
Abstract
Background:
Ovarian cysts are more common in adolescents than has been assumed. Large ovarian cysts, however, are rare. Conventionally, large ovarian cysts have been managed by laparotomy. Laparoscopy has advantages of minimal bleeding, minimal postoperative pain, early recovery, and minimal scarring.
Case:
A 14-year-old Omani adolescent female had bilateral ovarian cysts, the larger of which had twisted and, owing to its size, had induced hydronephrosis. A laparoscopic cystectomy was performed with preservation of this patient's ovaries.
Results:
Less than 50 mL of blood was lost during the entire procedure. The patient was discharged in good condition on the second postoperative day. A histopathologic examination showed the specimen was a serous cystadenoma. There was no evidence of cellular atypia.
Conclusions:
The maximum size of ovarian cysts that can be treated with laparoscopy has not been determined. However, with proper selection of cases, cyst size cannot be a limitation for laparoscopic surgery.
Introduction
Widespread use of imaging facilities such as ultrasonography (USG), computed tomography (CT), and magnetic resonance imaging (MRI) have increased detection rates of ovarian cysts in pediatric and adolescent children, suggesting that these cysts are more common than has been assumed.
The majority of cysts in prepubertal and adolescent females are benign, with the most-common being mucinous cystadenomas, mature teratomas, and serous cystadenomas. Large ovarian cysts—defined as ≥15 cm—are very rare. The incidence of large ovarian cysts (> than 5 cm) in adolescents is 15.1%. 1 Laparoscopic surgery is preferred to minimize postoperative pain as well as achieving shorter hospital stays, minimal bleeding, and better cosmetic acceptance. In pediatric and adolescent patients, however, it can be challenging to manage a giant ovarian cyst laparoscopically due to a potential risk of cyst rupture owing to the restricted operating field.
