
Abstract
Abstract
Objective:
The goal of this study was to perform microscopic and macroscopic analyses of reanastomosis of the rat uterine horn, with and without prolonged Nelaton catheter use.
Materials and Methods:
Nine rats with bilaterally sectioned and reanastomosed uterine horns were analyzed. The left uterine horn was reanastomosed with prolonged use of a Nelaton catheter (group 1; G1), and the right horn was reanastomosed without catheter use (group 0; G0). After 14 days, the rats were euthanized, and their uterine horns were removed. Microscopic and macroscopic analyses were performed.
Results:
Microscopic analysis revealed a fibrotic presence rate of 44.4% and an absence rate of 55.6% in G0. In G1, a higher fibrotic presence rate of 66.6% was found. The inflammatory infiltrate was considered mild in 11.1%, moderate in 55.6%, and intense in 33.3% of the G1 uterine horns, whereas it was considered mild in 66.6%, moderate in 33.3%, and 0% of the G0 uterine horns (p = 0.029). In G0, mild, moderate, and intense neovascularization was found in 5 rats (55.5%), 3 rats (33.3%), and 1 rat (11.1%), respectively, whereas, in G1, mild, moderate, and intense neovascularization was found in 3 rats (33.3%) each (p = 0.470). Granulomas were present in 7 uterine horns (77.8%) in G0 and in 9 uterine horns (100%) in G1. Unexpected findings were only noted in G0.
Conclusions:
Prolonged use of the Nelaton catheter for bilateral reanastomosis of the rat uterine horn led to an increased inflammatory response and an absence of unexpected findings.
Introduction
Tubal ligation is the most widely used contraceptive method worldwide. The frequency of this procedure varies among countries, but the average is ∼20%. Postoperative regret usually occurs for family reasons or following loss of children, with a rate ranging from 6% to 20%. In addition, 1%–5% of women desire tubal reanastomosis (TR), which has a success rate ranging from 41% to 93%.1–4
The American Society of Reproductive Medicine supports TR as an option for treating patients who have undergone tubal ligation. Despite the increasing use and improvement of in-vitro fertilization (IVF) techniques, the global success rate is similar for both approaches. Notably, TR has a lower cost than IVF. 2
TR basically consists of opening the occluded distal and proximal ends of the fallopian tube, with patency confirmed by using methylene blue. Then, the permeable ends are brought together, and the serosal and muscularis layers are sutured separately with varying numbers of stitches; in some instances, the mucosal layer is also sutured.1,4,5 Some techniques involve use of a splint or a catheter when suturing the proximal and distal segments; this catheter or splint is subsequently removed and is not present during the healing process.1–5
Wound healing is a complex process involving the organization of cells, chemical signals, and an extracellular matrix to repair the damaged tissue. 6 Fibroblast activity and wound contraction during the remodeling phase can lead to stenosis in tubular organs, such as the ureter and urethra, which is prevented routinely with the use of a double-J stent or bladder catheter, respectively.7,8 Human uterine tubes and rat uterine horns have similarities in that they are tubular and have been used together in previous studies, because the uterus and the horn merge into one structure in rodents. 9
Given the importance and utility of TR, the objective of this study was to investigate reanastomosis of the uterine horns of Wistar rats with permanent implantation of a Nelaton catheter to evaluate the inflammatory response, tubal patency, neovascularization, necrosis, and other findings related to the histologic characteristics of healing. Another goal was to assess the possibility of prolonged catheter use in TR surgeries.
Materials and Methods
This study was an experimental study with Wistar rats (Rattus norvegicus albinus) obtained from the vivarium of the Federal University of Maranhão (Universidade Federal do Maranhão; UFMA), in Maranhão, Brazil, and was conducted from March 1, 2018, to March 30, 2018.
The study was performed in accordance with Brazilian legislation on the use of experimental animals (Arouca Law Number 11,794/2008); the guidelines from the Brazilian College of Animal Experimentation (Colégio Brasileiro de Experimentação Animal), which is an institution affiliated with the International Council for Laboratory Animal Science; and the Ethics Committee on the Use of Animals (Comitê de Ética de Uso de Animais) of the UFMA. The study began after receiving approval from the Ethics Committee on Animal Use of the Presidente Dutra University Hospital, UFMA, under protocol Number 23115.005784/2016-46.
The surgeries were performed at the Laboratory of Experimental Surgery of Maranhão (LabCEMA) in the Mother–Child Unit of the University Hospital (Hospital Universitário Unidade Materno–Infantil).
