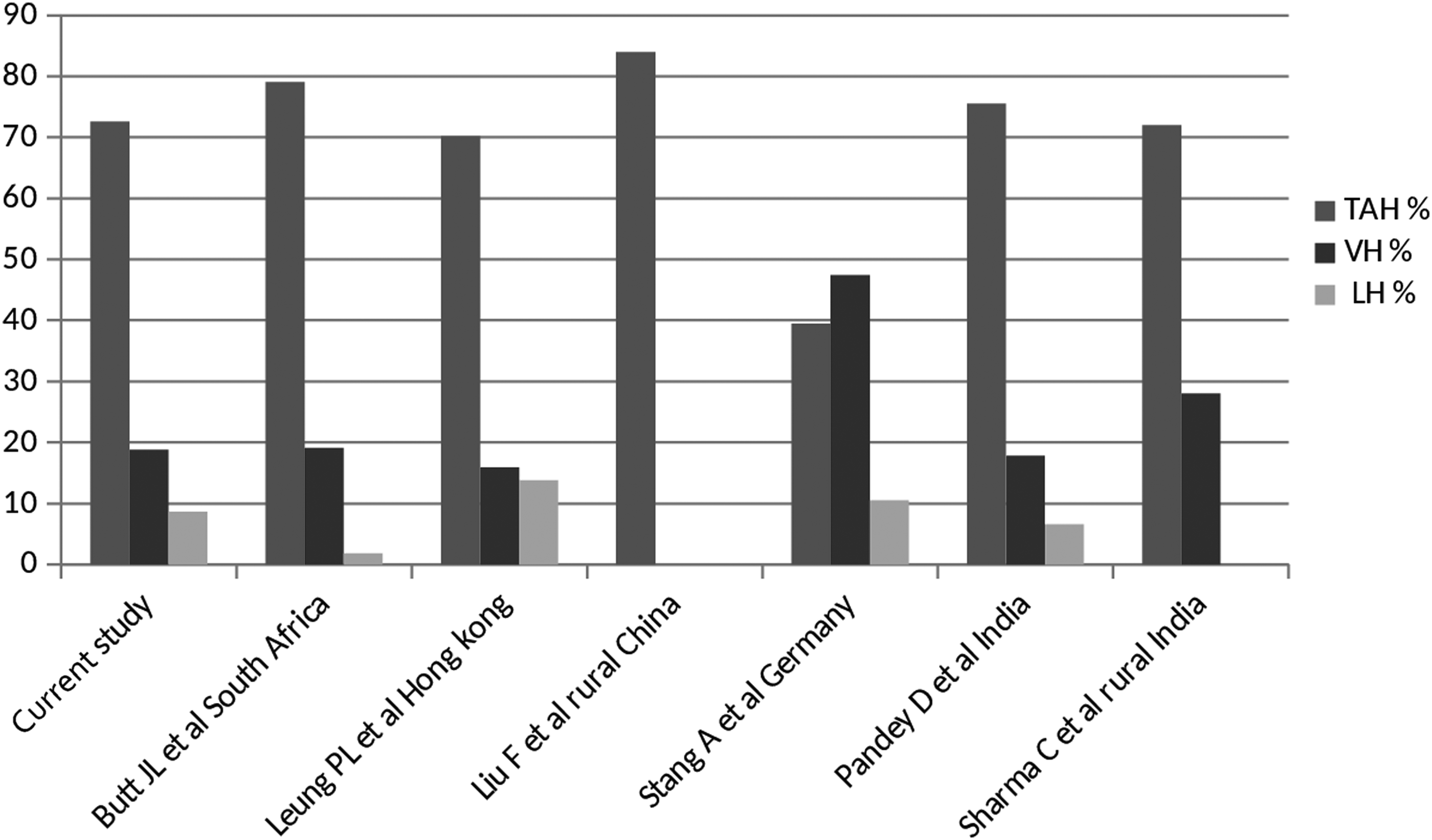
A total of 256 hysterectomies were performed over 5 years, of which 72.6% were abdominal, 18.8 % vaginal, and 8.6% laparoscopic procedures. This is in agreement with other audits in South Africa (TAH: 79.1%; VH: 19.1%; LAVH: 1.8%), 9 Hong Kong (TAH: 70.2%; VH: 15.9%; LH: 13.8%), 10 China (TAH: 84%), 11 and in another teaching hospital in India (TAH: 75.5%; VH: 17.8%; LH: 6.6%). 7 In Hong Kong, 10 LH was higher than in other places. In rural China, TAH was the dominant route for hysterectomy. 11 In contrast to these studies, Stang et al. 12 noted in Germany that VH (47.4%) was the most-preferred route followed by TAH (39.5%) and then LH (10.5%). See Figure 1 for this and other studies in selected countries.
