
Abstract
Abstract
Objective:
With the increasing age of the population, more elderly women undergo gynecologic surgery. While multiple studies have demonstrated the advantages of minimally invasive surgery (MIS), there is a paucity of data regarding MIS in elderly women. This study was performed to evaluate outcomes among elderly women undergoing gynecologic MIS.
Materials and Methods:
For this retrospective cohort study, medical records were reviewed for patients ≥65 years old who underwent MIS performed by gynecologic oncologists at a single institution between 2009 and 2016. Outcomes among “younger-elderly” (ages 65–79) and “older elderly” (≥ age 80) patients were compared.
Results:
Two-hundred and ninety-eight patients, age ≥65, underwent MIS (younger-elderly = 268; older-elderly = 29). The median age in the younger-elderly was 69 (range: 65–79) and, in the older-elderly patients, 83 (range: 80–93). The older-elderly had more medical comorbidities than the younger-elderly patients (median Charlson index: 7 versus 5; p < 0.001). There was no significant difference between the 2 groups with respect to surgical approach, underlying malignancy, conversion to laparotomy, and hospital stay. There was also no significant difference between the younger- and older-elderly patients in rates of complications, or in 30- and 90-day readmissions.
Conclusions:
MIS with early discharge is a safe approach in elderly patients undergoing surgery performed by gynecologic oncologists. Elderly age should not prohibit consideration of MIS with early hospital discharge.
Introduction
The United States has experienced a significant growth in its elderly population. People ages 65 and older account for 13% of the total U.S. population, and the number of people in this age group is increasing at a rate faster than the total population (15% versus 9%). 1 It is estimated that, by 2050, 70 million individuals will be over age 65, and the number of those over age of 85 is expected to double. 2
The aging population is projected to contribute to a rise in cases of patients with cancer diagnoses. 3 Importantly, the age-adjusted cancer mortality rate for patients older than age 65 is significantly greater (1068/100,000) than for those under age 65 (67/100,000). 3 Additionally, with advancing age, patients are affected by an increasing number of comorbidities posing greater surgical and anesthesia risks.
Minimally invasive surgery (MIS) methods, including vaginal, laparoscopic, and robotic-assisted laparoscopic surgery, are becoming more common in the field of gynecology. New data suggest that these methods are safe and feasible for treating elderly patients.4–10 Current studies have focused primarily on treatment of benign gynecologic conditions, and there is a paucity of data with specific evaluations of elderly patients undergoing MIS for gynecologic malignancies. Furthermore, many of the existing studies are limited by small sample sizes and restriction to the “younger-elderly” population, failing to address the special considerations for those over the age of 80. This study was conducted to evaluate outcomes among a large cohort of elderly patients, many of whom were “older-elderly,” who were undergoing MIS performed by gynecologic oncologists.
Materials and Methods
This study was approved by the New York University School of Medicines’ institutional review board. A retrospective review was conducted of all patients 65 years and older undergoing MIS performed by gynecologic oncologists at a single institution between January 1, 2009, and March 1, 2016. Patients were included in the study if they were age 65 or older and had undergone MIS performed by a gynecologic oncologist at the NYU Langone Medical Center, New York, NY. MIS approaches included robotic, laparoscopic, and vaginal surgeries. Due to the retrospective nature of this study, a waiver of authorization for informed consent was obtained. Clinical information was gathered from the electronic medical records. Two groups of elderly patients were defined: (1) younger-elderly patients, which included those ages 65–79; and (2) older-elderly patients, which included those age 80 and older.
Demographic data were collected for both groups—including ages, body mass indices (BMIs), medical comorbidities, preoperative diagnoses, postoperative diagnoses, and American Society of Anesthesiologists classes. Data were also collected regarding the surgeries and hospital stays—including operative times, types of MIS (robotic versus laparoscopic versus vaginal), conversions to laparotomy, reasons for conversion, estimated blood losses, perioperative and postoperative transfusions, complications, hospital stays (in days), and readmissions. Surgical and postsurgical outcomes were compared among the younger-elderly and older-elderly patients.
Statistical methods
Continuous variables used to compare outcomes for different age groups were tested for normality via the Kolmogorov–Smirnov test; univariate tests were applied according to whether the variables of interest were distributed normally (i.e., t-test) or not normally (i.e., Mann–Whitney-U test). Associations between categorical variables were evaluated with χ2 tests or Fisher's exact tests as appropriate for the category sizes.
