
Abstract
Objective:
Placenta accreta is an abnormal implantation of the placenta, which often leads to postpartum bleeding. Cesarean hysterectomy is the most recommended procedure. However, more-conservative management is currently being investigated to maintain future fertility or uterus. This study was designed to describe a new systematic surgical technique for preserving the uterus while removing the abnormal placenta. Additional goals were to determine the characteristics and outcomes of this procedure.
Materials and Methods:
This approach involved corporal incision, hypogastric artery ligation, and using an ovarian and pericervical uterine tourniquet. Fifty-nine patients were enrolled in this cross-sectional study, with a median age of 29, ranging from ages 25 to 37. Eighteen of these patients (30.5%) were in their second pregnancy and had only 1 previous childbirth, 38 patients (64.4%) were in their third pregnancy, and 3 (5.1%) were in their forth pregnancy.
Results:
All patients had successful uterine preservation after the removal of their abnormal placentae. Median bleeding volume was 550 (range: 300–1200) mL. Bladder injury occurred in 1 patient.
Conclusions:
Using this systematic surgical technique and temporarily devascularizing the patients' uteri, it was possible to remove the abnormal placentae—without incurring massive bleeding—and then to reconstruct the uteri.
Introduction
Placenta accreta is a term used to describe abnormal placenta implants when placental villi are attached to the myometrium due to absence of the decidua basalis and a defective Nitabuch's layer. 1 Previous cesarean delivery is one of the major risk factors for placenta accreta. 2
Currently, there are two management options for the treatment of placenta accreta: (1) cesarean hysterectomy and (2) conservative treatment. Cesarean hysterectomy at the time of delivery is the recommended procedure for placenta accreta. 3 However, this procedure is associated with a significant risk of injury to the surrounding tissues (e.g., the genitourinary tract) and a potential for massive bleeding. Hysterectomy also means fertility loss and could be associated with some psychologic impacts. 4
In conservative management, the placenta might be left in situ and undergo spontaneous resorption. However, the term conservative does not mean a “no surgery” approach. Blood flow is decreased by utilizing pelvic arterial embolization or balloon-occlusion catheters. This conservative approach allows uterine conservation and future fertility whenever it is desired. However, conservative treatment may also be followed by an interval hysterectomy, either by an open surgical approach or by minimally invasive surgery. 5
In 2012, another alternative procedure was reported for managing placenta percreta. This technique—the Triple-P procedure—consists of
Massive bleeding can be prevented by uterine compression sutures, uterine balloon tamponades, and pelvic devascularization during such operations. 6 During pregnancy, the uterus obtains its blood supply primarily (90%) from the uterine arteries and the remaining 10% of the blood comes from the ovarian and vaginal arteries. Occlusion of the arteries will cause ischemia of the uterus. The mechanism of uterine arteries that lose the ability to constrict when uncontrolled bleeding occurs in placenta accreta is still unknown. 7 During this time, in order to overcome this condition, some researchers have described ligation of blood vessels in patients who have placenta accreta; however there has not been any report describing the effect of combined ligation of pelvic vessels to create temporary devascularization to the uterus.
In most cases, placenta accreta can only be known at the time of delivery, during the manual attempt to detach the placenta, which may cause serious postpartum hemorrhage that leads to complications, such as a need for massive blood products transfusion, as well as disseminated intravascular coagulation; acute renal failure; infectious morbidities; acute respiratory distress syndrome; and loss of fertility. The rate of mortality is as high as 7%. 8
Currently, the main goals for placenta accreta management are to maintain the uterine functions as best as possible, to prevent the possibility of bleeding, and to maintain fertility for subsequent pregnancies.
This study was designed to describe the surgical steps of an alternative conservative treatment of placenta accrete, involving hypogastric-artery ligation, utero–ovarian artery ligation, uterine devascularization, and use of a pericervical tourniquet. Another goal was to identify the characteristics and clinical outcomes of this procedure.
Materials and Methods
Ethical approval and consent to participate
Ethical approval was granted by the institutional review board of Hermina Maternal and Pediatric Hospital, in Depok, Indonesia. Written consent to participate was provided by each patient prior to undergoing the surgical procedure. Written informed consent was also obtained from each patient for publication of this article and its accompanying images.
