
Abstract
Abstract
Background:
Endometrial stromal sarcoma (ESS) is a rare tumor. Extension into the inferior vena cava (IVC) and heart has been described infrequently.
Case:
A 35-year-old female had low-grade ESS with intracardiac extension. A multidisciplinary team performed laparotomy, hysterectomy, and thoracotomy to obtain access to her intracardiac thrombus and, then, removal of the thrombus in her IVC.
Results:
This successful multidisciplinary team management produced a favorable outcome. This patient is currently being maintained on adjuvant hormonal therapy with 1 mg/day of anastrozole (an aromatase inhibitor to prevent conversion of androgen to estrogen).
Conclusions
: ESS is a rare tumor with intracaval and intracardiac extension. Diagnosis is usually made through histopathology. A multidisciplinary approach is required for optimal management.
Introduction
Uterine cancer is the fifth most common cancer in women (∼48% of all cancers in women) with a cumulative risk of 1% developing this disease by age 751 Uterine cancer includes endometrial carcinomas (85%–90%) and uterine sarcomas (2 to 5%). 1
Endometrial stromal sarcoma (ESS) is a rare tumor that comprises up to 0.2% of all uterine malignancies and ∼10% of all uterine sarcomas. 2
Tumor tissue originating from uterine pathology and extending into the inferior vena cava (IVC) is very rare and has been observed with leiomyoma (∼200 reported cases) and with ESS (∼26 reported cases). 3 Only a few cases with an intracardiac extension of the tumor thrombus in the IVC have been reported.4–6 However, it has also been mentioned that more than 50% of intravenous low-grade ESS cases could include intracardiac extensions. 7 Women with ESS or intravenous leiomyomatosis can present with a tumor thrombus in the IVC—and it is not possible to distinguish between these two conditions on the basis of imaging; the diagnosis is made after histopathologic examination of excised specimens.
This article reports on a young woman with low-grade ESS with a tumor thrombus in the IVC and intracardiac extension into the right atrium.
Case
A 35-year-old woman with no significant past medical history presented to a gynecology department with heavy menstrual bleeding and a sensation of heaviness in her lower abdomen for 5–6 months. Her prolonged bleeding lasted for 7–10 days at intervals of 15–20 days. Her previous menstrual cycles had been regular, with bleeding for 3–5 days each month. She was para 2, with 2 normal vaginal deliveries, and with 2 daughters, ages 18 and 14.
She had undergone a pelvic ultrasound (US) 5 months prior, which was said to show normal results, but the report was not available. As her symptoms worsened gradually, she underwent another abdominopelvic US followed by contrast-enhanced computed tomography (CECT) at a private clinic a week prior to the current presentation. These scans revealed a predominantly solid mass with a cystic area arising from the right posterolateral wall of the uterus measuring 11.6 × 6.4 cm, likely to be a broad-ligament fibroid with cystic degeneration. The right adenexa was not visualized separately, the left ovary was normal, and there was no free fluid. A thrombus was present in the IVC, extending from its bifurcation up to the chest.
Her last menstrual period had been 20 days prior. Her weight was 45 kg, her hemoglobin level was 10 g/dL, her blood pressure was 110/70 mm Hg, her pulse rate was 88 beats per minute, and her respiratory rate was 16 breaths per minute. A chest examination revealed bilateral vesicular breathing with no added sounds. A cardiovascular examination revealed normal heart sounds with no murmur. She did not have any lymphadenopathy or edema of the lower limbs.
Abdominal examination revealed a pelvic mass of ∼16 weeks' pregnant uterus size. There was no free fluid or organomegaly. Speculum examination revealed that her cervix and vagina looked normal. On bimanual examination, the pelvic mass appeared to be continuous with the uterus. The uterine body and fundus were deviated toward the left side due to a right-sided mass in the region of the broad ligament. She was admitted to the hospital, and, based on the findings of an IVC thrombus, she was started on 40 mg of injected enoxaparin subcutaneously twice per day.