The Charlson comorbidity index was used to assess medical comorbidities for patients. This tool is used to evaluate 22 conditions and to assign a score of 1, 2, 3, or 6. The condition scores were totaled for each patient, and the median scores were compared between the age groups. The acceptable α-error level was set at p = 0.05 for 2-tailed tests. Data were analyzed with SPSS statistical software (version 20, SPSS, Inc.).
Results
Two hundred and ninety-eight patients age ≥65 underwent MIS performed by gynecologic oncologists at NYU Langone Medical Center during the study period. Of these, 268 patients were in the younger-elderly group, and 29 patients were in the older-elderly group. The median ages at the time of surgery were 69 (range: 65–79) in the younger-elderly group and 83 (range 80–93) in the older-elderly group.
Table 1 outlines the characteristics of the 2 groups. The older-elderly group had more medical comorbidities than the younger-elderly group (median Charlson comorbidity index: 7 versus 5; p < 0.001). There was no significant difference between the 2 groups with respect to BMI, with median BMIs of 28 in the younger-elderly group and 27 in the older-elderly group (p = 0.450). There was no significant difference in rates of underlying malignancy between the groups, with 158 (59%) of the younger-elderly and 23 (79%) of the older-elderly patients having malignant indications for surgery (p = 0.096). Surgical times were similar between the 2 groups, with median operative times of 167 minutes (range: 56–425 minutes) for the younger-elderly and 133 minutes (range: 33–568 minutes) for the older-elderly (p = 0.127).
Surgical Outcomes in Elderly Patients Under and ≥ 80 yrs
yrs, years; min, minutes.
Surgical complications were rare, occurring in 8 (3%) of the younger-elderly patients, and there were no complications in the older-elderly patients (p = 0.436; Tables 1 and 2). There was no significant difference in the rates of conversion to laparotomy, with 34 (13%) and 4 (14%) of the younger- and older-elderly cases, respectively, being converted (p = 0.774; Table 1). The most common reason for converting to laparotomy in both groups was the ability to achieve complete tumor resection, with 22 (8%) in the younger-elderly group, and 4 (14%) in the older-elderly group. The following reasons for conversion in the younger-elderly group were adhesions (5), visualization (4), intolerance of pneumoperitoneum (2), and bleeding (1). There was also no difference with respect to surgical approach in the 2 groups, in which >60% of the patients in both groups underwent robotic surgery, and 28% versus 35% had laparoscopic surgery, and 1% versus 2% had vaginal surgery in the younger-elderly group and the older-elderly group, respectively. (Table 1; Fig. 1).
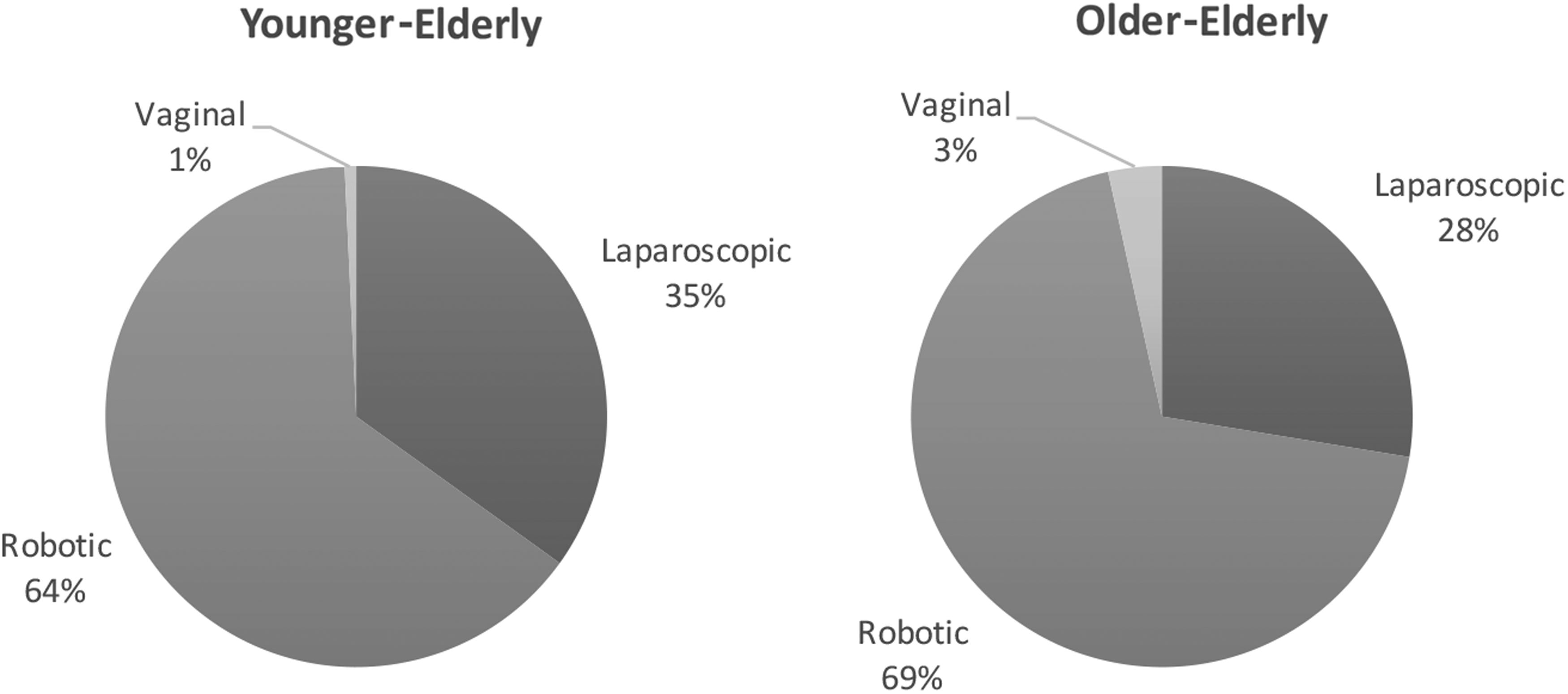
Surgical approach in “younger-elderly” and “older-elderly” patients. There was no difference with respect to surgical approach in the younger- and older-elderly groups, with more than 60% undergoing robotic surgery, ∼28%–35% undergoing laparoscopic surgery, and ≤3% undergoing vaginal surgery in both groups.
Surgical Complications in Younger- and Older-Elderly Patients
yrs, years.
