
Abstract
Abstract
Background:
There is an increase in women complaining about having chronic pain, dyspareunia, and urologic symptoms due to adhesions after repeated cesarean sections. Laparoscopic adhesiolysis can reduce these patients' symptoms.
Cases:
Three women had dyspareunia, pain, and characteristic findings on gynecologic examination and ultrasounds after cesarean sections. laparoscopic adhesiolysis was performed in these patients to reduce their symptoms. All 3 had a second operations for different indications.
Results:
Photographs taken during the second operations showed no new adhesions in these 3 cases. The patients reported no dyspareunia, no urologic symptoms, and a decrease in pain (as shown by pain scores) after adhesiolysis.
Conclusions:
These findings indicate that laparoscopic adhesiolysis might be worth considering in severe cases of post-cesarean adhesion syndrome. The increasing rate of cesarean sections leads to more women with post-cesarean adhesion syndrome. Clinical attention must be paid to the triad of specific symptoms that can occur after cesarean section, as it is feasible to perform successful laparoscopic adhesiolysis. Recent literature suggests that 2-layer closure might be superior to 1-layer closure and that closing the peritoneum might help prevent adhesions.
Introduction
The current evidence-based Joel-Cohen technique from 2008 for cesarean section is recommended so that patients experience less fever, pain, and analgesic requirements, as well as losing less blood and having shorter surgeries and hospital stays. There is no information included on long-term morbidity, such as abnormal adhesive placental attachments or scar ruptures in subsequent pregnancies. Ectopic pregnancies in cesarean scars, niches (isthmoceles), pain, iatrogenic endometriosis, infertility, and ileus have also been described with increasing incidence after cesarean sections. The current authors have seen an increase in young women with chronic pain shortly after emergency or repeated cesareans but having delayed referrals to hospitals, due to negligence of their symptoms for some time (“doctor's delay”).
This article presents 3 cases of patients with severe symptoms due to adhesions after cesarean sections. The current authors performed laparoscopic adhesiolysis, using antiadhesive agents. Photographs from subsequent second operations for other indications were taken months after the adhesiolysis in the 3 patients, and these photographs are included in this article.
Cases
Case 1
A para 3 woman, with a vaginal delivery in 2006, had placental remnants. She requested a cesarean section in 2010. Then, in 2014, an emergency cesarean section was performed in gestational week 32 + 5, due to preterm premature rupture of the membranes. This patient had an accrete placenta. The uterotomy was sutured in 1 layer consecutively, with unlocked sutures and 3 extra-hemostatic sutures and nonclosure of the peritoneum.
Immediately after the procedure, the patient was examined for Ogilvie's syndrome, and showed only obstipation. However, 1 month after this patient's cesarean section, an ultrasound (US) showed formation of a niche with placental tissue (Fig. 1) and hysteroscopic resection was performed. A pathology report showed proliferative endometrium with decomposition and necrosis. A cervical bacteriologic sample showed Peptostreptococcus. Antibiotics were prescribed. After another month, she experienced severe pain especially when she had a full bladder. The cervix was not visible and was fixated behind the symphysis. There was still a Peptostreptococcus infection in the cervical sample.