This article presents a case of bilateral ovarian cysts in an adolescent wherein one of the cysts underwent torsions leading to hydronephrosis due to the cyst's sheer large size; this was a rare entity. Ovarian cystectomy was performed through laparoscopy and the patient's ovary was reconstructed.
Case
A 14-year-old Omani girl presented to the obstetrics emergency department with pain and constipation for 2 days. The pain was localized to her right loin area.
An examination revealed a distended abdomen with a tense, mobile swelling in the abdomen extending from the pelvis to the xiphisternum. The swelling was tender on palpation. All of this patient's vital signs were within normal limits.
USG showed a very large, clear cyst occupying the whole abdomen. The ovaries could not be visualized separately. CT showed a large, thin-walled abdominopelvic lesion, measuring 35 × 22 × 13 cm (Figs. 1 and 2) with high-density fluid. This mass displaced adjacent structures. There was no evidence of any solid-enhancing component/calcification. The uterus and endometrium were normal; fluid was seen in endometrial cavity. The left ovary was not visible separately and a small follicular cyst (2.5 × 2.4 cm) was seen in the right ovary. Apart from bilateral hydroureteronephrosis, all other viscera were unremarkable. A routine laboratory workup and tumor markers were within normal limits.
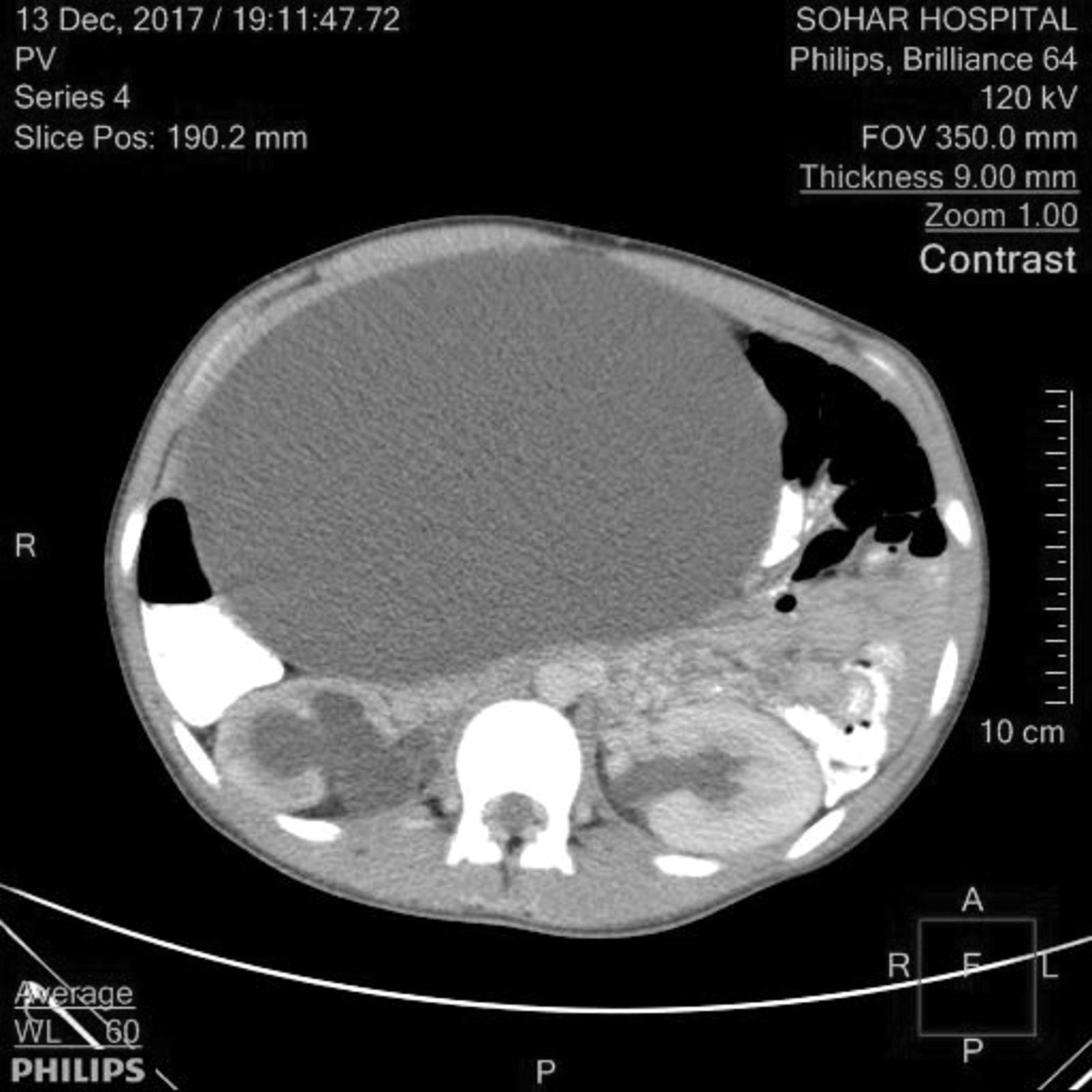
Computed tomography scan of the patient's mid-abdomen.
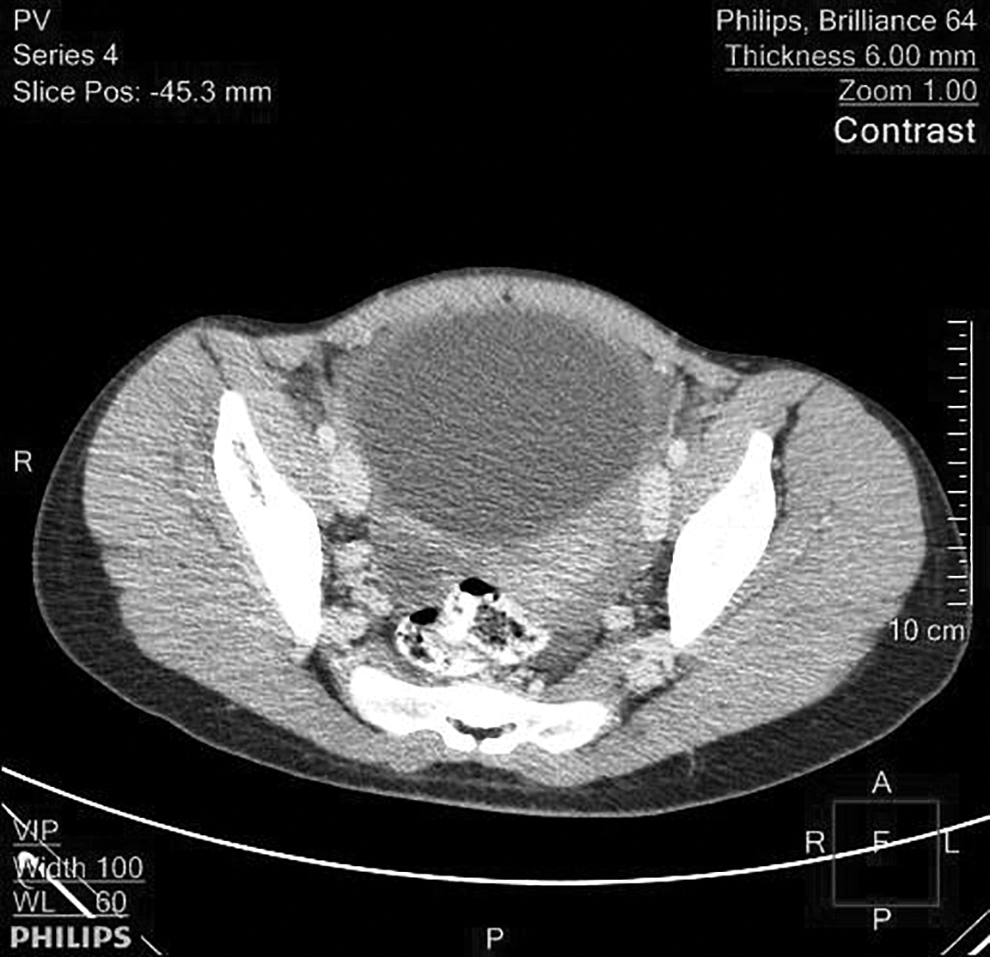
Computed tomography scan of the patient's pelvis.