Nine 180-day-old adult female virgin Wistar rats, weighing between 180 g and 250 g, were selected. The animals were grouped with 5 or 4 animals per polypropylene cage. The cages had stainless-steel wire bar lids and measured 46 cm × 31 cm × 16 cm; the cage bottoms were lined with wood shavings that were changed every 48 hours. The rats were kept under constant environmental conditions and received food rations for rats (Purina,® São Paulo, Brazil) and water ad libitum for 7 days for adaptation. The room where the cages were kept was subjected to noise control, a 22°C ± 2°C temperature, 40%–60% relative humidity, and 12-hour light and dark cycles.
The rats were labeled, using a 4-mm permanent marker (Pilot,® São Paulo), and were monitored daily, as well as recording the dates, weights, complications, and observations.
Each rat served as an experimental and control animal simultaneously. The left uterine horn was reanastomosed using a Nelaton catheter Number 4 (nontoxic, silicone-coated polyvinyl chloride; Embramed,® São Paulo) and was in G1, whereas the right uterine horn was reanastomosed without using this catheter and was in G0.
The rats were subjected to a 12-hour fast and weighed in an electronic balance device (Marte® A500, Minas Gerais); the values obtained (in g) were recorded. After weighing, the rats were anesthetized with a mixture of 2% xylazine (Calmiun 2%,® São Paulo) and 5% ketamine (São Paulo) at a 1:1 ratio and at a dose of 0.2 mL per 100 g of weight. The mixture was injected intramuscularly with a 13 mm × 4.5 mm hypodermic needle (Becton Dickinson, Paraná, Brazil) on the posterior edge of each rat's left thigh. Anesthetic efficacy was verified by the loss of corneal-eyelid and tail reflexes. Then, each rat was placed on a 20 cm × 30 cm wooden board. Fur was manually removed from the abdominal caudal region, antisepsis with polyvinyl pyrrolidone–iodine (Povidine Tópico,® São Paulo) was performed, and a surgical drape was put in place.
The reanastomosis performed on both uterine horns of each Wistar rat was microsurgical tubal reanastomosis by a temporary, loose, parallel, 4-quadrant suture technique. 5 A 3-cm midline incision was made on the caudal third of the abdomen with a Number 15 scalpel (Solidor,® Minas Gerais, Brazil) by cutting through the skin, muscular aponeurotic plane, and peritoneum, followed by identification of the organs in the abdominal cavity and the uterine horns. In the left uterine horn, a transverse incision was made with a Number 15 scalpel, followed by passage of the aspiration catheter and termino–terminal suturing with 910-polyglactin suture number 6-0 (Vicryl® Coated/Ethicon, São Paulo) with equidistantly separated stitches in sets of 3. After reanastomosis, the catheter was attached to the lower part of the same uterine horn with a transfixion suture to avoid expulsion. In the right uterine horn, only the transverse incision and suture described above were made, with no catheter placement or attachment (Fig. 1).
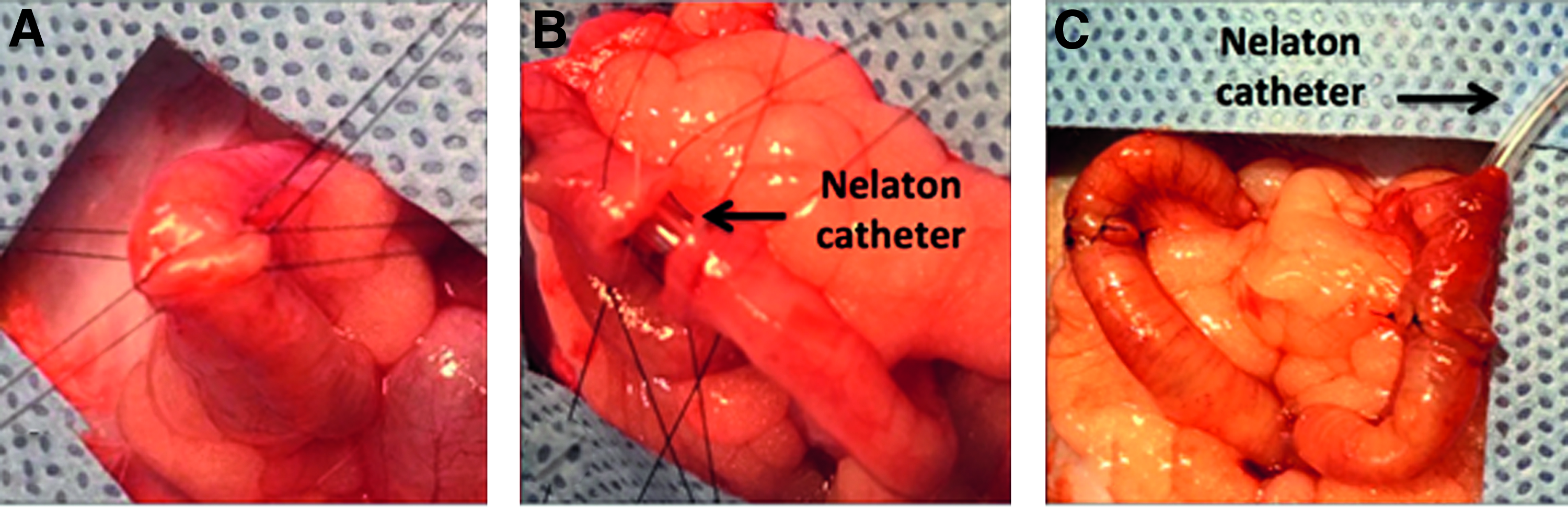
Surgical procedure in a Wistar rat with temporary, loose parallel sutures in the 6 o'clock, 12 o'clock, 3 o'clock, and 9 o'clock positions:
