
Abstract
Abstract
Background:
Cervical insufficiency is one cause of preterm birth and its associated neonatal outcomes. Transabdominal cerclage is an option for women with cervical insufficiency and a history of prior failed transvaginal cerclage or anatomical limitations to transvaginal cerclage. Case series and systematic reviews are increasing in the literature showing obstetrical and surgical benefits of laparoscopic and robotic approaches, compared to the conventional laparotomy approach. However, publications on this surgical intervention for women with cervical insufficiency and a pregnancy complicated by multifetal gestation are limited.
Case:
A 33-year-old, gravida 6, para 0140 African-American woman with history of recurrent cervical insufficiency, including 3 second-trimester deliveries and a prior failed transvaginal cerclage, underwent a robotic-assisted transabdominal cerclage in a trichorionic-triamniotic triplet pregnancy.
Results:
The patient had an uncomplicated postoperative course and her pregnancy resulted in a 35-week cesarean delivery of 3 healthy newborns.
Conclusions:
Prophylactic robotic-assisted transabdominal cerclage by an experienced surgeon is a feasible alternative for patients with cervical insufficiency in higher-order multifetal gestation pregnancies.
Introduction
Cervical insufficiency, defined as the inability of the uterine cervix to retain a pregnancy in the second trimester in the absence of uterine contractions, is a contributor to preterm birth and its associated neonatal morbidity and mortality. 1 Management of these gravidas includes expectant management, progesterone supplementation, a pessary, and/or cervical cerclage.2,3 While the vast majority of cerclages are performed via a transvaginal approach, transabdominal cerclage is reserved for a small subset of women with previous transvaginal cerclage failures and/or anatomical limitations to transvaginal placements.1,2 Transabdominal cerclage is performed either via a conventional laparotomy approach or laparoscopic or robotic approaches. Surgical techniques can vary, with most surgeons using a straight- or straightened-needle technique, while others have described a needleless technique.3,4
Transvaginal cerclage in multifetal gestation pregnancies is a controversial topic and is generally not recommended by societies, including the American College of Obstetricians and Gynecologists. 5 Isolated case reports of transabdominal cerclage in twins exist, with even less literature reporting on its use for higher-order multiples.6,7 This article reports on the case of a prophylactic, needleless, robotic-assisted, transabdominal cerclage in a women with a triplet pregnancy and a history of recurrent cervical insufficiency with a prior failed transvaginal cerclage.
Case
A 33-year-old, gravida 6, para 0140 African-American woman presented with spontaneous conception of trichorionic–triamniotic triplets and an obstetric history notable for 3 prior second-trimester deliveries. Her previous pregnancy was managed with a transvaginal cerclage at 12 weeks' gestation that required placement of a second transvaginal cerclage at 16 weeks' gestation due to cervical dilation. Unfortunately, the patient presented at 21 weeks with preterm premature rupture of membranes for which voluntary interruption of the pregnancy was chosen. She additionally had 2 spontaneous abortions in the first trimester. She had no known risk factors for cervical insufficiency, such as prior surgical trauma to the cervix, obstetrical lacerations, or congenital anomalies.
Given her history of recurrent cervical insufficiency, this patient was seen by maternal–fetal medicine specialists to discuss prophylactic cerclage. The patient was informed that transvaginal or transabdominal cerclage were not recommended in multifetal pregnancies due to the paucity of supporting evidence. 5 Despite this, the patient was referred to the current authors' minimally invasive gynecology clinic at 10 weeks' gestational age to discuss robotic-assisted transabdominal cerclage. During her initial consultation, expectant management was recommended and that an interval prophylactic transabdominal cerclage would be indicated before her next conception. She was counseled that this specific procedure had not been documented in the literature in a triplet pregnancy. The feasibility of completing the transabdominal cerclage successfully was discussed, given her enlarged, multifetal gravid uterus. This patient's unique anatomical variations specific to her case were considered preoperatively, including size and weight of her uterus, inability to use a uterine manipulator, and increased uterine vasculature. Hemorrhage, rupture of membranes, and pregnancy loss were considered the major risks to surgery. Despite these precautions, a joint decision to proceed with robotic-assisted transabdominal cerclage was made.