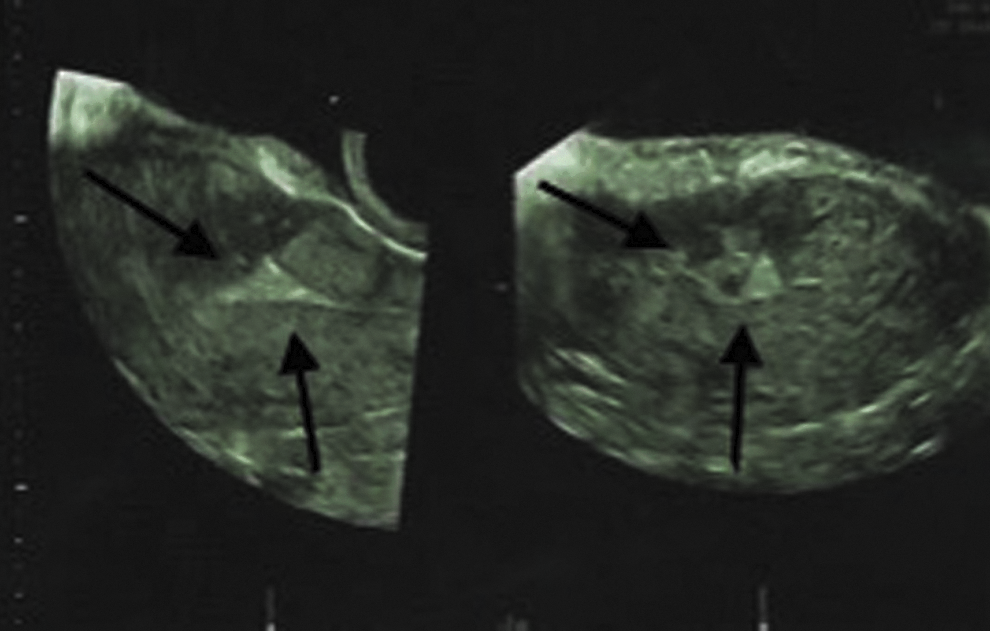
Case 1: 1 month after the cesarean section. Ultrasound showed a triangular hyperechoic area/niche (arrows) and irregular myometrium at the uterotomy.
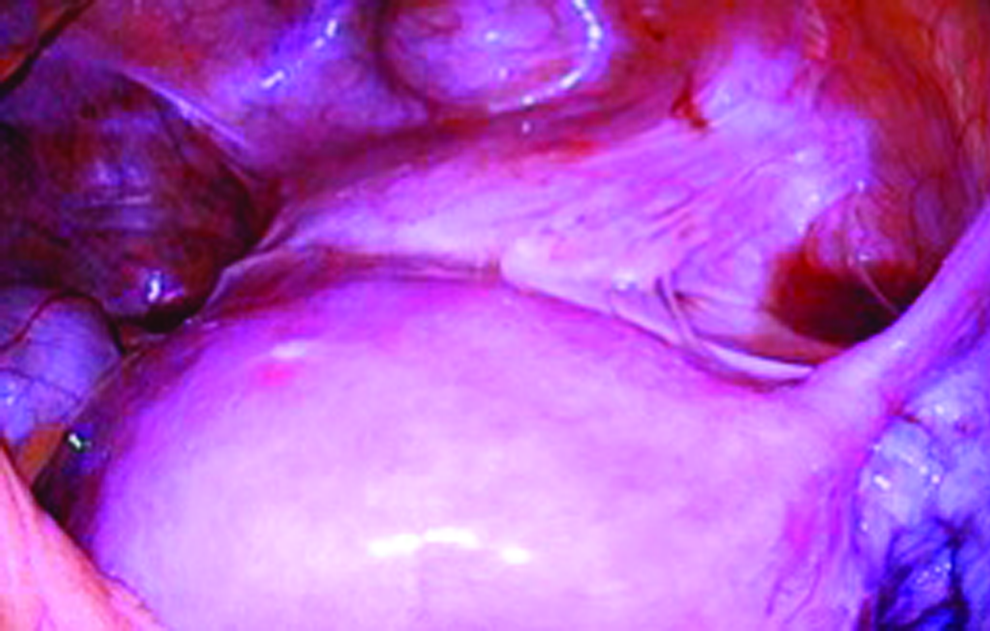
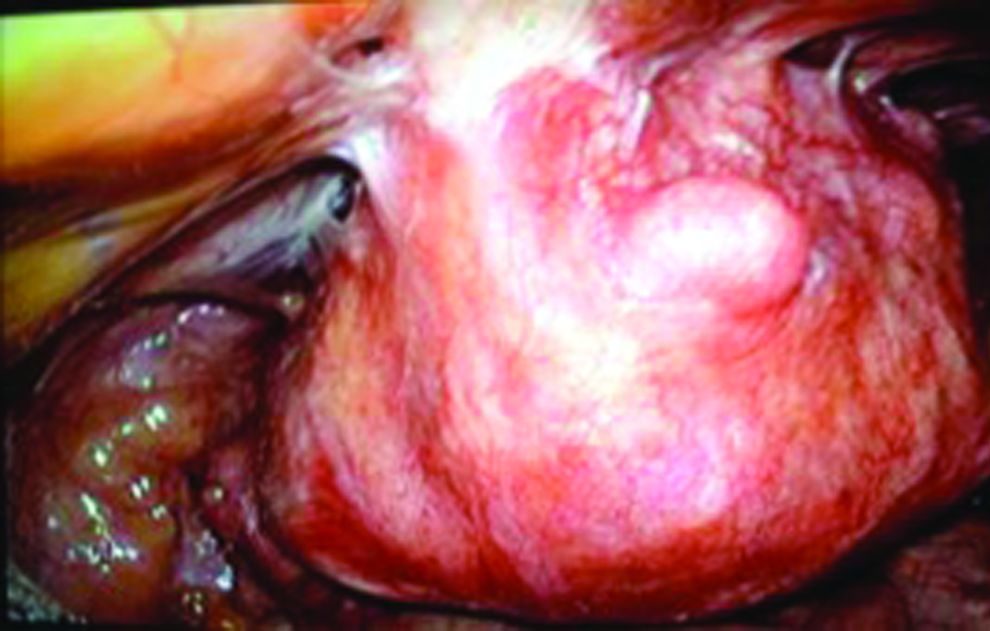
Three months after this patient's cesarean section, a laparoscopy was performed. The bladder was found embedded in adhesions and fixated to the uterotomy (Fig. 2). The adhesions were removed while the bladder was filled with 100–200 mL of saline in order to avoid bladder lesions. A hemostatic mèche was placed over the uterotomy, and antiadhesive gel was placed over the bladder and round ligaments.