Study design and subjects
This was a cross-sectional study of the alternative surgical technique introduced for pregnant women with placenta accreta. Subjects were patients who desired to preserve their fertility by maintaining their uteri and who were willing to undergo this new procedure. Diagnosis of placenta accreta was made prenatally using ultrasound (US) imaging. To be included in the study, the patients had to have at least 1 previous cesarean delivery.
A total of 59 patients were enrolled in this study; the median age was 29 years, ranging from 25 to 37. Eighteen of these patients (30.5%) were in each in a second pregnancy and had only a previous childbirth, 38 patients (64.4%) were each in a third pregnancy, and 3 of patients (5.1%) were each in a fourth pregnancy.
Cesarean delivery at 38 weeks of gestational age or more were planned for these patients at their preferred hospitals in Malaysia (Hermina Maternal and Pediatric Hospital in Depok; Siloam Hospital, in Bekasi; YPK Mandiri Hospital, in Jakarta; Harapan Kita Hospital, in Jakarta; and Hasanah Graha Afiah Hospital, in Depok. Surgery was performed by the author in all respective hospitals as an invited gynecologic consultant. All patients gave their written informed consent prior to surgery. Patient demographics are shown in Table 1.
Demographic Data of the Study Patients
Hospitals [all in Malaysia]: Siloam-B, Siloam Hospital, Bekasi; HMPH–D, Hermina Maternal and Pediatric Hospital, Depok; HKH-J, Harapan Kita Hospital, Jakarta; HGAH-D; Hasanah Graha Afiah Hospital, Depok; YPKMH-J, YPK Mandiri Hospital, Jakarta.
Pt., patient.
A contingency plan for emergency delivery before the planned date was made and included an institutional protocol for peripartum hemorrhage. Patients were also well-informed of the possibility of hysterectomy if the new surgery failed to stop massive bleeding whenever it occurs.
Surgical Technique
The author performed all surgical procedures.
