
Abstract
Abstract
Background:
Uterine arteriovenous fistula (UAVF), a rare condition, usually occurs in females of reproductive age and is commonly diagnosed in those with histories of myometrial traumas. UAVF is generally associated with severe bleeding. Treatment choices are usually limited to selective embolization or hysterectomy; however, other treatment options—such as surgical occlusion of the pelvic vessels, and, less frequently, en bloc resection of the lesion adjacent to the surrounding myometrium with uterine reconstruction—have also been reported. This article presents a case of conservative surgical management (CSM) of the condition, with details about a simple surgical technique and a literature review on this topic.
Case:
A 25-year-old female (gravida 1, molar 1), with a history of curettage 11 months before consultation, presented with severe vaginal bleeding and severe anemia. UAVF was diagnosed based on findings of Doppler ultrasound and magnetic resonance angiography. This patient was managed with complete surgical resection of the UAVF and uterine reconstruction.
Results:
Remarkably, this patient had a spontaneous pregnancy 15 months' postoperatively.
Conclusions:
A review of the literature identified only 5 reports on CSM, with the most frequently used treatments being hysterectomy and arterial embolization for UAVF. The former method eliminates all possibilities of future pregnancies, whereas the latter has a high failure rate for the first attempt. In cases of UAVF in which fertility preservation is preferred and expectant management is not possible, surgical resection of the affected area followed by uterine reconstruction represents a valid option for health care centers with experienced interdisciplinary teams.
Introduction
Uterine arteriovenous fistula (UAVF) is a rare condition, but it is considered potentially life-threatening, owing to the possibility of causing severe hemorrhage.
Most cases of UAVF occur during the reproductive years of females, and almost all cases to date have been reported in females with histories of curettage, 1 cesarean section, or other types of trauma. Although UAVF is rare, with only 100 cases reported until 2011, 2 it can cause severe vaginal bleeding 3 and should be considered as a cause of late postpartum hemorrhage.
The differential diagnoses of UAVF includes retained products of conception, gestational trophoblastic disease, endometrial polyps, and vascular neoplasms, as well as all entities with localized increases of uterine vascularization and arteriovenous short circuits noted on ultrasound (US). 4 The diagnosis is made using Doppler US and must be differentiated from the diagnosis of retention of placental remnants because UAVF is associated with massive bleeding when endometrial curettage is performed. 5
Treatment is usually limited to selective embolization or hysterectomy, although en bloc resection adjacent to the surrounding myometrium and selective coagulation have also been described.
This article presents the case of a woman with surgically managed UAVF who underwent a complete surgical resection of the malformation followed by a spontaneous pregnancy. In addition, the article presents a literature review on this subject.
Case
A 25-year-old female was gravida 1, molar 1. This patient's molar pregnancy was treated with curettage, resulting in a loss of the ß-subunit of human chorionic gonadotropin (ß-hCG). Following postcurettage at 11 months, the patient reported severe vaginal bleeding that lasted for 2 weeks, and was hospitalized for testing and treatment.
