
Abstract
Abstract
Background:
Interstitial pregnancy is a rare variant of tubal ectopic pregnancy that carries a risk of life-threatening hemorrhage.
Case:
A gravida 4, parity 2, female, with 1 previous abortion, presented at 8 weeks of pregnancy. She was experiencing dizziness, pain in her abdomen, and vaginal bleeding. A transvaginal scan was suggestive of a left-sided, ruptured ectopic pregnancy that was probably an interstitial pregnancy. The patient underwent emergency surgery. On laparoscopy, her condition was shown to be an interstitial pregnancy. The surgery was converted to laparotomy because of her hemodynamic instability. Cornual resection with ipsilateral salpingectomy were performed.
Results:
The patient was discharged on postoperative day 4. Histopathology testing confirmed that she had a left, interstitial, tubal ectopic pregnancy.
Conclusions:
Early diagnosis is a key element in appropriate management. Medical and conservative surgical methods are safe and effective. Selection of a treatment option must be individualized and based upon proper patient counseling, clinical presentation, hemodynamic status, future pregnancy desires, and surgeon expertise.
Introduction
All ectopic gestations are known for their potential risk of hemorrhage but interstitial ectopic pregnancy is associated with massive life-threatening hemorrhage. Interstitial pregnancy is an ectopic gestation that is implanted in the tubal segment traversing the muscular wall of the uterus. This kind of pregnancy accounts for 2%–4% of all tubal pregnancies, with a higher maternal mortality rate of 2%–2.5%. 1 This portion of the fallopian tube is relatively thicker than the rest of the tube and is highly vascular, as uterine and ovarian artery anastomoses at the cornua; hence, this leads to severe hemorrhage when an interstitial pregnancy ruptures. The diagnosis of interstitial pregnancy is difficult to make and is often missed. The eccentric location of the gestational sac and the very thin myometrium layer makes it difficult to differentiate among interstitial, corneal, and eccentric intrauterine angular pregnancies. Conventional treatment includes cornual resection by laparotomy. However, within the last 2 decades, medical management and laparoscopic conservative surgeries have been reported with successful outcomes. Although the literature has several case reports highlighting different treatment strategies, there are few studies that discuss all management options for interstitial pregnancy.
Case
A 33-year-old female, gravida 4, parity 2, with 1 previous abortion, presented at 8 weeks of gestation presented with acute pain her abdomen, vaginal bleeding, and dizziness. There was a history of an attempted induced medical abortion by the patient herself for a presumed intrauterine pregnancy. At presentation, she had severe pallor, a pulse rate of 120 beats per minute, and a blood pressure of 90/60 mmHg. Abdominal examination revealed tenderness in the left iliac fossa. Vaginal examination was suggestive of cervical motion tenderness and fullness in the posterior fornix. Transvaginal ultrasound (TVUS) of this patient showed an empty uterine cavity, and a gestation sac in the left cornua of the uterus with a crown–rump length of 1.8 cm and excessive free fluid in the pelvis. In view of this clinical and radiologic assessment, the diagnosis of a left, corneal, ruptured ectopic pregnancy was made.
After proper counseling and informed consent, emergency laparoscopic surgery was performed. On laparoscopy, ∼1.5 L of hemoperitoneum was seen with the ruptured left interstitial ectopic pregnancy. The uterus was normal in size with a gestational sac in the left interstitial tubal part. The right fallopian tube and ovary appeared to be healthy. Due to some electrocardiographic changes intraoperatively and the deteriorating hemodynamic condition of this patient, her surgery was converted to a laparotomy. Left salpingectomy and cornual resection were performed, (Figs. 1 and 2), and optimum hemostasis was achieved. Right tubal ligation was also performed in view of this patient's completed family and according to her wish. She received 3 units of blood transfusion in the intraoperative period and remained stable throughout the postoperative period.