Fourteen days after the procedure, the rats were euthanized and evaluated. Euthanasia was accomplished with sodium thiopental injection (Tiopental,® Cristália, São Paulo) at a dose of 150 mg/kg delivered intraperitoneally according to resolution Number14 on June 20, 2002, of the Federal Council of Veterinary Medicine of Brazil. Death was defined as respiratory arrest and complete lack of reflexes. 10
After confirmation of death, the animals were subjected to surgery, and tube patency was assessed using a methylene blue chromopertubation test in both groups. The uterine horn was sectioned below the anastomosis, and the chromopertubation test was performed by inserting a probe for methylene-blue injection and observing its exit in the opening posterior to the reanastomosis. Then, the samples were incinerated according to the LabCEMA protocol.
The removed specimens were cleaned with 0.9% sodium chloride, placed in a container containing 10% buffered formalin, labeled, and sent to the UFMA Hospital's pathology department. The samples were processed and the blocks were sent for histologic evaluation by the pathologist.
After the preparation stage, the slides were examined by the pathology department. The following criteria were analyzed in each group: cell necrosis; presence of neovascularization; inflammatory lymphomononuclear infiltrate (shown by hematoxylin and eosin staining); and presence of fibrosis (shown by Masson's trichrome staining).
Necrosis was evaluated as present or absent, with absence defined as involvement of 0% of the tissue in the examined slide. The collagen and smooth-muscle fiber contents in the tissue (fibrosis) were evaluated, using Masson's trichrome staining, and classified as the presence or absence of fibrosis. The presence of an inflammatory lymphomononuclear infiltrate was rated as follows: mild, up to 33%; moderate, 34%–66%; and intense, 67%–100%. These histopathologic evaluation criteria were formulated by the Department of Pathology of the Presidente Dutra University Hospital–UFMA, based on the literature.11–13
The data were organized in a database (Microsoft Excel), and the Stat Plus: Mac Pro, version 6, program was used for the statistical analysis. The following statistical tests were used to evaluate the association of the use or no use of the Nelaton catheter with the histologic variables: χ2 test for inflammatory infiltrate, neovascularization, and unexpected findings; and Fisher's exact test for fibrosis and granulomas. The level of significance to reject the null hypothesis was p < 0.05.
Results
The weights of the rats varied from 215 g to 250 g. The surgery time ranged from 14 minutes to 16 minutes from skin incision to full closure.
Macroscopic analysis of the abdominal cavities of the 9 rats was not the objective of this study and did not show alterations that could have compromised the study, such as purulent secretions; signs of peritonitis; severe fibrotic adhesions; or adhesions between the loops, uteri, and/or abdominal walls at the end of the experiment.
The microscopic analysis revealed a fibrotic presence rate of 44.4% and an absence rate of 55.6% in the G0 group (Table 1). In the G1 group, a higher fibrotic rate (66.6%) was noted, but the difference between the groups was not significant (p = 0.637).