VH as the route of choice in benign conditions should be recommended and preferred over TAH whenever possible. 13 If VH is not possible, LH should be chosen. TAH should be reserved only for special indications. Hysterectomy without a medical indication should not be performed solely on request of the patient. In the current authors' institution, route of hysterectomy was planned by the chief gynecologist, depending on each patient's characteristics (previous laparotomy, size of the mass, uterine descent, comorbid conditions) and consent after counseling regarding availability and financial feasibility.
A nationwide study in Portugal, by Gante et al., 14 from 2000 to 2014, and a study in Denmark by Lykke et al. 15 found that overall rates of hysterectomy had been reduced and that the average age of women undergoing surgery had increased. Laparoscopic and vaginal routes increased with a decline in the laparotomic route. Turner et al. 16 studied hysterectomy trends between 2000 and 2010 at the University of Pittsburgh and found that LH had surpassed TAH with a significant trend of increasing patient age. Mukhopadhaya and Manyonda, 17 in the United Kingdom, found decreases in surgery rates from 1995 to 2002 but an interesting plateau thereafter (until 2012), probably suggesting that alternative conservative therapy was ineffectual beyond certain clinical decisions and justified hysterectomy as the definitive treatment. India still lacks a national hysterectomy registry or a nationwide analysis of hysterectomies.
Sharma et al. 6 found that TAH (72%) was the most prevalent with a mean age of women undergoing surgery between 40 and 50. Prusty et al. 5 —in a district-level, household survey study held across 21 states and union territories of India—estimated a hysterectomy prevalence of 17 per 1000 ever-married women with a median age of 42. Increased parity and sterilization increased the surgical acceptance. Educated women and women of lower socioeconomic levels were less likely to opt for hysterectomy. The stark finding in this survey was that 36% of women who underwent hysterectomies were below age 40.
In the current study, the mean age of women undergoing hysterectomy was 46.5 ± 8.4 years, which correlated with other studies: 48 ± 9.9 years (Pandey et al. 7 ); 43 (Liu et al. 11 ); 51–55 ± 12.35 years (Gante et al. 14 ); 46–50 (Lykke et al. 15 ); and 46–51 (Turner et al. 16 ). The significant trend of increasing patient age could be due to younger women choosing alternatives to hysterectomy. In addition, over the past decades, anesthetic risks have been reduced and minimally invasive surgical approaches are practiced more. Hence, older patients are more likely to be offered—and undergo—advanced surgical procedures.
Benign conditions with general debility unresponsive to medical management are major indications for hysterectomy. In the current study, major indications for hysterectomy were symptomatic fibroid uterus (39.8% of total hysterectomies; 51.6% of TAHs; and 31.8% of LHs), prolapsed uterus (17.6% of total hysterectomies; and 93.7% of VHs), and AUB (14.8% of total hysterectomies; 15.9% of TAHs; and 36.3% of LHs). This correlated with Pandey et al., 7 Butt et al., 9 Leung et al., 10 and Liu et al., 11 and is in contrast to a study in Nepal Medical College, 18 where uterine prolapse was the major indication, followed by AUB. This result is supported by the fact that prolapsed uteri are common in high-altitude areas. Sharma et al., 6 in a retrospective study in a tertiary-care center in north India, reported AUB (52.5%) and prolapsed uteri (31%) as common indications, followed by fibroids and adenomyosis. According to German external hospital quality-assurance data, ∼60% of hysterectomies were performed to treat uterine fibroids. 12
Neis et al. 13 recommended hysterectomy for fibroids only if the patient's symptoms were actually fibroid-specific, she had no concern about future fertility, and her condition was unresponsive to treatment alternatives; in addition, she must indicate a wish to undergo hysterectomy after counseling regarding her treatment options. Endometrial ablation and hysterectomy are treatment options for women with AUB with failed medical therapy after ruling out premalignancy and malignancy. In endometriosis and adenomyosis, completed family and failed hormone therapy are considered indications for hysterectomy.
Mean hospitalization days (6.78 ± 1.9 days) in the current study were comparable with Indian data 7 but were higher, compared to other studies. Mean hospitalization days are reduced with changing routes and changing indications for hysterectomy. 14 In the United States, Turner et al. 16 reported an average length of stay of 1 ± 1 day for benign LH and 1.6 ± 1 days for VH (which were significantly shorter than the average 3.1 ± 2.3 days for TAH).
Hysterectomy has a higher incidence of short-term complications, such as hemorrhage, infection, and problems with wound healing. 19 Overall complication rates were 5.4% (intraoperative: 1.4%; and postoperative: 4%) in Germany, 13 8.5% in an Indian teaching hospital, 7 and 3.3%–3.% in Portugal. 14 Various studies7,9,10,17–19 across countries reported that the risk of complications was significantly lower in VH than in TAH and LH. Complications were higher in surgeries performed for malignancies. The overall complication rate in the current study was 7.1% (3.6% intraoperative and 3.5% postoperative). However, the blood-transfusion rate was significantly higher than in other studies, probably because the patients presented for surgery late or did not receive iron–sucrose supplementation due to financial constraints.
