
Abstract
Objective:
The aim of this research was to compare the tolerance of 4% chlorhexidine gluconate (CHG)/isopropyl alcohol versus 7.5% povidone–iodine (PI) vaginal cleansing solutions in patients undergoing hysteroscopic procedures.
Materials and Methods:
For this randomized controlled trial at a university hospital, women at least 18 years old, who were undergoing diagnostic or operative hysteroscopy procedures, were randomized to either PI or CHG antiseptic as a vaginal preparation in a single-blinded fashion. The primary outcome was the presence and severity of vaginal dryness, vaginal burning, vaginal itching, unusual vaginal discharge, and burning or pain with urination. Patients completed a standardized survey at 3 timepoints: preoperatively (T0); immediately postoperatively (T1); and 24–48 hours postoperatively (T2).
Results:
Of 134 patients recruited and randomized, 123 (63 = PI, 60 = CHG) were analyzed at T0 and 97 patients completed all follow-up surveys. When controlling for age, menopause, catheterization, and T0 scores, patients treated with CHG had significantly higher rates of vaginal dryness (adjusted odds ratio (aOR): 4.38; 95% confidence interval (CI): 1.06–17.96; p = 0.042), vaginal burning (aOR: 6.45; 95% CI: 2.33–17.86; p < 0.001), and burning or pain with urination (aOR: 3.30; 95% CI: 1.18–9.19; p = 0.022). At T1, 54.2% of CHG versus 34.9% of PI patients had adverse symptoms. At T2, patients receiving CHG noted significantly more vaginal burning (aOR: 5.05; 95% CI: 1.85–13.78; p = 0.002), unusual discharge (aOR: 3.56; 95% CI: 1.13–11.26; p = 0.030), and burning or pain with urination (aOR: 4.78; 95% CI: 1.66–13.78; p = 0.004). At T2, 68.8% CHG versus 43.8% PI patients experienced adverse symptoms.
Conclusions:
Use of CHG vaginal preparation was associated with significantly worse vaginal and urinary symptoms, compared with PI, both in the immediate postoperative period and 24–48 hours postoperatively. Patients treated with CHG vaginal antiseptic for clean-contaminated gynecologic surgeries should be warned about the potential adverse side-effects.
Introduction
In recent years, interest in preventing surgical-site infections has grown, and the American College of Obstetricians and Gynecologists (ACOG) issued a Committee Opinion in 2013, 1 that was reaffirmed in 2018, highlighting this topic. 2 The authors of these Opinions advocated that a critical measure that should be taken preoperatively in one of the most common clean-contaminated surgeries performed by gynecologists—hysterectomy—is vaginal antisepsis. Although only povidone–iodine (PI) is approved by the U.S. Food and Drug Administration for vaginal antisepsis, the ACOG advocated that chlorhexidine with a low concentration of alcohol (4%) is both safe and effective for off-label use as a surgical antiseptic for the vagina.1,2 One can apply these same recommendations to more-minor clean-contaminated procedures that breach the endocervix, such as hysteroscopy, when vaginal antisepsis was similarly recommended. 2
Chlorhexidine–alcohol has been used safely for more than 40 years, and given that studies have shown that chlorhexidine–alcohol is more efficacious than PI for preventing deep or superficial surgical-site infections, 3 many surgeons are now using chlorhexidine with a low concentration of alcohol as their vaginal antiseptic of choice prior to hysteroscopy. However, manufacturers caution against using the product in genital areas, as the solution can cause irritation and sensitization. Although the antiseptic properties of chlorhexidine–alcohol and PI have been studied, the tolerance of the vaginal milieu to chlorhexidine–alcohol and PI preparations has not yet been studied rigorously as a primary outcome. Thus, the current authors conducted a randomized control trial (RCT) comparing the tolerance to these two antiseptic preparations at the time of hysteroscopic procedures.
Materials and Methods
This single-center, single-blinded RCT was approved by the Northwestern University Institutional Review Board (IRB; No. STU00204759), as well as by ClinicalTrials.gov (date of registration: October 9, 2017; Clinical trial identification number: NCT03305159).*.
Women at least age 18, who were undergoing diagnostic or operative hysteroscopy procedures were recruited at the Northwestern Prentice Women's Hospital. Women were excluded if they were pregnant or if they had active atopic dermatitis, any known chronic vulvovaginal disorder, or previous allergic reactions or anaphylaxis to chlorhexidine or PI. Women were also excluded if they were undergoing dilatation and curettage for a pregnancy-related reason or if they were undergoing concurrent nonhysteroscopic procedures at the time of surgery.