Histologic Evaluations, Unexpected Findings, & Evaluation of Uterine Horn Patency of Wistar rats Without (G0) and With (G1) Nelaton Catheters
The inflammatory infiltrate was classified as mild, moderate, or intense. The G1 group showed 11.1% mild, 55.6% moderate, and 33.3% intense inflammatory infiltrates. In the G0 group, 66.6% of the uterine horns had mild, 33.3% had moderate, and none had intense inflammatory infiltrate (Table 1). A significant difference (p = 0.029) was noted between the groups, with a more-severe inflammatory process in the group with the permanent Nelaton catheters.
Neovascularization (Fig. 2A) was classified as mild, moderate, or intense. In the G0 group, 55.6% of the uterine horns showed mild, 33.3% moderate, and 11.1% intense neovascularization (Table 1). The G1 group uterine horns showed 33.3% of all three forms of neovascularization (mild, moderate, and intense) (p = 0.472).
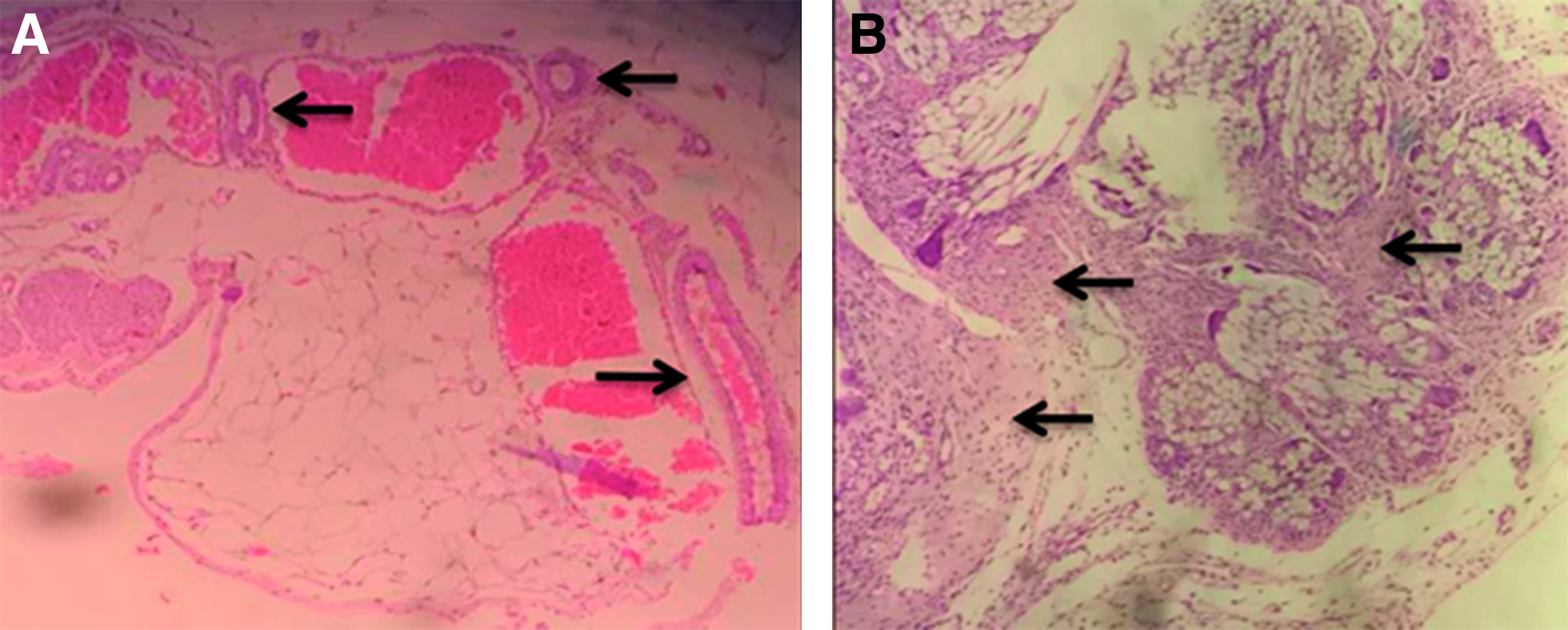
Granulomas (Fig. 2B) were present in 77.8% of the slides in the G0 and in 100% of the slides in the G1 groups (p = 0.470). Among the unexpected findings, abscess formation (n = 1), glandular dilatation (n = 2), marked eosinophilia (n = 1), and endometritis with ulceration of the epithelium (n = 1) were noted in the G0 group. Although these findings were not found in G1 (Table 1), no significant difference was detected (p = 0.140). Tubal patency was observed in 100% of the cases in both groups (Table 1).