The procedure was performed at 11 weeks' gestational age to overcome the anticipated anatomical challenges associated with a rapidly growing uterus. The surgery was performed under general anesthesia. A sponge-wrapped ring forceps in the vagina was used to delineate anterior and posterior anatomical borders. Pneumoperitoneum was achieved with CO2 insufflation via a Veress needle placed at the base of the umbilicus, after which a blunt 8-mm robotic trocar was inserted under direct visualization ∼3 cm cephalad to the umbilicus. Two bilateral lower-quadrant 8-mm robotic trocars were placed, and a third 12-mm accessory port was placed in the left midclavicular line between the supraumbilical and left lateral trocars. The patient was placed in a Trendelenburg position, the robot was docked, and visualization of the pelvic-floor landmarks—including the cervicovaginal junction, round ligaments, uterosacral ligaments, bilateral ureters, and bladder—was achieved. Robotic laparoscopes used included 8-mm 0° and 8-mm 30° scopes. Instruments used included robotic monopolar scissors, Maryland bipolar forceps, a robotic needle driver for grasping the Mersilene tape to secure the knots tightly, and an endo paddle retractor device, which was used to aid in visualization of anatomical landmarks around the enlarged uterus. Exchanging the 30° robotic scope orientation facilitated greater visualization around the gravid uterus.