All participating women provided informed consents and underwent a standardized preoperative history taking, including demographics, pregnancies, comorbidities, medications, menopausal status, and the presence of vaginal or urinary symptoms prior to surgery. Participants were randomized using a computer-generated system on the day of surgery by a study member to receive either 7.5% PI (Purdue Products, Stamford, CT) or 4% chlorhexidine gluconate (CHG)/4% isopropyl alcohol treatment (CareFusion, Vernon Hills, IL) for surgical preparation of their vaginas. All hysteroscopies took place in an operating room suite with anesthesia. Vaginal preparation was performed in the standard manner by physicians or experienced operating room staff, with 3–5 internal sponges used. No sterile water rinsing was performed. Participants were blinded to treatment allocation, but the surgeons were not blinded, given that it would be obvious to the surgeon what type of preparation would be used due to the difference in color between both preparations. Both antiseptic solutions are approved for surgical preparation of the vagina at Northwestern's Prentice Women's Hospital.
The objective of the study was to compare the tolerance to CHG versus PI vaginal cleansing preparations by determining if there were any differences in vaginal and urinary symptoms after surgery. The current authors hypothesized that the CHG would result in more vaginal and urinary irritation than the PI. In order to assess tolerance, patient surveys were administered. The survey of vaginal and urinary symptoms used in this study was designed using the PRO-CTCAE [Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events] created by the National Institute of Health and National Cancer Institute. 4 A sample of the preoperative (T0) survey is shown in Appendix 1. The PRO-CTCAE is a measurement system used in cancer clinical trials to detect symptomatic adverse events. The language and format of the PTO-CTCAE questions have been tested cognitively. Questions on vaginal burning and itching were investigator-developed items using similar language as the PRO-CTCAE, given that these adverse events were not contained in the PRO-CTCAE item library.
The primary outcome of the study was to determine and compare the frequency in which women selected “none,” “mild,” “moderate,” “severe,” or “very severe” for each of the 6 questions regarding vaginal dryness, vaginal burning, vaginal itching, unusual vaginal discharge, pain or burning with urination, or any other symptoms that they wished to report for both antiseptics. To minimize bias, a study member, separate from the medical team, administered the survey questions regarding vaginal and urinary symptoms. Surveys were given at 3 timepoints: preoperatively (T0); immediately postoperatively (T1); and 24–48 hours postoperatively (T2). The T0 surveys were administered in person prior to the procedure, and the T1 surveys were administered in person after the patient had awakened from anesthesia postprocedure but prior to discharge. The T2 survey was administered over the telephone at the times the patients chose as most convenient between 24–48 hours postoperatively. Survey responses were analyzed as binary variables (symptom present versus symptom not present), as well as ordinal variables with total composite scores calculated as none (0 points), mild/moderate (1 point), or severe/very severe (2 points) for each outcome.
Based on prior literature demonstrating medication-related vaginal and urinary symptom effect sizes between 7 and 15 percentage points, an 18 percentage-point effect size was desired. 5 It was calculated that a sample size of 57 women in each study arm would be needed to demonstrate an 18 percentage-point difference in patient-reported vaginal and urinary symptoms at 80% power with a 2-sided α of 0.05.
All data analyses and statistical processes were performed using SAS version 9.4 (SAS Institute, Cary, NC). Data were analyzed in a per-protocol manner. χ 2 tests of association and two sample t-tests were used to compare baseline characteristics between the 2 randomized PI- and CHG-treated groups. Fisher's exact test was used to test the association between the treatment groups and baseline characteristics with low cell counts. Adjusted odds ratios (aORs), controlling for age, menopause, catheterization, and T0 scores were calculated using binary logistic regression to determine if there was a statistical difference between the 2 treatment groups for each outcome at each timepoint. Additionally, each survey was given a total composite score. Simple and multiple linear regressions were used to test the association of the treatment and the total composite scores at T1 and T2. A 2-sided p-value of ≤0.05 was taken to indicate statistical significance for all hypothesis tests.
Results
From August 2017 to April 2018, 134 patients were randomized (PI: n = 66; CHG: n = 68). After exclusion for procedural factors causing ineligibility, 63 PI patients and 60 CHG patients were analyzed at T0. A total of 122 and 97 patients completed surveys for analysis at T1 and T2, respectively; 26 patients were lost to follow-up from T0 to T2 (Fig. 1). The baseline characteristics of the 2 randomized groups are shown in Table 1. Demographic characteristics were similar between the groups. Baseline vaginal and urinary symptoms were similar, other than an increased baseline presence of unusual vaginal discharge in the PI group. Of note, there were no differences in type of anesthesia and bladder catheterization use between the 2 groups.