Each patient was placed in a supine position under spinal anesthesia. Placental mapping and borders were identified carefully, using US, preoperatively or intraoperatively as needed. A midline vertical incision was made from the mons pubis to above the umbilicus just below the xyphoid process (Fig. 1). This choice of incision allowed sufficient exposure if a hysterectomy were needed. After that, a classical uterine incision was made through the central part of the uterus body (Fig. 2). Neonatal delivery was performed by classic cesarean section. This was performed high in the upper uterine segment, according to the placental mapping, avoiding the placenta and its edges (Fig. 3).

Illustration of median incision from the upper part of the pubic mound (mons pubis) to above the umbilicus just below the xiphoid process.
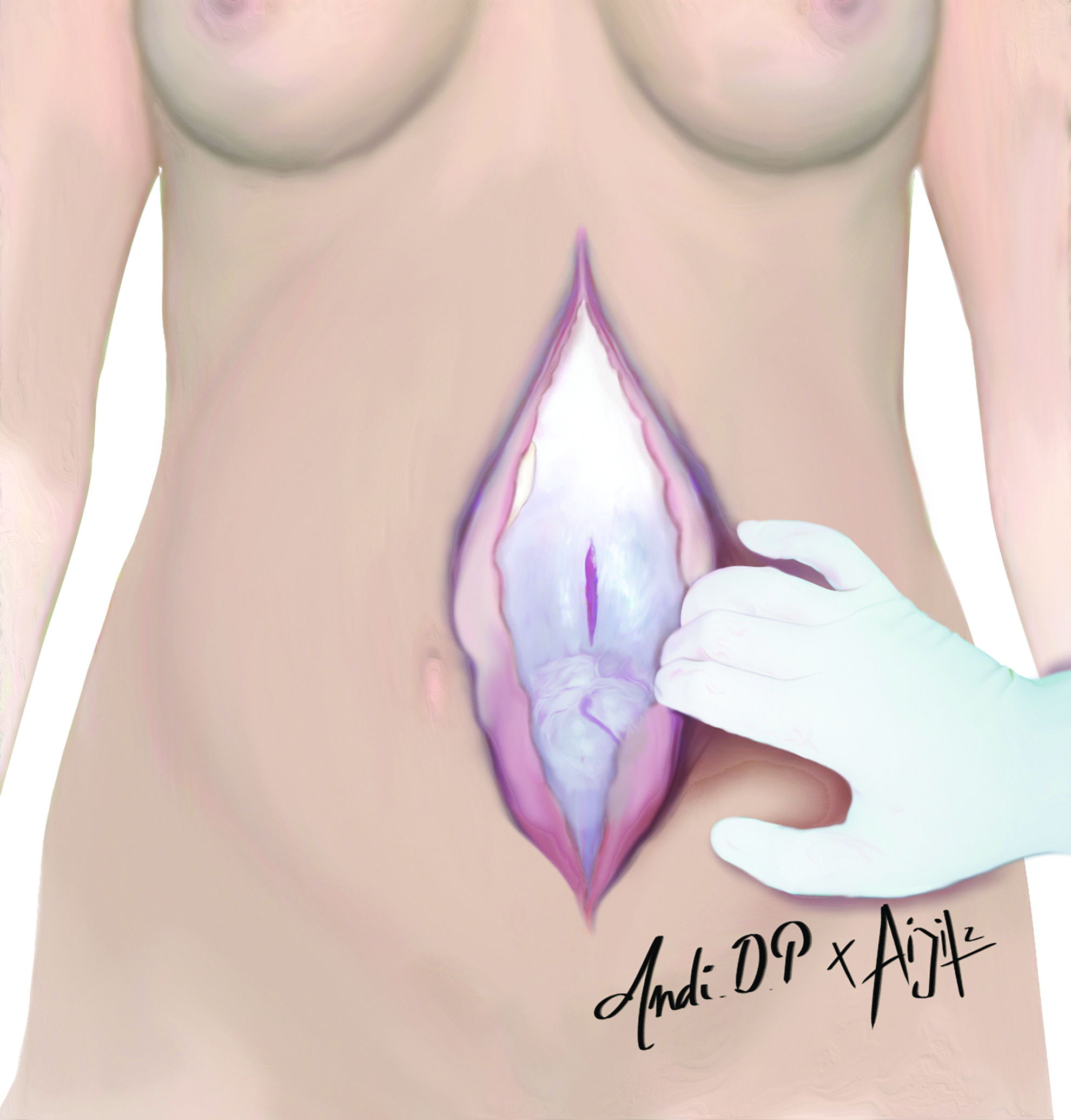
Illustration of classical uterine incision through the central part of the uterus body.

Illustration of neonate in the uterus that was delivered before removing placenta accreta.
For this procedure, a uterine incision was made to avoid any blood-vessel protrusion, because this might have been where the attachment of the placenta occurred, which is usually above the cervix. Once the neonate was delivered, the umbilical cord was clamped with Forester clamps to keep the placenta undisturbed in situ and reduce bleeding (Fig. 4).

Illustration of clamping the uterine muscles with Forester clamps to reduce bleeding.
The next step was to create pelvic devascularization by multiple ligations of the supplying arteries to the uterus: the bilateral hypogastric (iliac internal) vessels; the bilateral utero–ovarian vessels; or a utero–ovarian anastomosis; and by use of a pericervical tourniquet (Fig. 5). Selecting the first blood vessel to be ligated depended on each patient's condition. If there was heavy bleeding, the pericervical tourniquet was installed first. To ligate the hypogastric artery, it was recommended to first identify the ureter on the edge of the pelvis, and then incise the peritoneum from the point of bifurcation of the proximal common iliac artery along the external iliac artery caudally as far as ∼8 cm.