The 30° robotic laparoscope was placed in a downward orientation and anterior broad ligament reflection was performed with short bursts of electrosurgery by monopolar scissors. This was performed with simultaneous cephalad pressure on the vaginal sponged instrument and gentle cephalad retraction of the uterus with the laparoscopic paddle using a “rolling” technique. The bladder peritoneum was displaced safely from the cervicovaginal junction, and the cervicouterine isthmus was identified with visualization of the uterine arteries bilaterally. To facilitate approximation of the cerclage tape directly at the level of the cervicouterine isthmus, a blunt tunneling technique was performed medial to the uterine arteries at this location. Using the same techniques, a posterior peritoneal reflection was created with monopolar scissors to permit visualization of the uterine arteries bilaterally. This was achieved using the 30° robotic laparoscope in an upward orientation and the laparoscopic paddle to elevate the gravid uterus cephalad and anterior gently. A similar tunneling technique was repeated bilaterally in an anterior direction.
This technique created an avascular tunnel, which was previously described by Mourad and Burke. 4 A 5-mm needleless Mersilene tape was passed circumferentially, using Maryland forceps at the cervicouterine isthmus medial to the uterine arteries. The tape was confirmed to be lying flat across the serosal surface without kinks or twists, and 5 square knots were placed in the posterior cul-de-sac (Fig. 1).
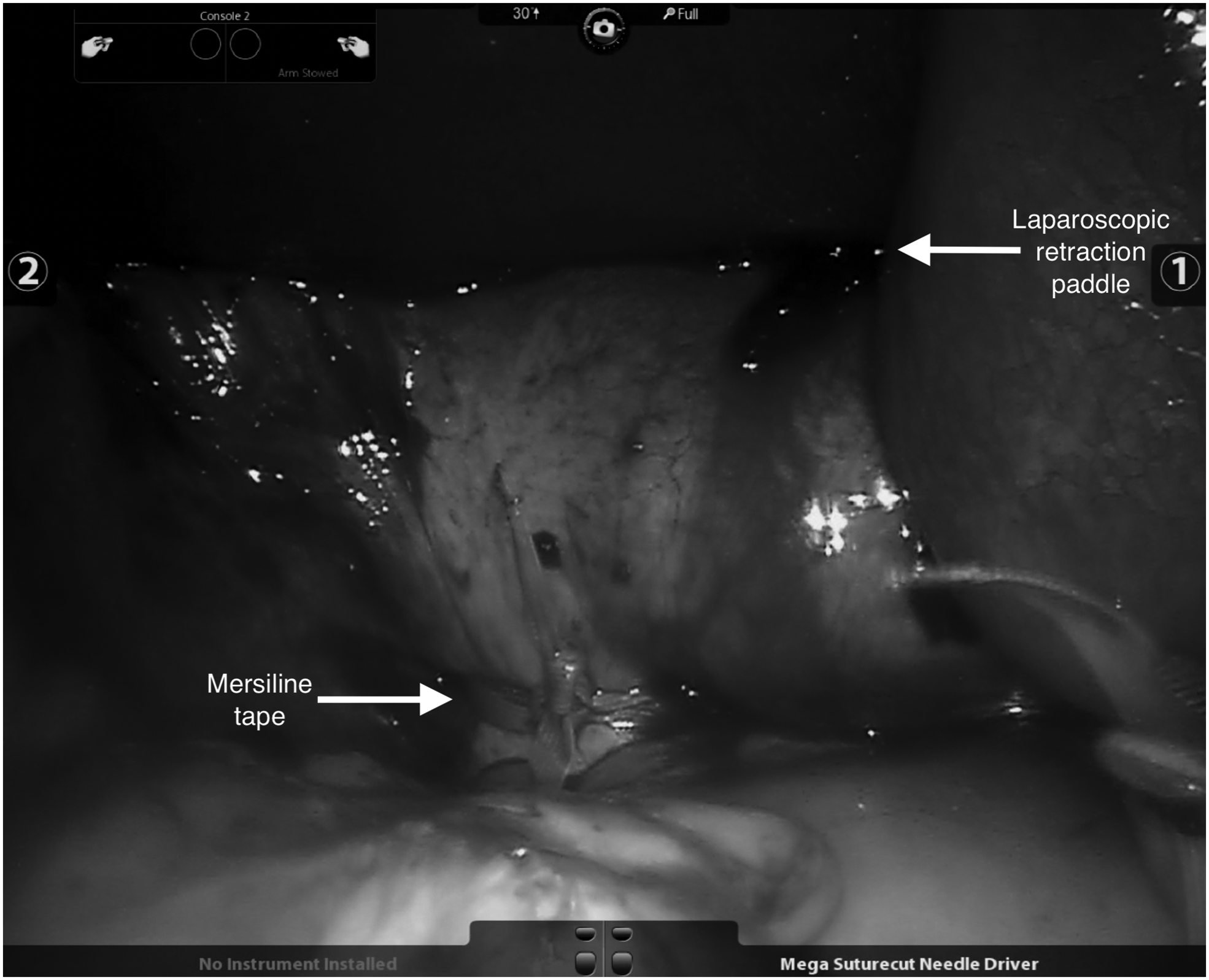
Transabdominal cerclage knot tied posteriorly using a laparoscopic paddle for retraction.
Results
The operative time was 2 hours and estimated blood loss was 50 mL. The patient was discharged home on the first postoperative day following fetal well-being seen on ultrasound (US). Follow-up included a 17-week transvaginal US, which showed a long and closed cervix with the cerclage tape at the level of the cervicouterine isthmus (Figs. 2 and 3). The remainder of the pregnancy was uneventful. The patient underwent a scheduled primary cesarean section at 35 weeks and 2 days. The transabdominal cerclage tape was identified easily at the cervicouterine isthmus and was removed without trauma or migration of the cerclage noted. Three healthy infants were delivered with weights of 2296 g, 2693 g, and 2778 g.
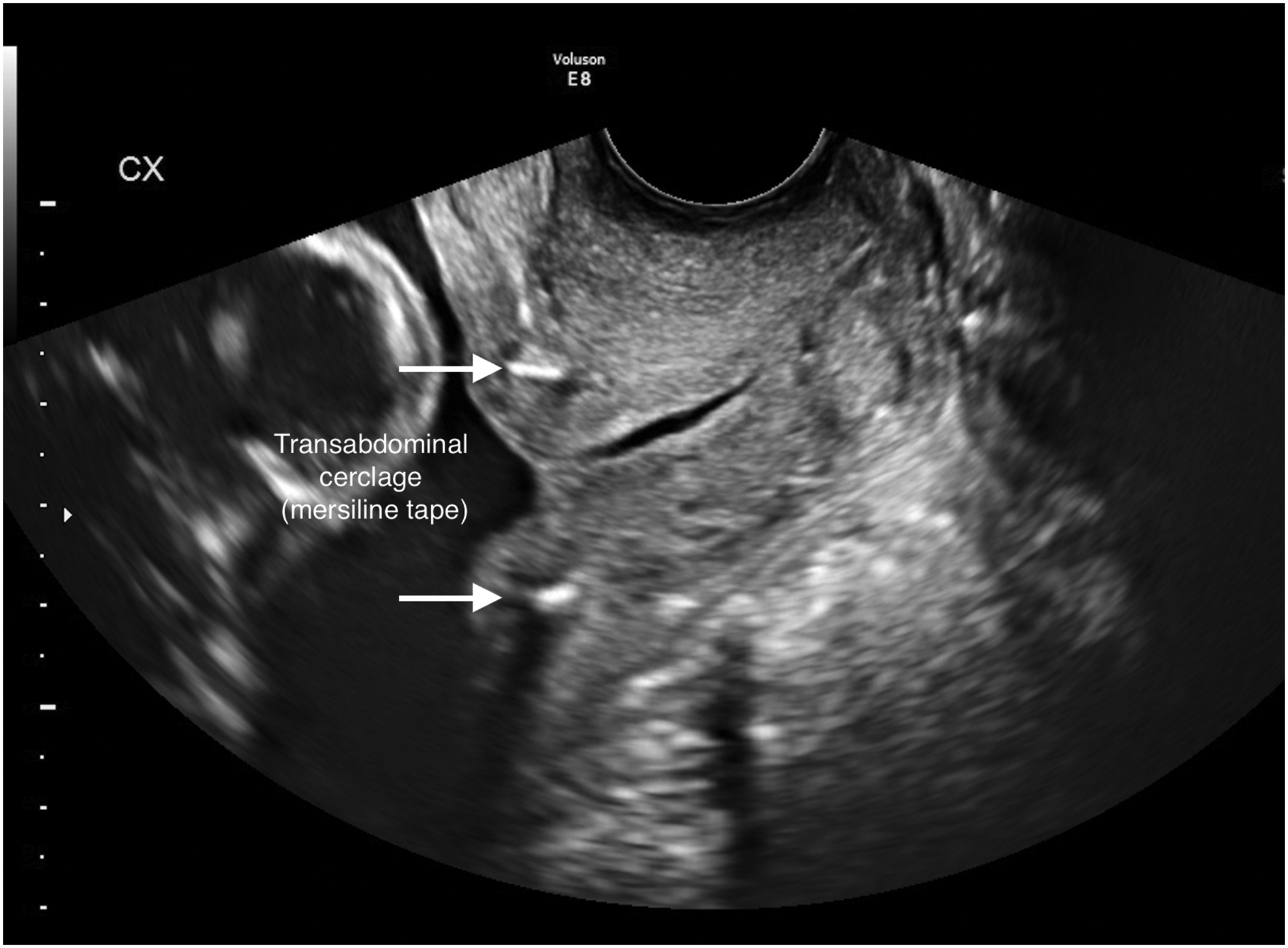
Transabdominal cerclage visualized on transvaginal ultrasound at 17 weeks' gestation. Image courtesy of John Elliott, MD.
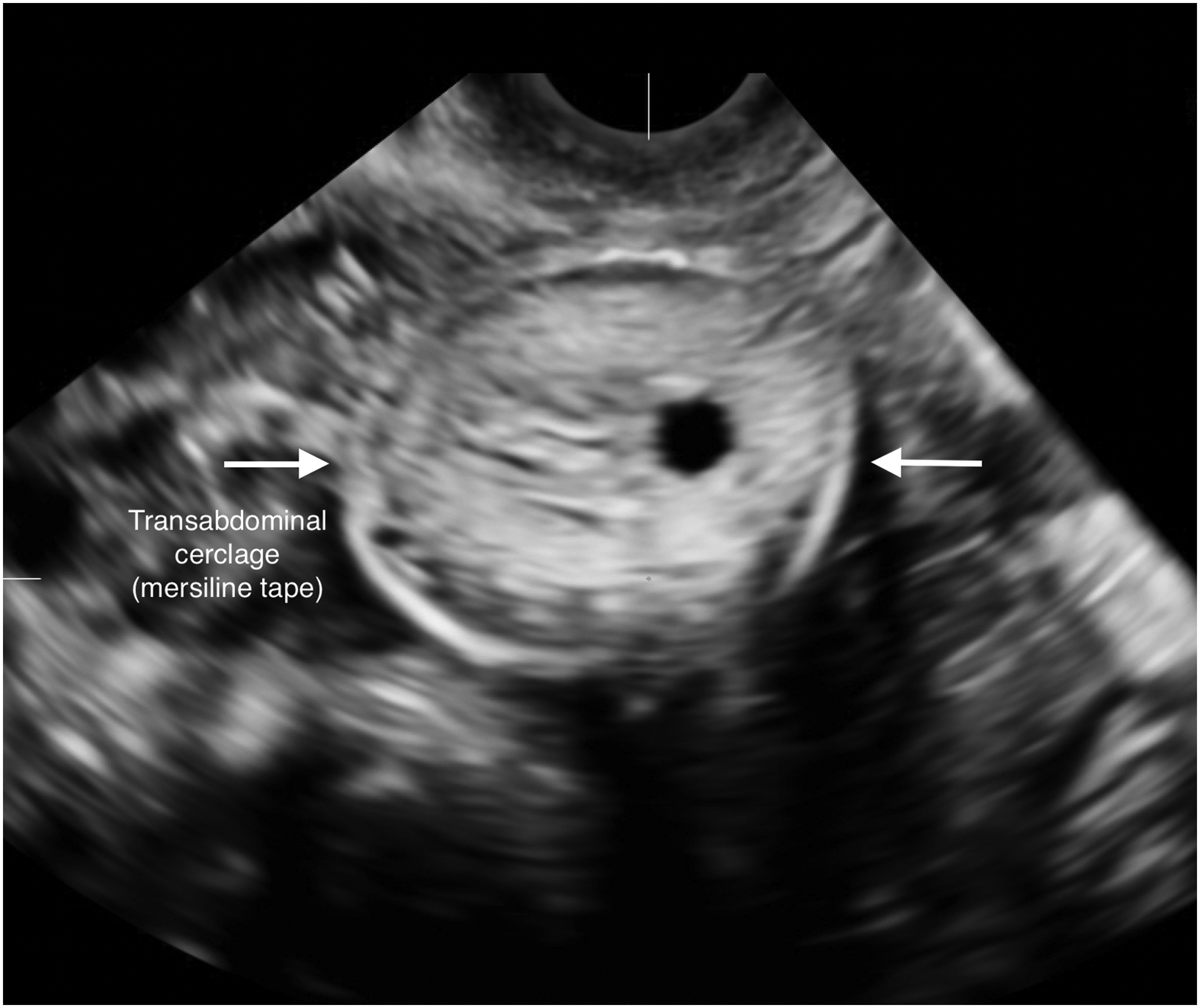
Transverse view of transabdominal cerclage at the level of the cervicouterine isthmus. Image courtesy of John Elliott, MD.