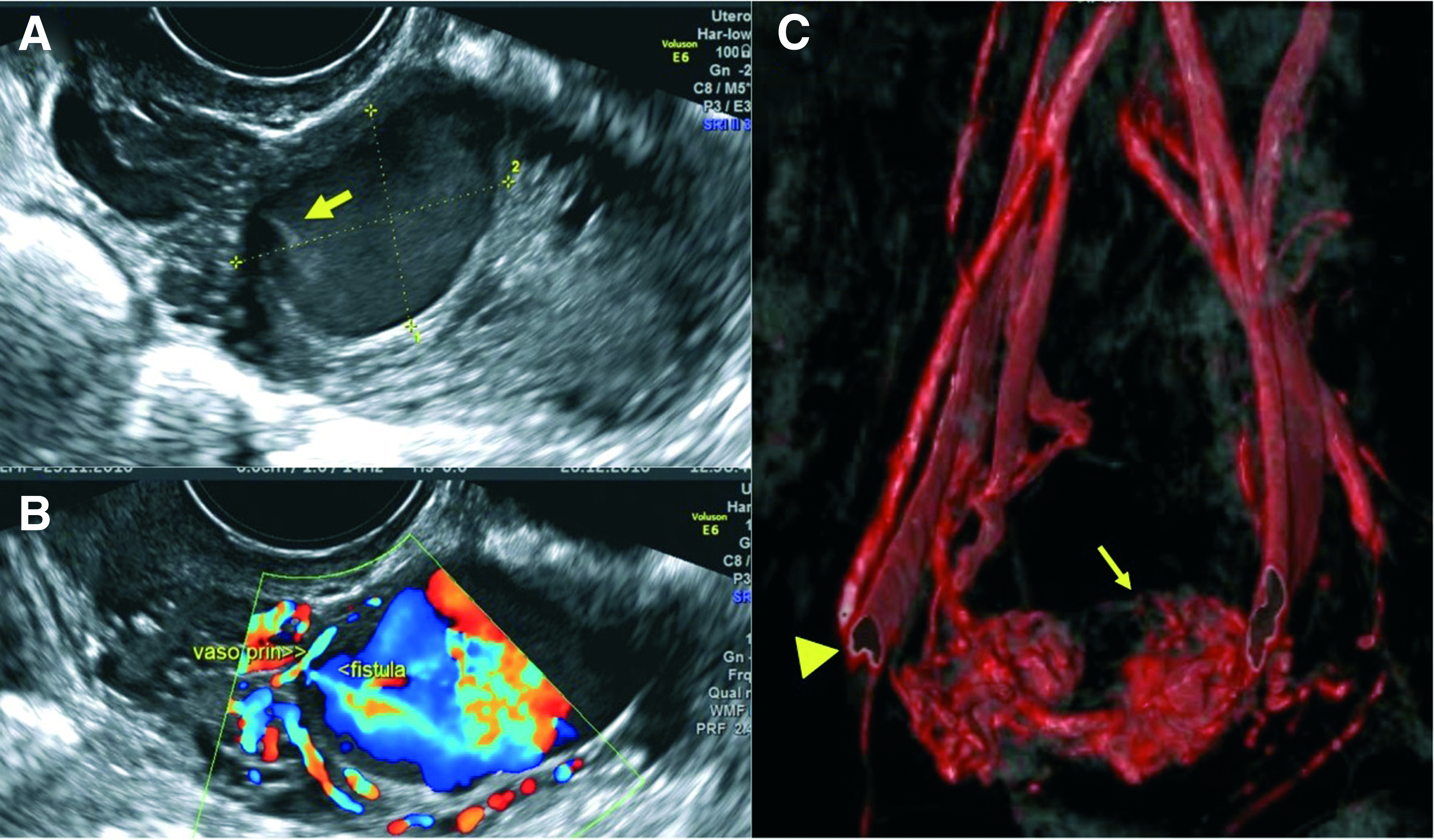
A US examination revealed a 23 × 28 mm intramyometrial mass located on the left uterine isthmus at a distance 2 mm from the endometrial cavity. The mass had an obvious flow detected by Doppler US and a jet flow corresponding to arterial flow (Fig. 1). Furthermore, magnetic resonance angiography revealed an intramyometrial vascular nest with multiple anastomoses between the branches of both uterine arteries and other branches corresponding to the collaterals of the internal iliac arteries. Based on these findings, UAVF was diagnosed, and the size of the mass indicated a high risk of rupture and the possibility of severe bleeding. Considering the large size of this mass and its multiple collaterals, the use of endovascular management was eliminated. On the patient's second hospitalization day, her vaginal bleeding increased and her hemoglobin level decreased from 9 dL to 7 g/dL. Accordingly, conservative treatment comprising surgical resection of the malformation was proposed, considering the patient's desire for fertility preservation. Upon completion of laparotomy, although the lesion was not evident on inspection, it was evident on palpation of the left side of the isthmus.
The following surgical steps were undertaken for the resection of the fistulous mass:
Wide dissection of the vesicouterine area to expose the entire uterine anterolateral surface of the uterus Identification of the UAVF on palpation and confirmation via US Vascular isolation of the malformation using hemostatic sutures in four quadrants (Figs. 2 and 3) Total resection of the UAVF and part of the surrounding myometrium Identification of the cervical canal and endometrial cavity, using a plastic catheter prior to performing uterine closure Hysterorrhaphy using separate square stitches (Figs. 2 and 4).