Case 1: 3 months after the cesarean section. During the first operation, the patient's bladder was found embedded in adhesions and fixated to the uterotomy.
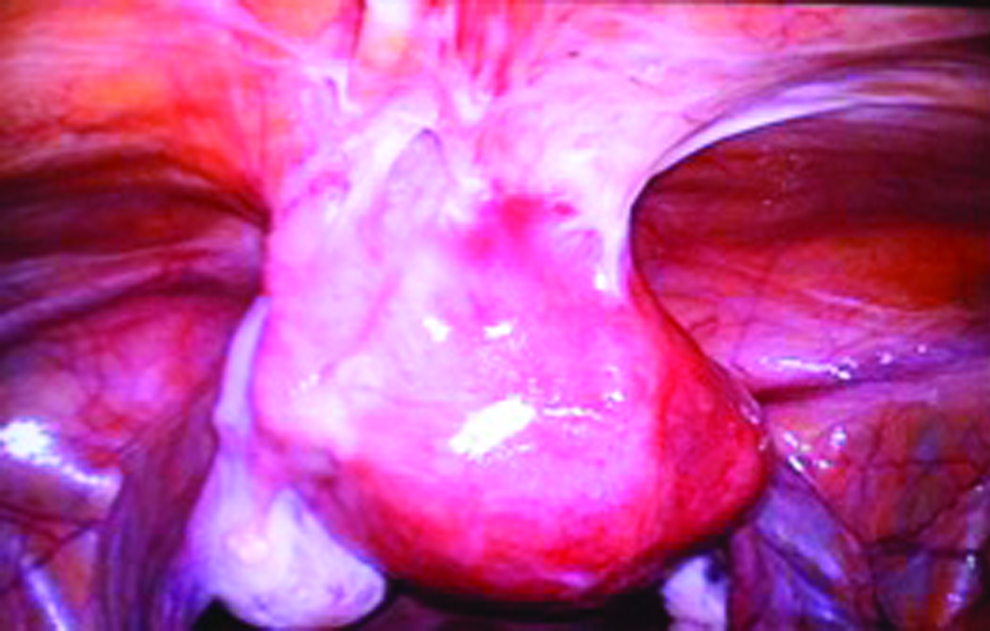
The patient had an initial decrease in pain score and no dyspareunia but, after a few menstrual periods, she complained of dysmenorrhea and opted for a hysterectomy. During this operation, which was performed 8 months after the cesarean section, the mèche was still visible, covering the uterotomy, but no new adhesions were seen (Fig. 3). She was without pain on the fourth postoperative day and still remained so at her 1-year follow-up.