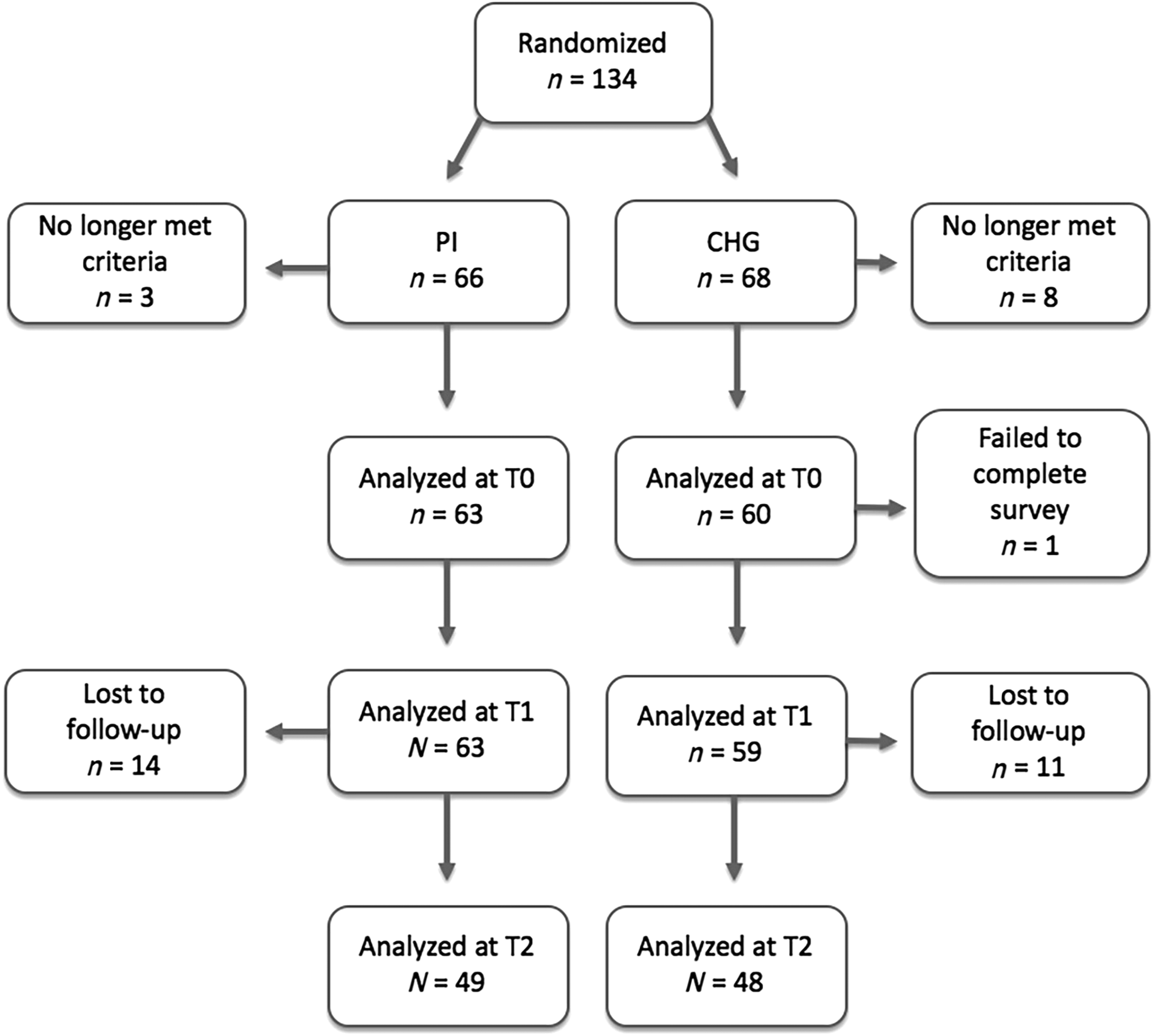
Recruitment flow diagram. Of 134 patients recruited, 11 were excluded from further participastion in the study for failure to meet demographic and procedure-related study inclusion criteria. PI, povidone iodine group; CHG, chlorhexidine gluconate group; T0, immediately preoperatively; T1, immediately postoperatively; T2, 24–48 hours postoperatively.
Baseline & Perioperative Characteristics
Data are mean ± standard deviation or n (%) unless otherwise specified.
Parity is described as median (range).
All p-values are from Pearson's χ 2 unless otherwise specified.
p-Value from t test; †P-Value from Fisher's exact test.
Bolded values are significant at p < 0.05.
PI, povidone–iodine; CHG, chlorhexidine gluconate; yr, years; MAC with Local, monitored anesthesia care with local anesthesia.