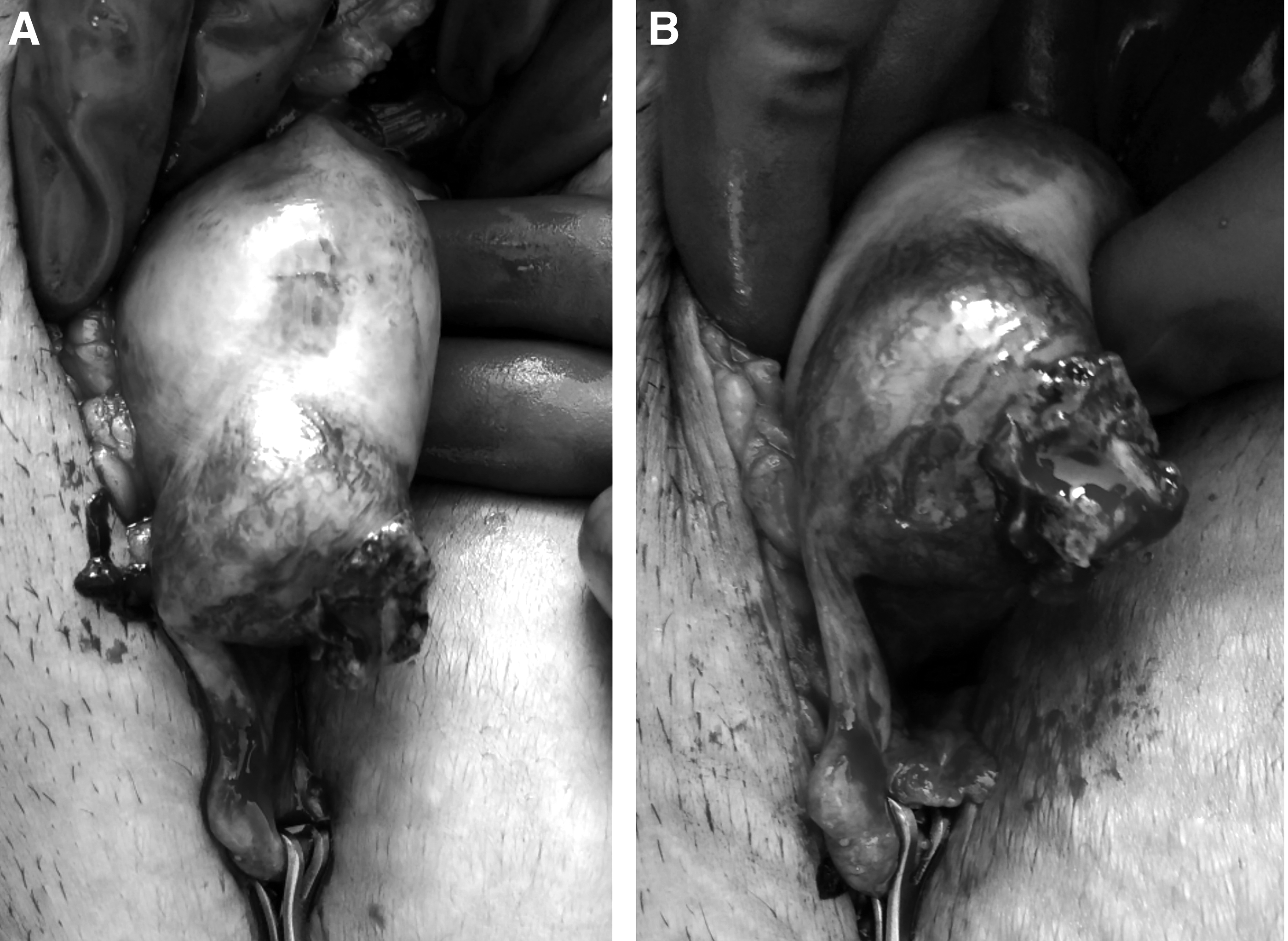

Resected fallopian tube with product of conception in the interstitial part.
Results
The patient was discharged on the fourth postoperative day. Histopathology testing confirmed the diagnosis of a left, interstitial, tubal ectopic pregnancy.
