
Abstract
Abstract
Background:
Women with enlarged leiomyomatous uteri often have limited options for termination of pregnancy (TOP) and are referred to tertiary-care centers for management. This article presents a unique surgical approach to TOP in such women that has not been previously described in the literature.
Case:
A 35-year-old gravida 6, para 2032, at 9 weeks and 3 days of pregnancy, presented with a 30-week-sized leiomyomatous uterus displacing the pregnancy to the fundus with distortion of the cervix and endometrial cavity. This patient desired future fertility and declined medical management of her condition. She underwent a transfundal suction curettage via laparotomy at 13 weeks and 2 days of her pregnancy.
Results:
The patient's estimated blood loss was 300 cc. She had an uncomplicated postoperative course and underwent a myomectomy 12 weeks after a surgical abortion.
Conclusions:
A literature review revealed several case reports of medical management, and 1 reported use of an endotracheal tube for surgical termination. However, no other reports were found to guide surgical management in women with enlarged leiomyomatous uteri. When conventional suction curettage or dilation and extraction are not technically feasible in pregnant women, due to distortion of the cervix and endometrial cavity secondary to the leiomyomas, transfundal suction curettage via laparotomy may be considered. This approach is an alternative to medical management in women with enlarged leiomyomatous uteri who desire termination of their pregnancies.
Introduction
First- and second-trimester surgical termination of pregnancy (TOP), either by suction curettage (dilatation and curettage; D&C) or dilatation and evacuation (D&E), is effective and safe. 1 The presence of leiomyomas can make conventional surgical abortions technically impossible, due to constraints of instrument lengths and flexibilities. The literature is limited with respect to techniques for surgical abortion in these patients. This article discusses 1 case of surgical abortion in a woman with a large leiomyomatous uterus and an obstructed cervical canal, who declined medical management and desired future fertility.
Case
A 35-year-old, gravida 6, para 2032 patient presented at 9 weeks and 3 days of pregnancy for elective TOP. Her history included class III obesity (a body mass index of 41) and anemia with a history of a recent transfusion. She had had 2 spontaneous vaginal deliveries, 2 suction curettages for elective TOPs, and 1 spontaneous abortion. Examination revealed that the patient had a 30-week-sized irregular leiomyomatous uterus.
A sonogram showed a 9 weeks and 3 days' intrauterine pregnancy displaced into the right uterine fundus, 3–4 cm above the umbilicus. Magnetic resonance imaging was obtained to determine the path of the cervical canal from the cervical os to the gestational sac. The scan showed an intrauterine pregnancy displaced to the uterine fundus at 6 cm above the umbilicus (Fig. 1). The uterus measured 23 × 18 × 12 cm, and the distance between the cervix and the gestational sac was 19 cm with multiple sharp-angled curves. Access to the pregnancy vaginally was not feasible due to limitations in instrument lengths and distortion of the cervical canal. Surgical and medical options discussed with the patient included gravid hysterectomy, hysterotomy, and medical management with Laminaria spp. and misoprostol. She declined medical management and chose hysterotomy at 13 weeks and 2 days due to her desire for future fertility and the risk of failure of medical management.