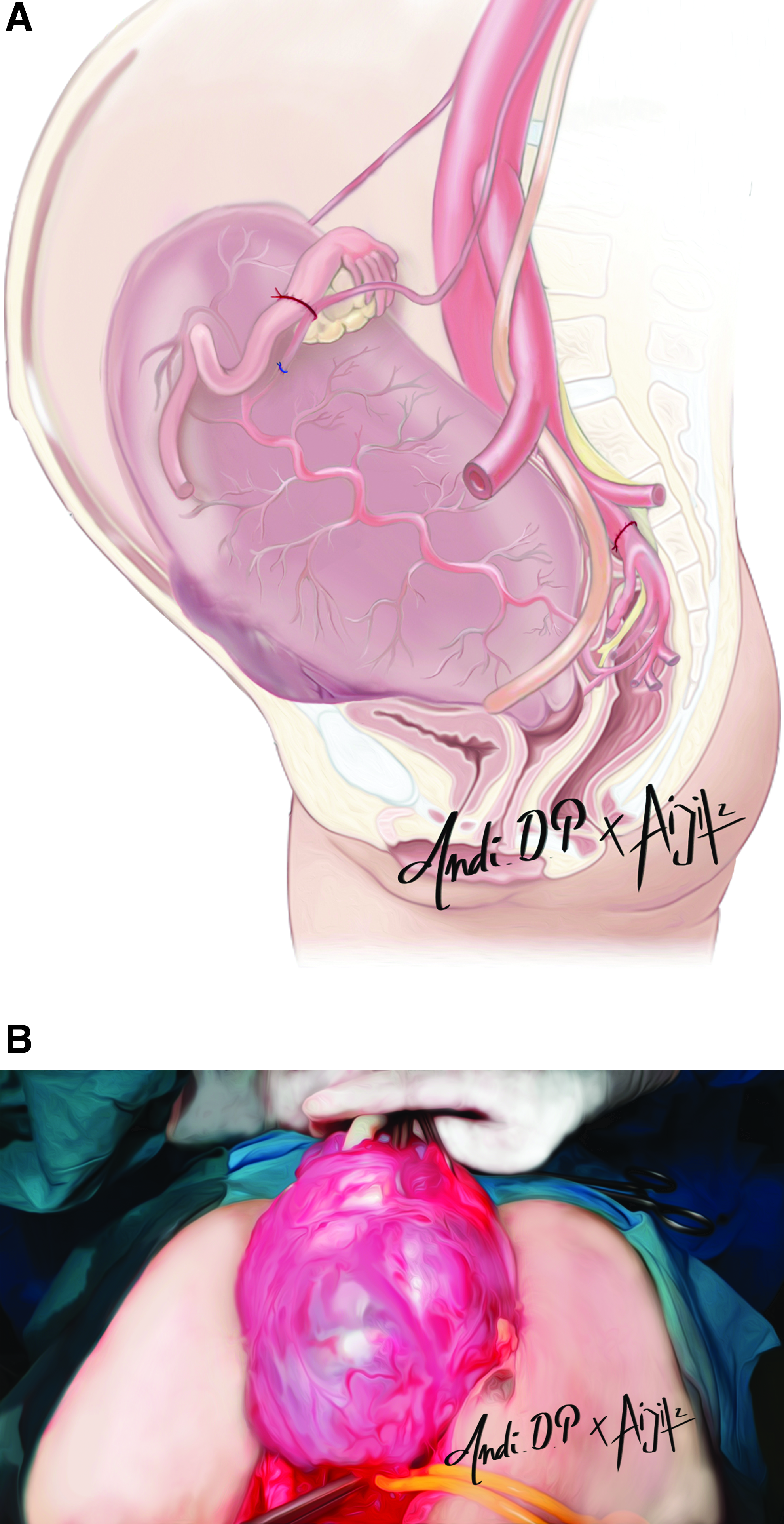
Visible bulging placenta.
Dissecting with the fingers or cutting the front part of broad ligament parallel to the infundibulopelvic ligament with scissors, the ureter was retracted medially to expose the retroperitoneal anatomy. There were fascia around the internal iliac artery. These fascia were cut thoroughly later, using a long hemostat to free the arteries from other structures that were attached and to ensure the connection between the internal iliac artery and the iliac vein. A 90° clamp was passed under the internal iliac artery from the lateral side to the medial side, right after the branching common iliac artery. The internal iliac artery was ligated singly using an absorbable suture (polyglycolic acid 1.0.; Safil®). Blood supplies from the uterine vessels and infundibulopelvic ligament were ligated using an absorbable suture (polyglycolic acid 2.0.; Safil).
A Foley's urethral catheter was used as a pericervical tourniquet. This tourniquet was placed at the base of the uterus close to the insertion of the uterosacral ligaments during the surgery. Also, during the surgery, sometimes this tourniquet was released intermittently (at ∼30-minute intervals) and removed after repair of the uterus. Before excision, the urinary bladder was lowered to separate it from the bulging placenta (Fig. 6).

Illustration of lowering the urinary bladder (arrow) to separate it from the bulging placenta.
The uterus was excised with the attached placenta accreta around the placenta's edge. It was necessary to do this 0.5–1 cm from the edge to avoid placental injury and massive bleeding (Fig. 7). The lower segment of the uterus was sutured, using polilyglycolic acid 2.0. After hemostasis was secured, a 24-Fr. Foley's catheter balloon was inflated with 50 mL of saline and inserted into the uterine cavity (Fig. 8).