Case 1: 8 months after the cesarean section. During the second operation, the mèche was visible covering the uterotomy. No new adhesions were seen.
Case 2
A para 3 woman had a history of 2 emergency cesarean sections. Nine years later, she had a gastric bypass, and, in 2014, had internal herniation in Peterson's space. One year after gastric bypass, she had lost 55 kg. However, this patient complained of experiencing pain during her abdominal exercises as well as having severe dyspareunia. Treatment for her pelvic-muscle tension was attempted without effect. The cervix was not visible; it was fixated behind the symphysis. US showed an anteflexed uterus with the isthmus fixated to the anterior abdominal wall with 2-cm–thick cicatricial fibroid tissue between the bladder and the uterus.
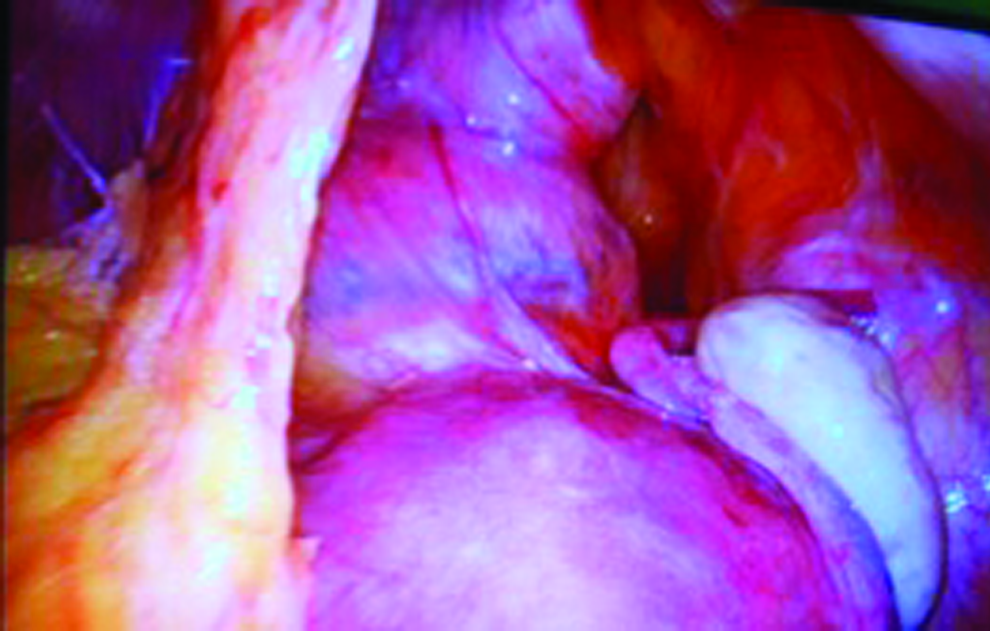
A diagnostic laparoscopy was performed and the uterus was found adherent to the anterior abdominal wall and the bladder was completely hidden (Fig. 4). The left salpinx and the left round ligament were invisibly adhesive between the rectus muscles. The adhesions were removed as described in Case 1 (Fig. 5).
Case 2: 15 years after the cesarean section. During the first operation, the uterus was found adhesive to the anterior abdominal wall, and the bladder was completely hidden. The left salpinx and the left round ligament were adhesive in-between the rectus muscles.
