
Abstract
Abstract
Background:
Gliomatosis peritonei is a rare condition characterized by the presence of implants of mature glial tissue throughout the peritoneum. According to the World Health Organization grading system for immature teratomas, gliomatosis peritonei is assigned to grade 0. Intraoperatively, gliomatosis peritonei is seen as multiple, tiny, well-circumscribed, gray–white peritoneal nodules. Clinicoradiologically, the condition is often misdiagnosed as peritoneal carcinomatosis or peritoneal tuberculosis.
Case:
This article reports on a case of gliomatosis peritonei with an immature teratoma in a 7-year-old girl, who presented with abdominal pain of 1 month's duration. The diagnosis was established after resection of this left adnexal mass along with an omentectomy. Confirmation was established with the help of immunohistochemistry testing.
Results:
The patient was relieved of her abdominal pain and is being followed-up regularly.
Conclusions:
A definitive diagnosis requires histopathologic examination and positive immunohistochemical staining with neural markers. A thorough search for the presence of immature neuroepithelial tissue is imperative in such cases to exclude the possibility of a metastatic immature teratoma.
Introduction
Gliomatosis peritonei is a rare condition characterized by presence of islands or implants of mature glial tissue throughout the peritoneum. The condition is most often seen in association with immature teratomas and, occasionally, in patients who have ventriculoperitoneal shunting. 1 According to the World Health Organization (WHO) grading system for immature teratomas, gliomatosis peritonei is regarded as a grade 0 immature teratoma.1,2 A definite diagnosis can be established by histopathologic examination and immunohistochemical confirmation. Additionally, thorough sampling to exclude the presence of immature neuroepithelial tissue should be performed to exclude the possibility of a metastatic immature teratoma. Irrespective of the extent of spreading, the condition has a favorable prognosis, and malignant transformation leading to development of gliomas has been noted only in exceptional cases.
Case
A 7-year-old girl presented with lower abdominal pain for a duration of 1 month prior to presentation. A physical examination revealed that she had a firm palpable mass in the left lower quadrant of her abdomen. Ultrasonography and computerized tomography scanning revealed a 15 × 11–cm, heterogeneous solid–cystic mass in the left adnexa. An exploratory laparotomy revealed a large solid–cystic mass involving the left ovary. The patient underwent resection of this left adnexal mass along with an omentectomy.
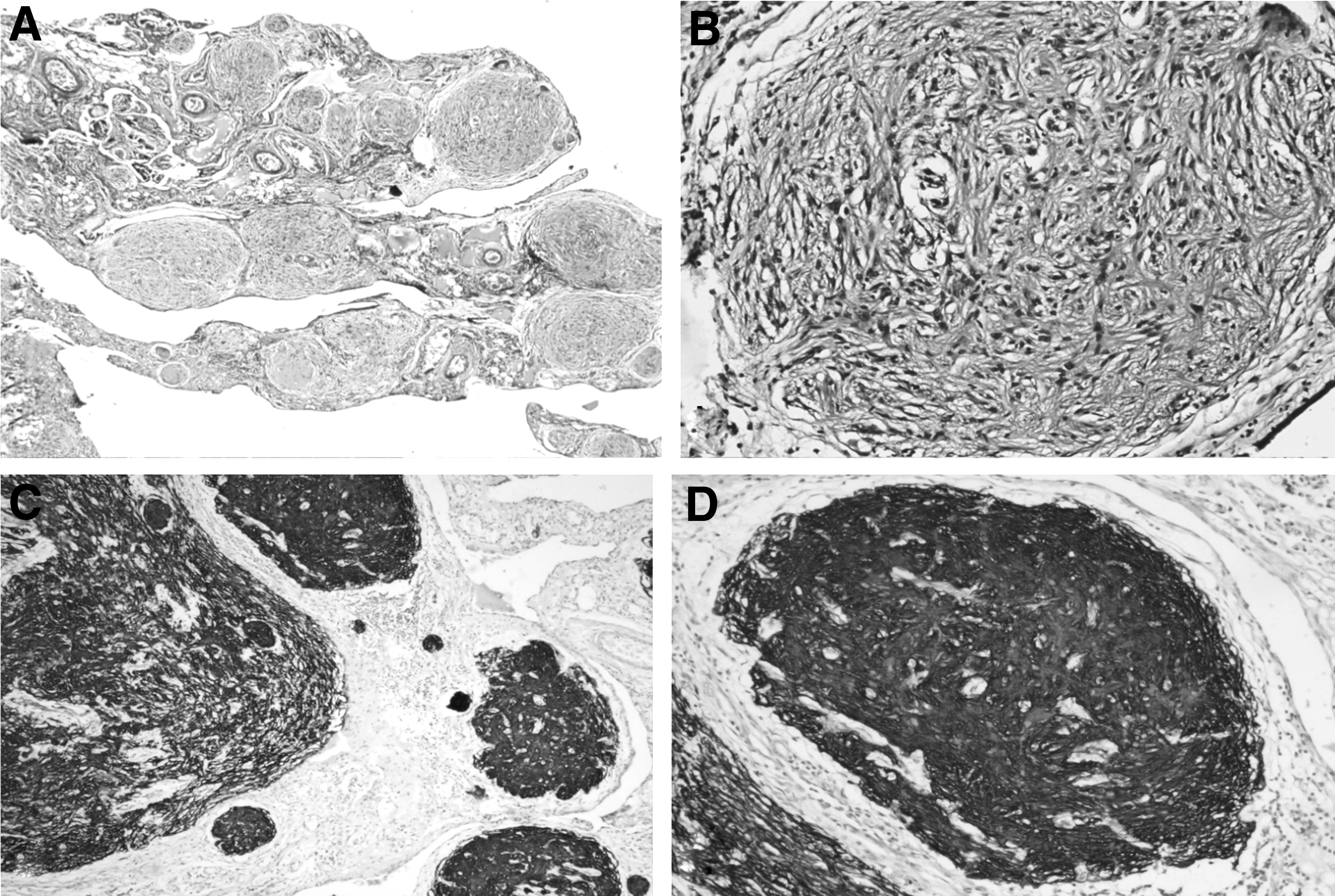
Grossly, the left adnexal mass measured 16 × 11 × 7 cm. The outer surface was intact and lobulated. The cut section showed a predominant solid component (90%) and multilocular cystic components (10%). The solid areas had a variegated appearance. Additionally, hair shafts, and cartilagenous and calcified areas were also identified (Fig. 1A). The omentectomy specimen measured 10 × 6 × 2 cm. No tumor deposits could be identified. Hematoxylin and eosin–stained sections from the tumor showed tissues arising from all three germ-cell layers, including mature glial tissue, ganglion cells, smooth muscle, adipose tissue, and gastrointestinal-lining epithelium. Immature neuroepithelial tissue was identified in multiple foci, in a low-power field, in multiple sections examined (Fig. 1B–D). Sections from the omentum showed well-circumscribed nodules of mature glial tissue. No immature tissue was identified. Immunohistochemical staining for glial fibrillary acidic protein (GFAP) revealed strong diffuse cytoplasmic positivity in the glial cells (Fig. 2). Based on these histopathologic and immunohistochemical findings, a diagnosis of an immature teratoma, WHO Grade III, with gliomatosis peritonei was rendered.

Results
The patient's symptom of abdominal pain was relieved, and she is being followed-up regularly.
Discussion