Illustrations.

Catheter inserted into the abdominal cavity. Urine drainage port passed through the vaginal canal. Fixation of the catheter by suturing it to the skin.
The catheter tube was then passed through the vaginal canal. The catheter balloon was also used to also help press the lower-segment uterine suture and monitor intracavum uterine bleeding. The final step was uterine reconstruction and skin closure. Reconstruction of the lower segment of the uterus was made by suturing the isthmus to the uterus body (Fig. 9). Afterward, the pericervical tourniquet was released. A second catheter was then inserted into the abdominal cavity to assess intra-abdominal hemorrhage for the next 24 hours.
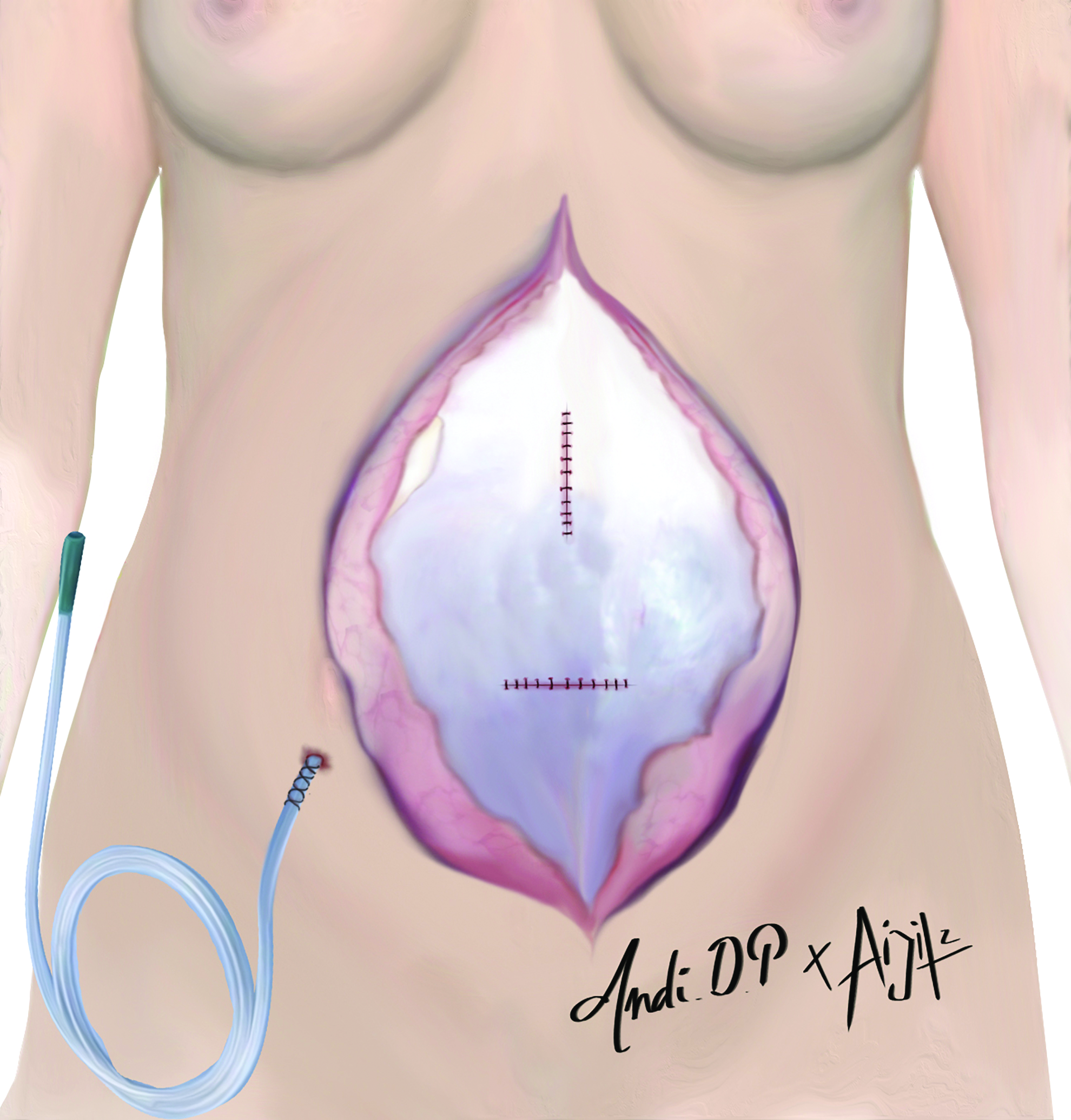
Uterine reconstruction and intra-abdominal drain placement.