Entry in abdomen was made through the Palmar point, using a 10-mm port. Two lateral 5 mm ports were also inserted, and then another 10-mm port was inserted in the umbilical area. An ovarian cyst (Fig. 3), emanating from the left ovary, was seen occupying almost the whole abdominal cavity. This cyst had undergone torsion ,twice (Fig. 4), which were corrected. The cyst wall was then punctured and, using suction nearly 6 L of clear fluid was aspirated. Despite the torsions caused by the cyst, the left ovary's blood circulation was normal. The cyst wall was peeled off and this ovary was reconstructed using endosutures. The specimen was removed, using an endobag. The right ovary was seen; it had a small clear cyst, which was punctured.
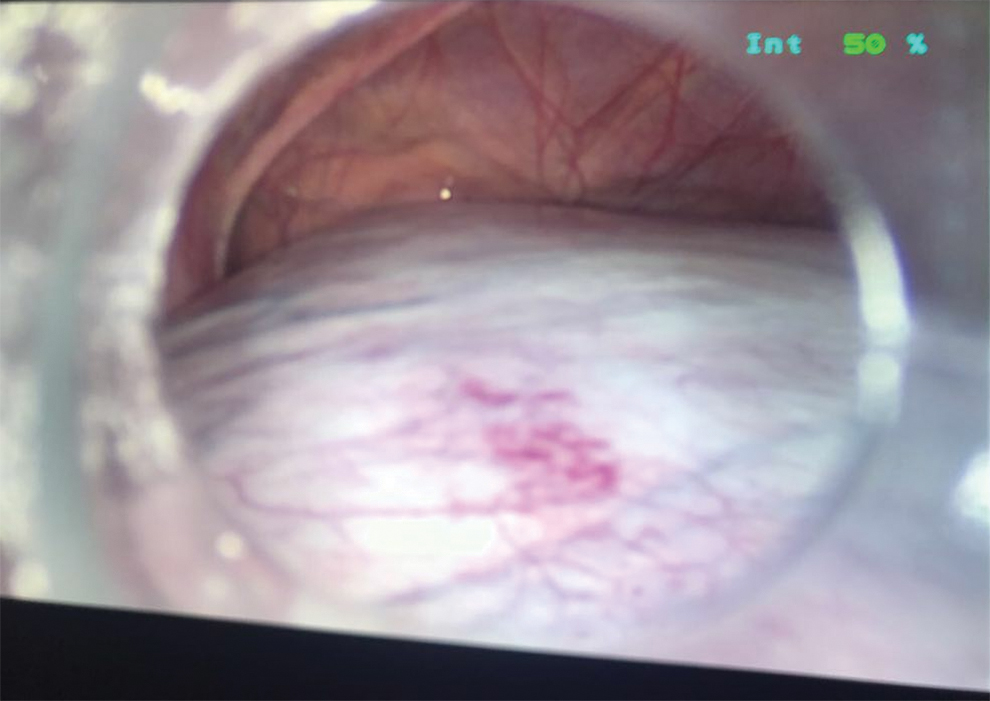
Panoramic view of the patient's giant ovarian cyst. Color images are available online.