An US after admission showed similar findings and an endometrial thickness of 7 mm. Doppler US of her lower limbs revealed no evidence of deep-vein thrombosis. CECT of the chest, abdomen, and pelvis (Fig. 1) was performed. This revealed a heterogeneous mass with cystic areas, measuring 14 × 9.1 × 11 cm, arising from the uterus, predominantly on the right side.
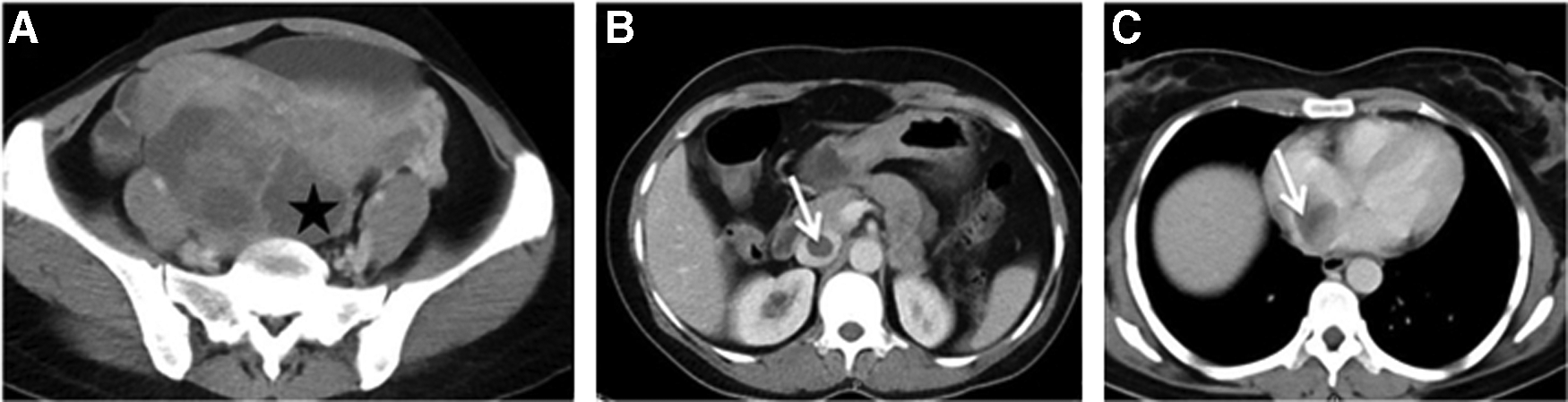
Axial contrast-enhanced computed tomography images showing a heterogeneous mass in the uterus with
The mass was infiltrating into the myometrium. The right ovary could not be seen separately, the left ovary was normal, and there was no free fluid. A hypodense filling defect was observed in the right common iliac vein, the IVC, and extending into the right atrium. Due to these findings, the possibilities of uterine sarcoma or leiomyoma with intravenous leiomyomatosis were considered.
An US-guided percutaneous core-biopsy from the pelvic mass showed spindles arranged diffusely and in short fascicles with oval-to-elongated nuclei. The cells showed fine granular chromatin, inconspicuous nuclei, and scant neoplasm with indistinct cell borders. Immunohistochemistry (IHC) showed negative cell development (CD)–117, negative S-100, membranous ß-catenin, and 5% Ki-67. These findings suggested a smooth-muscle neoplasm.
With a probable diagnosis of a smooth-muscle tumor of the uterus with intravenous extension, the patient was scheduled for laparotomy, hysterectomy, and thoracotomy to obtain access to her intracardiac thrombus and, then, removal of the IVC thrombus. A multidisciplinary team performed the surgery in a cardiac operation theater with a facility for performing a cardiopulmonary bypass. Laparotomy revealed a large predominantly solid mass arising from the uterus extending into the right broad ligament and reaching up to the right pelvic wall, with peritoneal adhesions to the lateral pelvic wall. The right ovary and fallopian tube were indistinguishable from this mass, and the left ovary and fallopian tube appeared normal. Total abdominal hysterectomy with bilateral salpingo-oophorectomy were performed. This was followed by a thoracotomy, and the cardiac surgeon achieved resection of the intracardiac mass by a right atriotomy. Next, the vascular surgeon performed an IVC thrombectomy to remove a 26-cm long tumor thrombus extending from the right common iliac vein up to the right atrium (Fig. 2).