Gliomatosis peritonei is an uncommon disease characterized by multifocal peritoneal and omental implants composed entirely of mature glial tissue. The condition is most commonly seen in association with ovarian teratomas, especially immature ovarian teratomas. To date, fewer than 100 cases have been reported in the literature.3,4 Two theories have been proposed to explain the histogenesis of gliomatosis peritonei. According to one theory, the primary teratoma itself gives rise to the peritoneal-glial implants, either by direct implantation after rupture of the tumor capsule or via angiolymphatic spreading.1,5 The other, more widely supported, theory suggests that these implants arise consequent to differentiation of the pluripotent Müllerian stem cells residing on the peritoneal surface or by differentiation of the subperitoneal mesenchymal cells. 6
Radiologically, as well as intraoperatively, the tiny, well-circumscribed, disseminated peritoneal nodules might be misdiagnosed as peritoneal carcinomatosis or peritoneal tuberculosis. 7 Within the last 3 years, 2 studies highlighted that these deposits show contrast enhancement and intense 18F-fluorodeoxyglucose (FDG) avidity, and can be misdiagnosed on positron emission tomography as metastases from immature teratomas; hence, gliomatosis peritonei needs to considered as a differential while dealing with such cases.8,9
A definitive diagnosis requires histopathologic examination and positive immunohistochemical staining with neural markers, such as GFAP, neuron-specific enolase, or S100, to confirm the glial nature of the implants. Under the microscope, the implants of gliomatosis peritonei resemble benign, mature glial tissue with delicate fibrillary processes. Malignant transformation is extremely infrequent.10,11 The differentiation of peritoneal implants is important for establishing a prognosis. Therefore, extensive sampling of all peritoneal implants is crucial. If the implants do not show any teratomatous elements or malignant glial tissue, the mature glial implants can be disregarded, and the method of therapy should be decided according to the stage and grade of the primary ovarian teratoma. However, if immature glial tissue, or other teratomatous components, or both are present in the peritoneum or omentum, the treatment should be the same as that for a metastatic ovarian teratoma.
Treatment is mainly directed by the grade of the primary tumor, and many surgeons find complete resection of gliomatosis peritonei implants difficult. A more-conservative surgical approach is preferred for patients with extensive peritoneal spreading after exclusion of metastatic immature elements to minimize postoperative intra-abdominal adhesions. Residual peritoneal disease in gliomatosis peritonei could remain asymptomatic and quiescent over a long period of time, and these nodules could undergo spontaneous fibrosis and regression. However, in view of the risk of recurrence and malignant transformation in gliomatosis peritonei, long-term follow-up is obligatory for such patients. 2 The prognosis of gliomatosis peritonei is extremely favorable. As gliomatosis peritonei is always present with multifocal peritoneal implantation, optimal resection is tedious. A more-conservative surgical approach may be taken for patients with massive peritoneal spreading. 12 Although residual peritoneal disease can be totally quiescent over a long period of time, long-term follow-up is mandatory for patients with residual disease.
Conclusions
Gliomatosis peritonei is a rare condition seen mostly in association with immature teratomas. It presents with disseminated deposits over the omentum and peritoneum and can mimic peritoneal carcinomatosis or peritoneal tuberculosis. Differentiating gliomatosis peritonei from peritoneal tuberculosis, as well as from peritoneal carcinomatosis, is important, as the prognosis for gliomatosis peritonei is excellent. Establishing a definite diagnosis requires histopathologic examination and immunohistochemical confirmation of the glial nature of the cells. Extensive sampling and careful histopathologic examination is essential to exclude the possibility of a metastatic immature teratoma.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.