Discussion
Cervical insufficiency is one cause of preterm birth and is estimated to complicate 0.1%–1.0% of pregnancies. 8 The goal of treatment with cerclage for patients with cervical insufficiency is prevention of a subsequent preterm birth. Triplet pregnancies are at significantly higher risk for preterm birth, with a mean gestational age at delivery of 31.9 weeks. 9 Triplet and higher-order multiple-gestation pregnancies are rare, with estimates of only 153.5 per 100,000 births annually. 9 With this rare combination of cervical insufficiency in a triplet pregnancy, it is difficult to ascertain evidence-based recommendations for management.
The majority of published data regarding transabdominal cerclage for managing cervical insufficiency and prior failed transvaginal cerclage consists of information gathered from case reports/series, cohort studies, and systematic reviews. In 2011, Burger et al. published a comparison of the conventional laparotomy approach to those performed laparoscopically, but were unable to comment on superiority, given the limited number of patients and inconsistency of study methods. 8 A systematic review was published in 2018 by Moawad et al., which showed improved obstetric outcomes with the laparoscopic approach in conjunction with the known benefits of minimally invasive surgery. 3 These review articles did not include patients with multifetal-gestation pregnancies. Despite the limitations in research on this topic, successful outcomes in case reports such as this still prove valuable for optimizing management of these extreme cases.
The optimal timing for prophylactic transabdominal cerclage placement is preconception as an interval procedure, although preconception care is difficult to achieve, especially in high-risk populations. 10 To this end, surgeons are faced with a more-challenging transabdominal cerclage procedure, as a gravid patient has increased risks of hemorrhage, rupture of membranes, and pregnancy loss, compared to a patient undergoing an interval procedure. Helpful surgical techniques to navigate around a large gravid uterus are described in this current case report, such as the use of an accessory laparoscopic paddle and a 30° laparoscope. The “rolling” technique described with the laparoscopic paddle is performed by applying cephalad and posterior traction gently to the anterior aspect of the gravid uterus, and similarly applying cephalad and anterior traction to the posterior aspect of the gravid uterus. The authors believe that this technique permits greater visualization of the cervicouterine isthmus anteriorly and posteriorly around the multifetal-gestation uterus. Additionally, utilizing a needleless technique enables a more-precise placement of the cerclage tape within the created bilateral avascular tunnels. The current authors believe this technique can decrease the risk of hemorrhage in a patient with a highly vascularized gravid uterus.
Conclusions
To the current authors knowledge, this is the first reported robotic-assisted transabdominal cerclage in a triplet pregnancy. This case illustrates a successful obstetric outcome of triplets delivered more than 3 weeks after the average gestational age for triplets, and 14 weeks more than any of this patient's prior preterm deliveries. Prophylactic transabdominal cerclage, completed by an experienced surgeon via a robotic approach, is feasible in a triplet pregnancy in a patient with a history of cervical insufficiency. Improved pregnancy and/or neonatal outcomes cannot be determined by this case alone. Further studies are necessary to determine effectiveness, safety, and advisability for robotic-assisted transabdominal cerclage in higher-order multifetal gestations.
Footnotes
Acknowledgment
The authors thank John Elliott, MD, for the contribution of the US images in this report.
Author Disclosure Statement
No financial conflicts of interest exist.