Gross specimen of the resected uterus
This patient's peritoneal cytology was negative. Histopathology testing (Fig. 3) showed a uterine tumor reaching with tongue-like infiltrating margins and cells that were ovoid with coarse chromatin and scanty cytoplasm, with mitosis >5/10 high-power fields. On IHC, there was strong positivity for CD-10, and this was consistent with low-grade ESS. A strong positivity for progesterone receptors was seen. Both ovaries and the left fallopian tube were normal; the right fallopian tube had tumor emboli on the serosa. The IVC thrombus showed a tumor of similar morphology. Her final diagnosis was low-grade ESS.
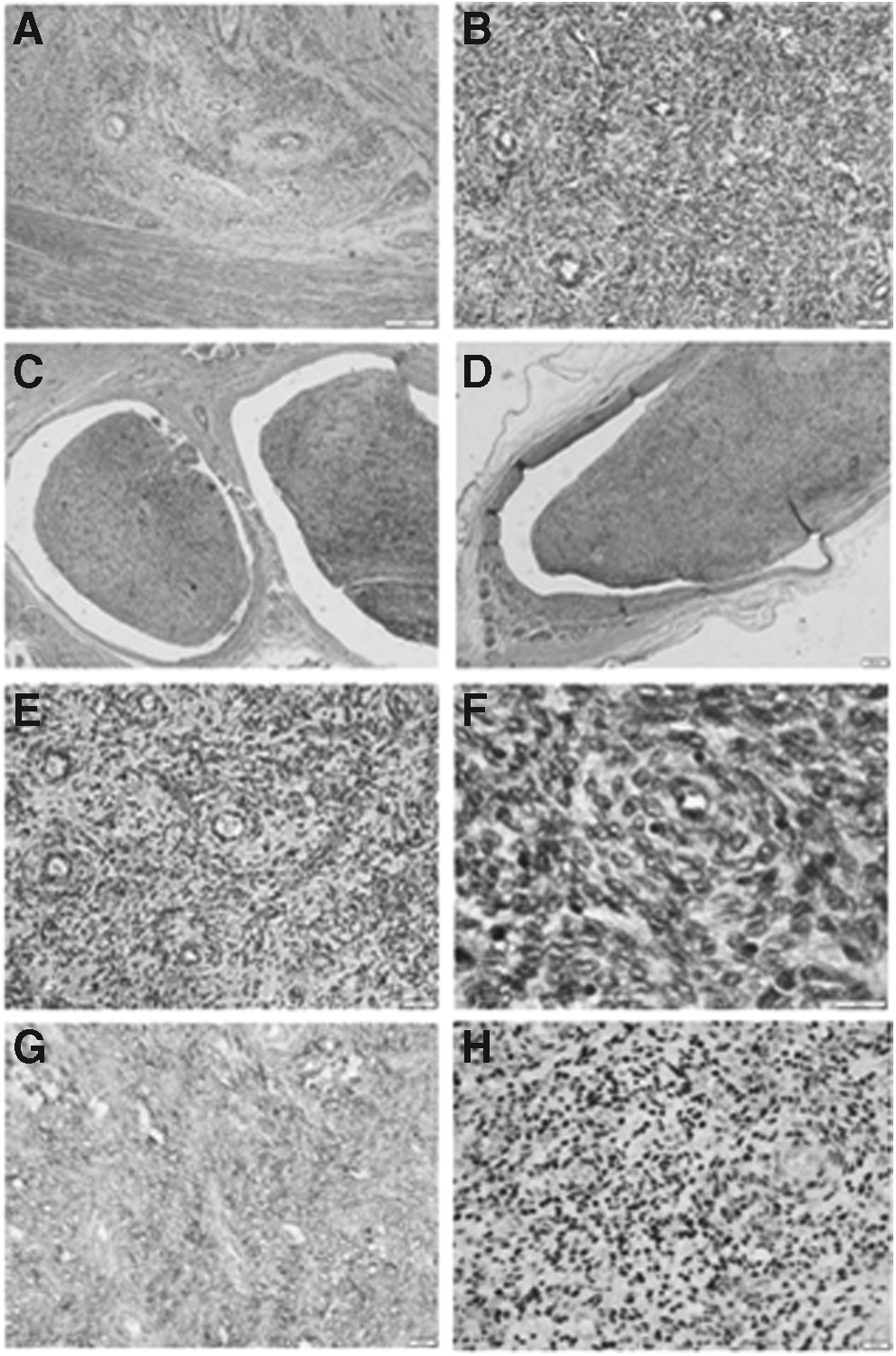
Low-grade endometrial stromal sarcoma.