Table 3 presents the hospital stays and readmissions for the younger- and older-elderly groups. Two hundred and eighteen (81%) younger-elderly patients and 22 (76%) older-elderly patients met criteria for ambulatory surgery, defined as an admission <24 hours (p = 0.310). The median length of hospital stay was 1 day for both groups (p = 0.689). There was no significant difference between the younger- and older-elderly patients with respect to rates of 30- and 90-day readmissions. Overall, 30- and 90-day hospital readmissions for both groups were rare, occurring in 13 (5%) and 2 (0.7%) of the younger-elderly group, and in 3 (10%) and 1 (3%) of the older-elderly group, respectively. Indications for hospital readmission among the younger-elderly group were port-site herniation (2), pelvic abscess (2), urosepsis (2), pleural effusion, small-bowel obstruction, anemia, diverticulitis, bowel injury, and lymphocele and fistula (1 each). Among the older-elderly, reasons for hospital readmission included port-site herniation, wound dehiscence, and acute kidney injury (1 each).
Hospital Stays and Readmissions
yrs, years, d, day(s); hrs, hours.
Discussion
The safety of MIS and same-day discharge were evaluated among elderly patients undergoing surgery performed by gynecologic oncologists. Overall, MIS with early hospital discharge was found to be a safe approach for elderly patients. While patients ≥80 years old were poorer surgical candidates, there were no significant differences in surgical outcomes or hospital stays, compared to the younger-elderly group.
The elderly gynecologic patient poses additional surgical challenges. She often has more medical comorbidities and less reserve for the thermoregulatory and fluid changes that occur during surgery. While MIS offers certain advantages, including less blood loss, decreased postoperative pain, shorter hospital stay, and faster recovery, this approach does present unique challenges, including pneumoperitoneum and, often, the necessity for steep Trendelenburg positioning.6–10 While these aspects of MIS might not be well-tolerated by the older-elderly patient, these aspects were not limiting factors in this study.
Previous studies have demonstrated the benefits of MIS in elderly patients, but the majority have focused on surgery for benign conditions and patients under age 80.6–9 The current study focused on patients undergoing surgery performed by gynecologic oncologists, with the majority of the patients having oncologic indications for surgery. While the overall sample size was larger than many prior studies, an important limitation was the small number of patients in the older-elderly group. Additional studies are necessary to evaluate the safety of MIS thoroughly in this unique patient population.
Conclusions
Although the older-elderly patients in the current study were poorer surgical candidates, compared to the younger-elderly patients, the surgical and postsurgical outcomes were similar in both groups. These patients should be counseled by their surgeons regarding the benefits of MIS, and carefully selected for this approach if determined to be good surgical candidates. Elderly age should not prohibit consideration of MIS with early hospital discharge.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.