Concurrent oophorectomy is a common debatable practice with significant ramifications in reproductive-age women due to the consequences of estrogen deficiency or the risk of subsequent ovarian malignancy. Approximately 1.43% of women develop ovarian malignancy. 19 Of these, 4%–14% had previous hysterectomies with retained fallopian tubes and ovaries. Future surgical interventions for benign ovarian cysts are prevented by concurrent oophorectomy. 20 In benign hysterectomy, risk history (breast and ovarian cancer, age, menopausal symptoms, endometriosis, chronic pelvic pain), transvaginal ultrasound (to detect ovarian cysts), intraoperative gross appearance, and informed consent of the patient are factors considered when making a decision to perform an oophorectomy.
Stang et al. 12 reported overall concomitant bilateral ovariectomies in 23% of hysterectomies, commonly when there was carcinoma in situ or premalignant genital lesions. In hysterectomy for benign lesions, the overall rate was 12%, strongly depending on the age of the women at surgery. Turner et al. 16 and Gante et al. 14 showed a significant decrease in oophorectomy rates in benign hysterectomies (71%–51.9%), attributing this to the growing body of literature demonstrating the potential benefits of ovarian preservation. An overall incidence of concurrent BSO was 45% in rural India 6 ; this was attributed this to a lack of risk screening and postoperative follow-ups. The current study showed an overall BSO rate of 64.1%, especially in patients ages 40–60. It was an interesting finding that 40.2% of oophorectomy specimens had subclinical follicular cysts on histopathologic examination.
Hysterectomies for benign conditions have led to a perception of unjustified hysterectomies. 21 Bassey et al. 21 found that 76.7% of indications and pathology reports correlated, and that 3.3% had significant alternative pathologies, making hysterectomy justified in these cases. Pandey et al. 7 reported that histopathologic examinations (HPE) correlated with preoperative diagnoses in 84.1% of cases and 19.6% had additional pathologies.
In the current study, HPE correlations were achieved in 88.2% of the cases, with the highest in carcinomas of the cervix (100%) and fibroids (94%) and the lowest (70%) in premalignant cervical lesions. Additional pathology reporting of adenomyosis (7.3% of women with fibroids; 35% of women with DUB; and 8.8% of women with prolapsed uteri) makes it the most underdiagnosed condition. In refractory DUB, it is worthwhile to reassess the endometrium (56% of endometrial pathologies were noted in hysterectomy specimens) and suspect adenomyosis. Additional pathologies (17%)—such as fibroids, endometrial hyperplasia, adenomyosis and CIN in prolapsed uteri—raise a question regarding the justifications for conservative surgeries12,13 for major pelvic organ prolapse.
The successful outcome of a procedure for a benign condition is alleviation of symptoms, improved quality of life (QoL), prevention of future malignancy, and patient satisfaction. Women differ in the distress they experience and in their future plans. However, their expectations would be correct evaluations, diagnoses, and available options. An informed decision is essential before planning further management. 13 To achieve the best outcome, the option of surgery should be evaluated meticulously (for availability, response, success, and recurrence rates) along with conservative options.
Oral medications alleviate symptoms but patient compliance over prolonged durations is a major limiting factor. 4 Endometrial ablation is an alternative to hysterectomy in endometrial pathology and can stop bleeding associated with other pathologies. Recurrence of symptoms and need of retreatment makes this ablation less popular. 4 UAE and a levonorgestrel intrauterine system is comparable to hysterectomy in terms of patient satisfaction and better QoL. However, limitations include minor side-effects and probable need for hysterectomy later.
Auditing of hysterectomies and major gynecologic procedures is an integral part of every medical college and is an indirect health indicator. Accurate data regarding number of patients, indications for surgery, postoperative complications, and blood transfusions are available only from developed countries. This retrospective study was performed to audit the data of gynecologic work in the first 5 years of a new medical college hospital in India. It should be noted that the results are almost on a par with all major studies across countries. Although the current authors did believe that many TAHs could have been either LHs or VHs, the major hindering factors were lacks of patient consent, lack of cost-effectiveness (for LH), and learning curves. From this data, the current authors would like to move on to prospective studies and have made Clavien–Dindo classification of complications integral to the authors' clinical work.
Conclusions
Hysterectomy should be considered as a definitive treatment for achieving permanent relief in symptomatic women with benign pathologies, who have no future fertility requirements, and for whom conservative options failed or are contraindicated. Patient satisfaction far outweighs the short-term complications. VH should be the default route. Laparoscopic and abdominal approaches may be preferable depending on pelvic pathology, patient factors, and surgeons' and patients' preferences. Prophylactic BSO should be considered only after assessing potential risks and benefits and obtaining the woman's consent. An approach of shared decision-making would definitely be preferred when considering hysterectomy. 22
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.