Results
Postoperatively, this patient recovered well with no morbidity. Enoxaparine was continued and was changed to Acitrom® tablets after 3 weeks. She was started on adjuvant hormonal therapy with 1 mg/day of anastrozole (an aromatase inhibitor to prevent conversion of androgen to estrogen), which she was continuing to take as of this writing. CECT of her chest, abdomen, and pelvis 1 month after surgery showed normal results. As of this writing, she was 5 months postoperative and well.
Discussion
ESS comprises ∼0.2%–1% of all uterine malignancies, with an annual incidence of ∼2 per 1,000,000 women. 2 ESS is often mistaken for a leiomyoma via a clinical diagnosis, and a final correct diagnosis is made postoperatively. Histopathologic diagnosis in a case of early low-grade ESS may be mistaken in up to 40% of cases, which can result in treatment delays. 8 ESS is classified as low-grade (fewer than 10 mitotic figures) or high-grade (more than 10 mitotic figures). Five-year survival rates of low-grade ESS are 80%–100% and high-grade ESS are 25%–55%. 6 The World Health Organization classification (2003) divided ESS into low-grade and undifferentiated ESS based on infiltration and morphology. 9 ESS has a tendency to spread through the venous system with infrequent involvement of the IVC and, even more rarely, intracardiac extension. About 26 cases have been reported with IVC or intracardiac tumor extension. 3 In some cases, preoperative CECT is not able to detect an intravascular extension that is free floating and, hence, multiple imaging methods such as magnetic resonance imaging and US may be utilized for adequate surgical planning and resection. 4
It is often difficult to differentiate low-grade ESS from leiomyoma, and a false diagnosis could be reported even after postoperative histopathologic examination. 10 The differentiation is important for proper management, as low-grade ESS is a malignant disease. Gross examination shows that both tumors are well-circumscribed; however, ESS is soft, rubbery, and yellowish in contrast to the firmness and whitish color of a leiomyoma. Both tumors show a wormlike projection into the vascular channels with possible extension to the IVC or heart; this projection can be peeled off easily from the endothelial lining of the blood vessels.11,12 One distinction might be that ESS (and not intravascular leiomyomatosis) might infiltrate surrounding tissues.11,13 This was observed intraoperatively in the current case, as the ovary and tube were incorporated into the tumor, and it was adherent to the lateral pelvic wall. Finally, an appropriate diagnosis is made by histopathology along with IHC, including markers such as CD-10 and ß-catenin. 14
Conclusions
Adequate management of ESS requires an approach that includes preoperative planning and a multidisciplinary team. With extensive radical surgery, a recurrence-free survival prognosis can be improved. For complete resection, appropriate anatomical exposure and vascular access are required; a full sternolaparotomy needs to be performed. Intracardiac extension can require a cardiopulmonary bypass for safe removal of a tumor thrombus. 6 Long-term survival in these patients is most importantly determined by a free resection margin. 15
For prevention of recurrences, adjuvant hormonal therapy—with progestins, aromatase inhibitors, and gonadotropin-releasing–hormone analogues—after surgical resection is suggested. No standard guidelines for adjuvant radio- and chemotherapy have yet been suggested for ESS management. 15
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.