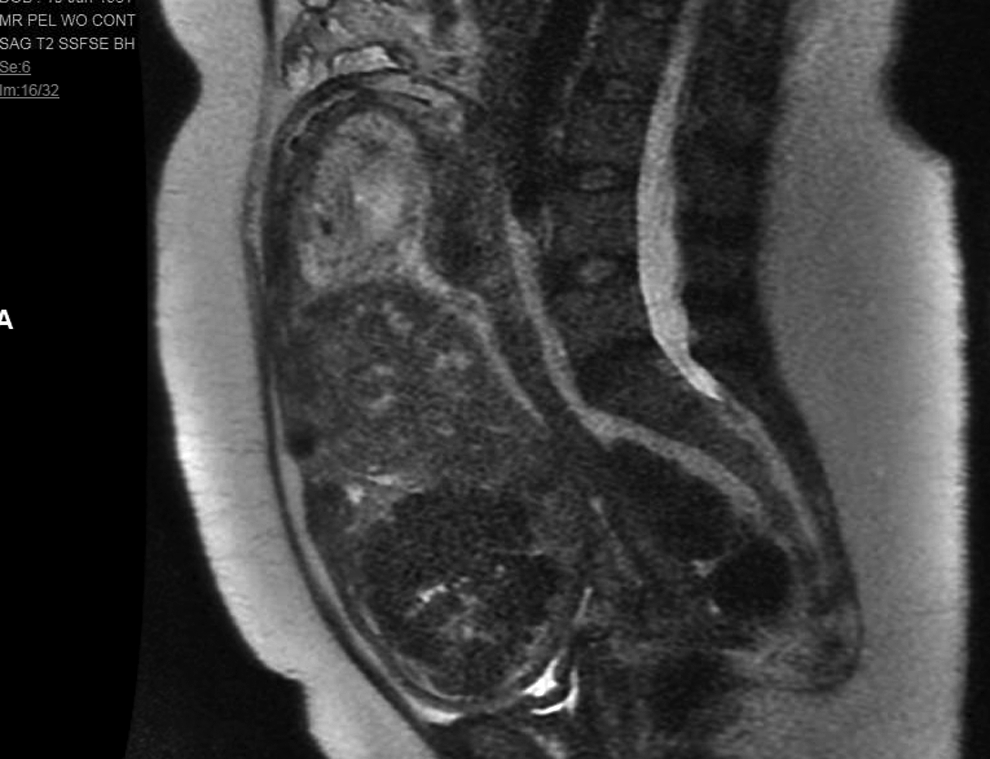
Magnetic resonance imaging showing multiple leiomyomas displacing 10 weeks' gestation to uterine fundus.
The patient's preoperative hemoglobin level was 9.2 g/dL. She underwent laparotomy via a midline vertical skin incision. Abdominal ultrasound (US) was performed to identify the shortest distance from the skin to the intrauterine sac prior to making the incision. After visualization of the uterus, the pregnancy was localized with ultrasonography of the uterus. Hysterotomy was performed in an area with a 2-cm thickness of myometrium and no leiomyomas. A spinal needle was inserted into the gestational sac under direct US guidance and filled with 60 mL of saline to confirm the location of the gestational sac and to distend the cavity. With the spinal needle still in place, a 1.5-cm stab incision was made in the myometrium with a scalpel. Suction curettage was performed under US guidance. Multiple passes were made with 16-mm-rigid, 12-mm-soft, and 8-mm-soft suction curettes until there was a gritty sensation and, on US, a thin endometrial stripe. No vaginal bleeding was noted. The hysterotomy was closed with a figure-of-8 stitch with an 0–chromic suture followed by an imbricating layer of a 1.0–chromic suture.
Results
The patient had an estimated blood loss of 300 cc and an uncomplicated postoperative course. She underwent a myomectomy 12 weeks after her surgical abortion.
Discussion
There have been few case reports describing surgical techniques for TOP in women with leiomyomas for whom traditional D&C and D&E were technically impossible. In the current case, TOP was performed by laparotomy and abdominal suction curettage under direct US guidance. To the current authors' knowledge, hysterotomy with abdominal suction curettage for TOP in these patients was been previously described once, utilizing laparoscopy for abdominal suction curettage after failed medical TOP. 2 Prior case reports also describe using endotracheal tubing or a flexible cannula in place of a standard suction curette to obtain increased length and improve access in patients with obstructing leiomyomas.3,4 Although using unconventional tools for the termination were considered, the current authors did not offer this as an option to the patient due to the location and number of fibroids, as well as the increased risk for uterine perforation, hemorrhage, and possible need for hysterectomy. In this case, the patient's anemia, and desire for future fertility, this procedure was deemed most appropriate for minimizing risk of the uncontrolled bleeding necessitating hysterectomy.
Conclusions
Suction curettage via hysterotomy allows localization of the gestational sac in the setting of multiple leiomyomas while reducing the risk of uncontrolled bleeding. The current authors recommend that this technique only be used when access through the cervix is impossible and the risk of failure and complications using other techniques are unsuitable for a patient. The disadvantages of this procedure include the morbidity associated with laparotomy and longer recovery time compared to conventional methods for TOP and the possible need for future cesarean delivery.
Footnotes
Acknowledgment
Written consent was obtained from the patient for publication of this case report and accompanying figure.
Author Disclosure Statement
No competing financial conflicts exist.