Discussion
Uterine tubes are essential for natural fertility. They play important roles in ovum, spermatozoon, and embryo transport. These tubes are also essential for sperm capacitation and egg fertilization. Tubal reanastomosis is an alternative treatment for women with infertility caused by obstructions and for women who had chosen surgical sterilization and then wanted to become pregnant, because they had found new partners, lost children, had financial improvements, or other reasons.1–4
Assisted reproduction technology has gained traction, and surgical treatments as primary therapies have been questioned; however, careful patient selection, using appropriate screening methods and microsurgery techniques and principles, have led to results comparable to those of IVF.12,14
Use of rat uterine horns as a model of human uterine tubes has been chosen for medical research studies to investigate biologic changes in the epithelium of the distal portion of the ligated uterine tubes. 9 In the present study, prolonged use of a Nelaton catheter in rats was applied only to investigate possible advantages and future use in the uterine tubes of humans.
Typically, a catheter is used for treatment of tubal obstruction in the proximal interstitial portion of the uterine tube and is aided by hysteroscopy, laparoscopy, and radiology. Other studies have used catheters to aid suturing in tubal reanastomosis and then removed the catheters.1,2,4,5,15 The current study proposed leaving the Nelaton catheters in place for 14 days, which corresponded to the inflammation and proliferation time of the healing process.
This study used coated Vicryl 6-0, which is a synthetic, sterile and absorbable surgical thread coated with a mixture of equal parts of polyglactin 370 copolymer (30% glycolide and 70%
With the use of polyglactin thread, microscopic changes, such as mononuclear-cell infiltration and interstitial fibrosis, appear to favor the formation of granulomas. 16 In the present study, granulomas were present in 77.8% of the slides from G0 and in 100% of the slides from G1; catheter use (p = 0.470) did not appear to affect granuloma formation significantly.
The inflammatory response is very important for any type of injury and healing. Some local and systemic factors might interfere with this process. Local factors are mainly related to the movement and presence of residues within the wound, such as necrotic tissue, foreign bodies, bacterial contamination, and tissue hypoxia. Such residues can act as physical barriers against the orderly development of granulation and collagen deposition or can exaggerate inflammation, thereby affecting the inflammatory response.17–19
Only the inflammatory infiltrate variable presented a significant association (p < 0.029). The catheter produced a moderate-to-intense inflammatory infiltrate in 88.9% of the horns, whereas only 44.4% of the horns in which a catheter was not used had moderate-to-intense inflammatory infiltrate. Thus, this study showed that catheter use led to higher inflammatory responses during the healing process.
Fibrosis is described as the replacement of a functional tissue with another tissue with less-elastic characteristics (connective tissue) and with properties different from those of the original tissue. Fibrosis is present during the reconstruction of lesions and is part of the healing process.18,19 Because fibrosis creates a replacement tissue that is less similar to the healthy tissue, fibrosis can be considered a negative effect in reanastomosis. In the present study, a greater presence of fibrosis was found in G1 (66.6%) than in G0 (44.4%), although the difference was not significant (p = 0.637).
The unexpected findings were abscess, glandular dilatation, acute eosinophilia, and endometritis with an ulcerated epithelium. The G1 group, which used the Nelaton catheter, did not have any cases of unexpected findings. The reason for this result is unclear.
Conclusions
The final objective of reanastomosis was achieved because all samples were patent, which was crucial for allowing the return of fertility. However, the presence of a higher inflammatory response in the group that used the Nelaton catheter was expected due to the presence of the foreign body and lower mobility of the operated organ.18–20 Future studies should be conducted with materials that produce lower foreign-body reactions to develop another TR option, given that surgical success is not 100%; a better approach increases the possibility of successful surgical treatment of obstructed tubes in patients with poor prognoses.1,2
The use of the Nelaton catheter during bilateral reanastomosis of the rat uterine horn led to an increase in inflammatory responses and an absence of unexpected findings; and did not appear to affect tubal patency, neovascularization, or presence of necrosis and fibrosis.
Footnotes
Acknowledgements
The authors acknowledge the help of the Experimental Surgery Laboratory of the University Hospital of the Federal University of Maranhão.
Author Disclosure Statement
No financial conflicts exist.