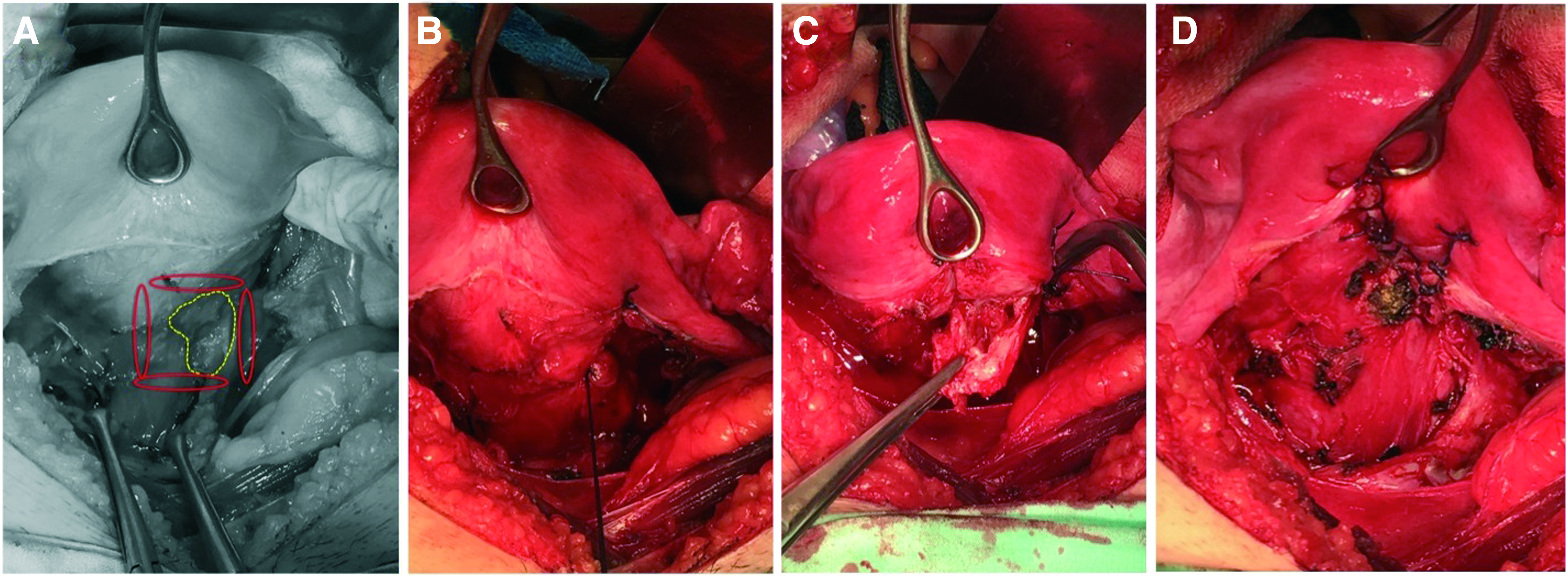
Anterior view of the uterus after dissection of the vesicouterine space.

Illustration of the hemostatic sutures' positions on the four quadrants, limiting vascular flow toward arterio (red) venous (blue) fistula. Color images are available online.

The patient's informed consent was obtained for this procedure.
Results
Intraoperative bleeding of 100 cc was estimated, and the total surgical time was 90 minutes, with no surgery-related complications. A subdermal implant was inserted as a contraceptive method for 14 months, and the patient was discharged on the second postoperative day. Follow-up US testing, performed at 3 weeks and at 14 months following discharge, revealed normal uterine vasculature. Similarly, follow-up hysterosalpingography and hysteroscopy revealed normal findings; hence, the subdermal implant was removed. One month later, the patient had a spontaneous pregnancy but had an incomplete abortion at 8 weeks, which was managed with vacuum curettage with no complications.
Discussion
A database search was conducted using PubMed, OVID, and SciELO for studies published between 1990 and 2017 using the terms
In 5 references, CSM was reportedly used (Table 1) for patients with histories of uterine traumas or gestational trophoblastic disease and who wished to achieve pregnancy in the future. In 2 cases, arterial embolization resulted in repeated failures. Furthermore, the affected area was resected in 1 patient because it was a gestational trophoblastic tumor. In 2 cases, the size and number of arterial anastomoses predicted a possible failure of pelvic vessel embolization (PVE). In fact, only 1 full-term pregnancy was reported following CSM. 6 In the other cases, hysterectomy was performed.