Discussion
Interstitial pregnancy is considered more dangerous than other tubal ectopic pregnancies because this region of the fallopian tube is thick, vascular, and more distensible due to its surrounding myometrium. Hence, an ectopic pregnancy is more likely to advance and rupture in later gestation. The rupture of an interstitial pregnancy leads to severe hemorrhage in almost one-fourth of cases, and there is a relatively high maternal mortality rate. 1
Diagnosis and management of interstitial pregnancy are challenging and require expertise. A high index of suspicion is needed. The principal diagnostic tools are ß-human chorionic gonadotropin (ß-hCG) level testing and TVUS. Due to an interstitial pregnancy's location, it can be confused with an angular pregnancy or a cornual pregnancy (a normal intrauterine pregnancy in an anomalous uterus, which is bicornuate, septate or unicornuate). Ultrasound (US) features of an interstitial, tubal ectopic pregnancy include an empty uterine cavity, a separate gestational sac more than 1 cm from the most lateral edge of the uterine cavity, and a thin myometrial layer (5 mm) surrounding the gestational sac. 2 These criteria are relatively specific (90%) for interstitial pregnancy but only have a 40% sensitivity. Another sign on US that has higher sensitivity (80%) and specificity (98%) is an interstitial line sign, which is a thin echogenic line extending directly up to the center of the chorionic sac. 3
Early diagnosis of interstitial pregnancy is crucial, as it allows surgeons to choose conservative management options, which include medical or conservative surgical methods. Diagnosis made in later gestation mostly calls for surgical treatment with cornual resection and even might require hysterectomy. Medical treatment with systemic or local injection of methotrexate is safe and effective in patients with unruptured smaller ectopic pregnancies, in which patients have low-serum ß-hCG and stable hemodynamics.1,4 Surgical treatment includes laparotomic, laparoscopic, or hysteroscopic approaches. The laparoscopic techniques include cornuostomy, cornual resection and salpingectomy, use of an ENDOLOOP,® and an encircling method. 5 In cornuostomy the ectopic gestation is removed without removing the surrounding myometrium, whereas in cornual resection, removal of the interstitial part of the fallopian tube along with the surrounding myometrium is performed. Cornuostomy is appropriate for gestation of sizes less than 3.5 cm, whereas cornual excision is recommended for gestation sizes of more than 4 cm. 1 The ENDOLOOP method and encircling suture around the cornua were reported to be safe and effective in a retrospective study by Moon et al. 6 Injection of diluted vasopressin below the interstitial pregnancy is also used to achieve hemostasis during laparoscopic surgery. 7
An hysteroscopic approach has also been reported in few cases, with successful outcomes, for managing cornual pregnancies. 8 Minelli et al. suggested that, under laparoscopic control, hysteroscopic resection of the cornual endometrium along with the tubal ostium can be performed without perforation of the uterus. 9 Thus, endoscopic management of interstitial pregnancy allows conservative fertility-sparing surgery with less postoperative pain, faster recovery, and a shorter hospital stay. Although medical method and endoscopy have emerged with successful outcomes for managing interstitial pregnancy, this has a potential risk of persistent ectopic pregnancies and recurrences in later pregnancies on the same side. Cornual resection is associated with decreased fertility and risk of uterine rupture at the interstitial portion of the tube in future pregnancies. 10 Elective cesarean section should be planned for later pregnancies. Future fertility concerns and mode of delivery in the next pregnancy should be explained at the time of counseling to choose a correct management option for a particular patient. Conservative treatment is preferred to preserve fertility, provided the patient is hemodynamically stable.
Conclusions
Interstitial pregnancy is a rare variant of a tubal ectopic pregnancy. This kind of ectopic pregnancy carries a risk of life threatening hemorrhage. Early diagnosis is a key element that contributes toward appropriate management. Medical and conservative surgical methods are safe and effective. Selection of a treatment option must be individualized and based upon proper patient counseling, clinical presentation, hemodynamic status, future pregnancy desires, and the surgeon's expertise.
Footnotes
Author Disclosure Statement
No financial conflicts exist.