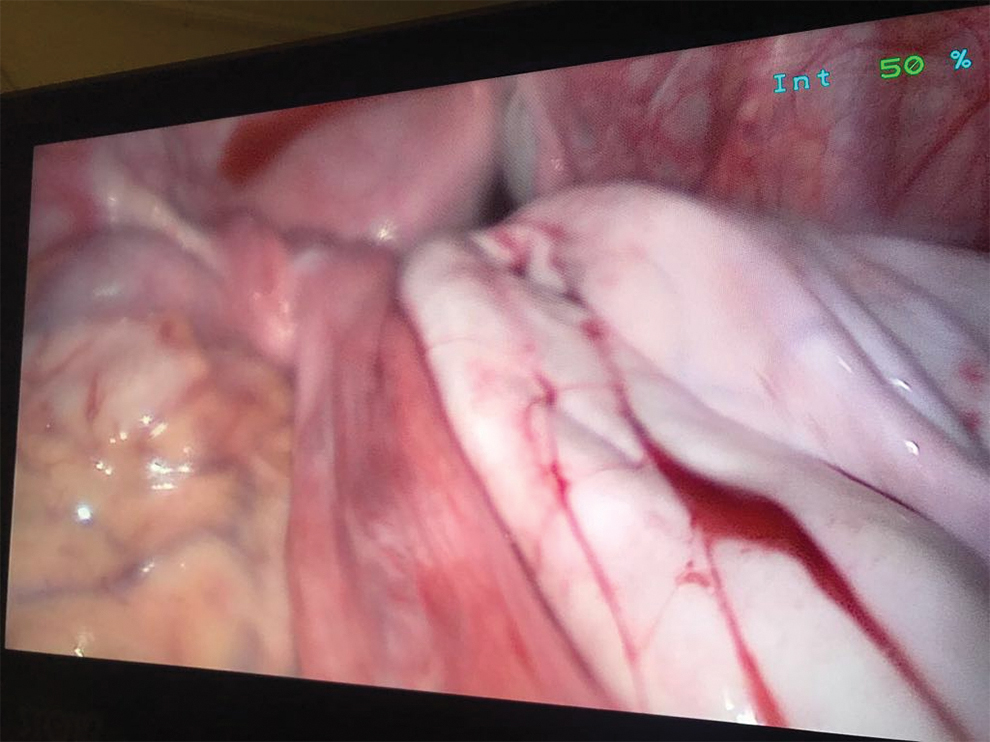
Cyst wall after aspiration; torsion is also visible. Color images are available online.
Results
Less than 50 mL of blood was lost during the entire procedure. This patient was discharged in good condition postoperative day 2. Histopathologic testing revealed that the cyst was a serous cystadenoma. There was no evidence of cellular atypia.
Discussion
Ovarian cysts are conventionally termed as large when they are >5 cm and giant or voluminous when they are >15 cm. 2 Giant ovarian cysts are very rarely seen and are often benign. A restricted operating field owing to its small surface area—particularly in adolescents—as well as the probability of malignancy and possibility of cyst rupture are critical points to be considered prior to choosing a laparoscopic approach to such cysts. The acknowledged modalities of management for giant cysts in adolescence are: (1) percutaneous drainage under USG guidance; (2) decompression with the help of a minilaparotomy and subsequent excision; (3) laparoscopic excision following USG-guided drainage. Potential leakage of the cyst contents into the abdominal cavity is a prominent complication associated with percutaneous USG-guided drainage; this is particularly hazardous if the cyst is malignant. Decompression of the cyst aided by a minilaparotomy and followed by excision is an alternative, but the origin of the cyst can be difficult to visualize in this procedure.
Diagnostic laparoscopy can be helpful in differentiating giant ovarian cysts from other intra-abdominal cystic growths. This procedure enables observation under direct vision and the growth's benign or malignant nature can be confirmed. If the situation so demands, this procedure can be converted to a laparotomy.
The advantages of laparoscopic surgery have been well-studied. Due to smaller incisions, this surgery results in fewer postoperative complications, early ambulation, early returns to normal routines, and reduced chances of deep-vein thrombosis and pulmonary embolism. Adhesions are not formed. Additionally, small laparoscopic scars are more cosmetically acceptable than larger scars. However, laparoscopic management of cystic ovarian lesions is not without its challenges. Large ovarian cysts can interfere with identification of ureters, bowels, the bladder and other important structures. 3
Few large cysts in adolescents have been documented earlier and even fewer reports of laparoscopic surgery for giant ovarian cysts in adolescence are available.2,4,5,6
The current case was unique not only in terms of the ovarian cysts, which were bilateral, but also because the patient presented with torsion of the larger cyst, which was compressing the ureter, leading to hydronephrosis. A maximum tumor size above which minimal access surgery is contraindicated has not been determined; nevertheless, with proper selection of cases, cyst size should not be contraindication to laparoscopic surgery.
Conclusions
Few reports5,7 have documented preservation of ovaries following laparoscopic cystectomies for giant cysts; in contrast, the majority of procedures for this are salpingo-oopherectomies/oophorectomies. The current patient's affected ovary in this case was salvaged, which is significant, as adolescents like this patient might want to have offspring later in life. Preservation of the ovaries will certainly improve patients' satisfaction postsurgery and quality of life as well as avoiding the risk of premature menopause in these individuals.
Footnotes
Acknowledgments
Approval for this report was granted by the hospital's regional research and ethics committee.
Author Disclosure Statement
No financial conflicts of interests exist.
Funding Information
No funding was received for this article.