The catheter tube was secured by suturing it to the skin (Fig. 8). Finally, a skin closure was performed similarly as usual. If monitoring revealed that the bleeding continued unabated or if there was another complication, a hysterectomy was performed to reduce morbidity and prevent death.
Results
Median bleeding volume was 550 (300–1200) mL. Bladder injury occurred in 1 patient. All patients had successful uterine preservation after removal of their abnormal placentae.
Discussion
This study tested a better, systematic surgical technique that allowed uterine preservation while removing abnormal placentae. By creating a temporarily devascularized uterus in each patient, the abnormal placenta was removed without causing massive bleeding; the uterus was then reconstructed.
This method can also be used on a placenta accreta that does not grow in the old cesarean incision.
The most common complication of placenta accreta is massive bleeding, with the average blood loss at the time of delivery of 3000–5500 mL. 3 Other complications that can occur are damage to the bladder, bowel, or ureters, including fistulae or incontinence.3,6 In the current author's hospital, before this technique was used, estimated blood loss (EBL) during such operations was ∼7000 mL.
The uterine arteries and the upper vesical arteries supply the blood flow to the uterine body, whereas the cervical arteries, the inferior vesical arteries, and the upper, middle, and lower vaginal arteries supply the lower segment. In general, the internal iliac, external iliac, and femoral systems are interconnected with the pelvic vascular system. 9 The internal and external compression of the abdominal aorta reduce the distal blood flow significantly. The compression is especially useful if there is active and uncontrolled bleeding due to the detachment of the placenta. The mechanism of the uterine-artery constriction when uncontrolled bleeding occurs is still not clear, and ligation is the definite and justifiable therapy. 9
Ligation, occlusion, or internal iliac artery embolization often fails to stop the bleeding of the placenta accreta. This is because the anastomosis to the artery is compensated rapidly. 9 Internal iliac artery occlusion reduces uterine blood flow by 49% and pulse pressure by 85%, generating pressure in the veins in the arterial circuit. 10
Occlusion or ligation of the uterine artery could be useless or insufficient in a case of a lower segment placental invasion. If the lower anastomosis system is occluded, necrosis is likely to result. Arterial embolization, followed by hemostatic procedures, such as ligation or compression, increase the risks of ischemic complications due to occlusion of the massive anastomosis components.
EBL as an indicator—or as a variable, in studies comparing complications that occur in placenta accreta—must be used with caution. For clinical purposes, measurement of postpartum hemoglobin and blood loss have low value and could lead to wrong conclusions. In this study, postpartum hemoglobin was not reported.
There are some changes opinions and actions taken in terms of treatment, from the historical cesarean hysterectomy to more-conservative methods of management involving uterine conservation and leaving the placenta in the uterus with—in some cases—adjuvant treatment with methotrexate or simply waiting for spontaneous resorption of the placenta. 11 By applying this new surgical approach, cesarean hysterectomy can be avoided and no further treatment would be required because the placenta had been completely removed. Further long-term study is needed to assess fertility preservation among these patients.
Conclusions
Conservative management of placenta accreta involving corporal incision; hypogastric artery ligation; and uterine, ovarian, and pericervical uterine tourniquets is a safe, fast, and effective method. This surgical approach is technically easier and may be used to avoid massive bleeding after delivery. The technique can also reduce other risks of postoperative complications related to hysterectomy and can maintain fertility for future pregnancies.
Footnotes
Acknowledgments
The author would like to thank the directors of the Rumah Sakit Dr. Cipto Mangunkusumo Hospital, Hermina Maternal and Pediatric Hospitals, Siloam Hospital, Sentra Medika Hospital, YPK Mandiri Hospital, Harapan Kita Hospital, and Hasanah Graha Afiah Hospital for their support in the preparation of this article. The author also acknowledges Aidil Z. for the illustrations.
Author Disclosure Statements
No financial conflicts of interest exist.