Previous Publications of Patients with UAVF Managed with Surgical Resection & Uterine Preservation (CSM)
CSM, conservative surgical management; hCG, human chorionic gonadotropin; IU, international units; D&C, dilatation and curettage; US, ultrasound; UAE, uterine arterial embolization; AVM, arteriovenous malformation; PVE, pelvic vessels embolization
Although hysterectomy represents definitive management, it implies the impossibility of future pregnancy. On the other hand, PVE requires a high level of specialization and involves risks, with possible complications such as those associated with arterial puncture and ovarian insufficiency. 7 PVE can also result in unwanted embolization with catastrophic consequences due to the passage of embolization materials into the kidneys, lungs, and brain. 8
PVE is a minimally invasive technique and usually facilitates the identification of the vessels involved, but recurrences are frequently reported. 9 The primary success rate of PVE is reportedly 61% 10 and is related to the surgeon's technique and experience, given that the uterus has a complex vascular supply 11 with additional supplying from the bladder and vaginal vessels, apart from those conventionally considered (uterine and gonadal vessels). This explains the inherent difficulty of endovascular management. 12
Some surgeons resort to surgical vascular ligation13–16 when confronted with repeated failures of PVE or when failure is predicted owing to an extensive network of arterial anastomoses; but hysterectomy is generally considered a preferred solution.
Therefore, the possibility of a second or third endovascular procedure is considered essential, along with additional therapeutic methods that facilitate fertility preservation. In this regard, few options are currently available. On the one hand, expectant management is another option for spontaneous regression; this approach is taken in up to 50% of cases, 17 particularly in cases of patients with asymptomatic UAVFs.18,19 Alternatively, it has been reported that use of the oral contraceptives methylergonovine, 20 danazol, 21 progesterone, or methotrexate 22 have led to the disappearance of these lesions. 23
The situation changes when a patient presents with active bleeding or hemodynamic instability, because expectant management is not feasible. In this case, the conventional option is hysterectomy even in centers with experience in UAVF management, 24 but CSM gains value if fertility preservation is preferred. This procedure, although not included in flow charts 25 and rarely reported in the literature (Table 1), is technically simple when the lesions are not very extensive (Fig. 3).
To date, only 5 reports of patients with UAVF undergoing CSM have been published (Table 1).6,26–29 The current patient had severe bleeding and severe anemia, requiring immediate intervention. The complexity of the arterial anastomoses related to the lesion (Fig. 1) eliminated the possibility of performing PVE for initial management, with surgical resection of the vascular lesion being performed successfully. As a hemostasis strategy, some researchers have performed arterial ligation prior to resection.6,26 The current authors' technique included placement of hemostatic sutures in four quadrants around the lesion (Fig. 3), enabling the achievement of hemostasis by resecting an ∼3-cm vascular nest (Figs. 2 and 4). Although this patient's lesion was relatively smaller than those reported previously, CSM has been reported to be useful against lesions of up to 5 cm. 26
Although this patient had a history of a molar pregnancy, her ß-hCG had become negative 10 months before the UAVF was identified, and histologic examination of the lesion, enabled by the primary use of PVE, eliminated the possibility of her having trophoblastic tissue. (Fig. 4). For cases in which positive chorionic gonadotropin is identified, a gestational trophoblastic tumor must be ruled out before intervention. 30
Following PVE for the management of UAVF, pregnancies have been reported in 53% of patients. 20 The results of patients following CSM have been reported rarely (Table 1), with only 1 reported full-term pregnancy 6 and the current case being the second one, although it resulted in an incomplete abortion at gestational 8 weeks.
Conclusions
Although the important role of interventional radiology and endovascular management of UAVF cannot be denied, its technical difficulty and possible complications must influence its inclusion among other management options. In selected cases of patients with the desire to preserve fertility, the need for definitive management—and without the option of conservative management—surgical resection of the affected area followed by uterine reconstruction represents a valid option at healthcare centers with experienced interdisciplinary teams.
Footnotes
Acknowledgment
The authors thank the Clinical Research Center of the Fundación Valle del Lili, Cali, Colombia, for the collaboration and advice during the work on this report.
Author Disclosure Statement
No financial conflicts of interest exist.