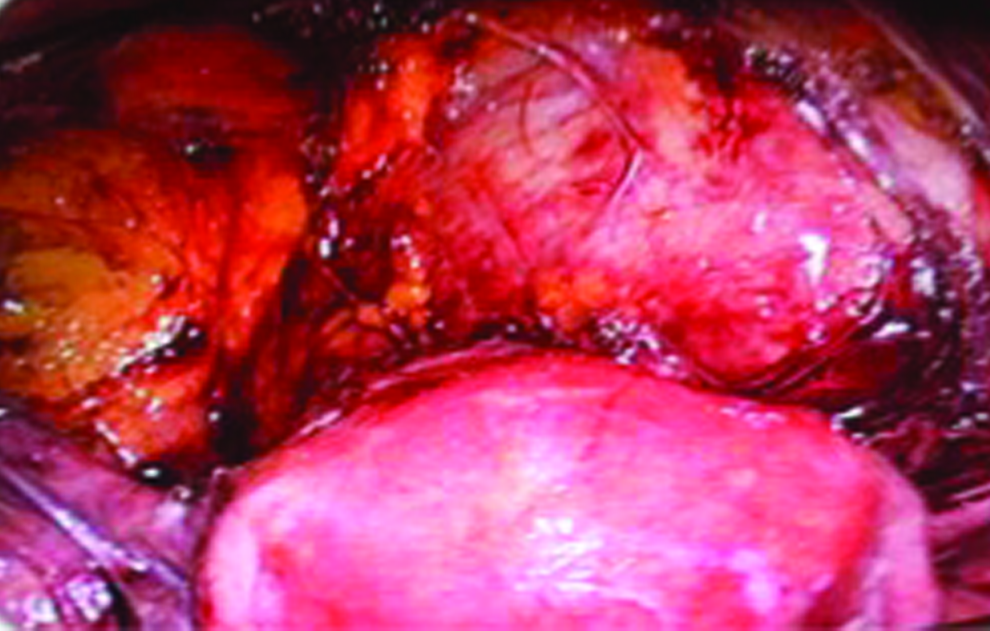
Case 2: 15 years after the cesarean section. During the first operation, the adhesions between the uterus and the bladder were removed. The bladder was filled with 200 mL of saline.
Three weeks after this surgery this patient experienced a distinct pain below the left side of her cesarean scar. Although her dyspareunia was gone, she insisted on a new laparoscopy. At this second look, no adhesions were found; only the mèche was visible on the front of the uterus (Fig. 6). However, in the abdominal wall, a 2-cm tumor was found between the fascia and the rectus muscle. The pathology report confirmed the suspicion of endometriosis, positive for CD10. The endometriosis was thought to be iatrogenic, possibly caused by the cesarean section. The patient's abdominal pain ceased after removal of the tumor.

Case 2: 15 years and 5 months after the cesarean section. During the second operation, no new adhesions were seen, and the mèche was visible on the front of the uterus.
Case 3:
A para 3 woman had a history of 2 emergency cesarean sections, the first due to disproportion and the other due to rupture of her uterine scar. During the second operation, the bladder was found to be adhesive on the front of the uterus, just below the rupture. This patient's third delivery, an elective cesarean section, was performed with the Joel–Cohen technique; the uterotomy was sutured in one layer with no peritoneal coverage.
Three years after the third cesarean section, this patient presented with lower abdominal pain and dyspareunia. US showed a niche, the uterus fixated toward the anterior abdominal wall, and the cervix fixated behind the symphysis. A laparoscopy was performed and the uterus was found to be adhesive to the anterior abdominal wall, the bladder was not visible, and the left round ligament was adhesive to the uterotomy (Fig. 7). The adhesions were removed as described in Case 1. Initially, the adhesiolysis had a good effect and the patient had no pain.
Case 3: 3 years after the cesarean section. During the first operation, the uterus was found fixated to the abdominal wall, the bladder was not visible, and the left round ligament was adhesive to the uterotomy.
However, her menorrhagia and dysmenorrhea gradually became worse, and she had an endometrial resection without effect; thus, a hysterectomy was planned. At that operation the bladder and front of the uterus were without adhesions, and the mèche was still visible over the uterotomy (Fig. 8).
Case 3: 3 years and 7 months after the cesarean section. During the second operation, only one adhesion was seen; it was from the omentum majus toward the anterior abdominal wall. The front of the uterus was visible, and the mèche was still visible over the uterotomy.
Results
The overall complaints from these patients presenting with post-cesarean adhesion syndrome comprised a triad of (1) dyspareunia, (2) lower abdominal pain at the rectus muscles, and (3) frequent urination combined with pain related to a filled bladder and during urination. The bladder symptoms and dyspareunia in all three cases disappeared after laparoscopic adhesiolysis, and the former fixated cervix became visible on gynecologic examinations. However, in these 3 cases, abdominal pain recurred for other reasons (chronic infection in the niche, iatrogenic endometriosis, and dysmenorrhea along with menorrhagia). However, the second operations performed after the adhesiolysis proved that these patient's adhesions did not recur.
Discussion
The current authors have had 27 patients with this triad of symptoms during the last 6 years, and these patients were all followed postoperatively. The pain disappeared quickly in the majority of these cases after adhesiolysis without new complaints.
In 2006, Van der Wal and colleagues stated, that considering the risk of complications associated with laparoscopic adhesiolysis, it should not be recommended as therapy for adhesion-related chronic abdominal pain. 1 The current authors' cases challenge that recommendation, as their patients had significantly improved quality of life (QoL) with sufficient bladder volume and no dyspareunia after adhesiolysis surgery.
In Denmark, ∼21% of all births are managed by cesarean section. 2 Evidence-based techniques for the different steps of this surgery have been published. 3 These recommendations were made on the basis of studies with only short-term follow-ups. With respect to long-term complications, a Danish study reported chronic pain in 4%–18% of patients 1 year after cesarean sections, with daily pain in 1%–6% of these patients. 2
A variety of antiadhesive agents have been developed to reduce adhesions after intra-abdominal surgery. It is possible to prevent de-novo adhesion formation by using adhesion barriers in gynecologic surgery. Furthermore, pelvic pain, QoL, and pregnancy rates are shown to improve after laparoscopic surgery using antiadhesive agents. 4 This strengthens the idea that patients presenting with the described triad of symptoms after cesarean section might benefit from laparoscopic adhesiolysis, as the 3 cases described in this article had no de-novo adhesions seen during their the second operations.
In the future with this high rate of cesarean deliveries, it can be important to focus on prevention of adhesions. A 2018 systematic review of literature on this topic, including 20 studies and 15,053 women, focused on long-term outcomes after cesarean sections. The review showed that double-layer unlocked sutures are preferable with respect to residual myometrial thickness, healing ratio, and dysmenorrhea. Furthermore, the reviewers found nonclosure of the parietal peritoneum was associated with more adhesion formation than closure. 5
The latter was consistent with the findings in another 2018 study on 250 women suffering from secondary infertility after cesarean sections. 6 The women were divided into three groups: (1) nonclosure of the peritoneum; (2) closure of the parietal peritoneum; and (3) closure of both the parietal and the visceral peritoneum. The researchers performed laparoscopy on all 250 women and found a statistically significant difference in adhesion formation among the 3 groups, with the nonclosure group having the most adhesions, mostly to a moderate or severe degree. In group 3, no patients had severe adhesions and only a few patients had moderate adhesions. The researchers concluded that closure of both the parietal and the visceral peritoneum, using proper surgical techniques for cesarean sections, led to fewer intra-abdominal adhesions; thus these closures and techniques were recommended.
Another 2018 article presented a critical analysis of the etiology of cesarean-section uterine-scar defects and the peritoneal-closure debate. 7 The author of that article stated that the uterotomy is best sutured in two layers of nonlocking continuous sutures without undue tightness and minimal inclusion of the decidua. Furthermore, this author advised closure of the uterovesical pouch of the peritoneum with just one or two interrupted sutures in order to prevent adhesion formation.
Conclusions
Increased attention should be given to the triad of symptoms after cesarean section: (1) dyspareunia; (2) voiding problems; and (3) an invisible cervix fixated behind the symphysis and a uterus fixated to the abdominal wall hiding the bladder. Laparoscopic adhesiolysis with modern technology can increase these patients' QoL without any de-novo adhesion formation. The time has come to reevaluate the evidence-based techniques used for cesarean sections, by taking potential long-term complications into account.
Footnotes
Acknowledgments
Kim Toftager-Larsen MD, DMSc (deceased January 8, 2018) made significant intellectual contributions to the research needed for this article and was involved in the manuscript writing process but could not give approval for the final version due to his death.
Author Disclosure Statement
No financial conflicts of interest exist.