Figure 2 and Table 2 summarize the results of these patient-reported outcomes between the 2 groups at T1 and T2. Of note, at T1, patients treated with CHG were significantly more likely than patients treated with PI to experience vaginal dryness (18.6% versus 6.4%; aOR: 4.38; 95% confidence interval (CI): 1.06–17.96; p = 0.042), vaginal burning (42.3% versus 12.7%; aOR: 6.45; 95% CI: 2.33–17.86; p = < 0.001), and pain with urination (28.8% versus 14.3%; aOR: 3.30; 95% CI: 1.18–9.19; p = 0.022). In total, at T1, 54.2% of CHG patients versus 34.9% of PI patients had adverse symptoms. At T2, patients receiving CHG were more likely than patients receiving PI to note vaginal burning (47.9% versus 18.3%; aOR: 5.05; 95% CI: 1.85–13.78; p = 0.002), pain with urination (41.7% versus 18.3%; aOR: 4.78; 95% CI: 1.66–13.78; p = 0.004), and unusual discharge (29.2% versus 12.5%; aOR: 3.56; 95% CI: 1.13–11.26; p = 0.030). In total, at T2, 68.8% CHG versus 43.8% PI patients experienced adverse symptoms.

Vaginal and urinary sympton differences (%) between patients treated with povidone–iodine (PI, black bars) versus chlorhexidine CHG, gray bars) immediately postoperatively
Unadjusted & Adjusted ORs for Vaginal & Urinary Symptoms in CHG Group, Compared to PI Group Immediately & 24–48 Hours Postoperatively
Adjusted for age, menopausal status, intraoperative bladder catheterization, & baseline (T0) scores.
Bolded values are significant at p < 0.05.
OR, odds ratio; CHG, chlorhexidine gluconate, PI, povidone–iodine; CI, confidence interval; T1, immediately postoperatively; T2, 24–48 hours postoperatively.
At T0, there was no difference in total survey scores between the PI and CHG treatment. However, treatment with CHG, compared to PI treatment, was significantly associated with worse total scores at both T1 (p = < 0.01) and T2 (p = < 0.01; Table 3).
Unadjusted & Adjusted Correlations for Total Scores in CHG Group, Compared to PI Group Immediately & 24–48 Hours Postoperatively
Adjusted for age, menopausal status, intraoperative bladder catheterization, and baseline (T0) scores
Bolded values are significant at p < 0.05
CHG, chlorhexidine gluconate; PI, povidone-iodine; T1, immediately postoperatively; T2, 24-48 hours postoperatively.
Overall, there were few additional patient-reported symptoms noted with both PI and CHG. One participant treated with PI developed a moderate rash and another participant reported severely swollen oral lips. Two participants treated with CHG for hysteroscopic myomectomy noted moderate and severe bleeding, respectively, and a third participant treated with CHG experienced severe swelling of the vulva immediately postoperatively that was reported to the IRB. Of note, no patients required inpatient admission and all symptoms were becoming reduced by 24–48 hours postoperatively. There were no surgical-site infections in either group.
Discussion
In this single-center, single-blinded RCT, the use of a 4% CHG vaginal preparation was associated with significantly worsened vaginal and urinary irritative symptoms, compared with a 7.5% PI preparation. This symptom difference existed in both immediately and 24–48 hours postoperatively. Specifically, CHG was associated with significantly worse vaginal burning and pain/burning with urination at both timepoints. Of note, neither antiseptic was associated with vaginal itching significantly.
These findings arise in the context of the ACOG guidelines approving the use of 4% CHG for vaginal surgical antisepsis prophylaxis. 1 These guidelines were extrapolated from a large randomized trial concluding that CHG skin preparations are twice as effective at preventing superficial surgical-site infections and three times as effective at preventing deep surgical-site infections as PI preparations. 3 It is important to note that this large trial analyzed only abdominal skin preparations as they relate to surgical-site infection in a variety of clean-contaminated procedures across specialties.
Surgical-site infections are publicly reported, significantly increase healthcare costs, and are the target of several quality initiatives.6–8 Deep or organ-space infections including cuff cellulitis, abscess, and peritonitis, occur in ∼1.1% of hysterectomies 9 ; these are associated with identifiable risk factors and are the most important targets of surgical-site infection reduction with abdominal and vaginal antisepsis. Notably, a recent large retrospective trial revealed lower rates of surgical-site infection after abdominal hysterectomy with CHG abdominal skin preparation, compared with a PI preparation. 10 Data on the implementation of a hysterectomy surgical-site infection prevention bundle including CHG vaginal antisepsis has been shown to reduce overall infectious morbidity from 4.5% to 1.8%. 11
However, only 1 RCT has specifically compared CHG and PI vaginal antiseptic preparations at vaginal hysterectomy. The authors found a significant decrease in “contaminated” intraoperative vaginal cultures after using a CHG preparation, but there was no difference in the incidence of postoperative infections or irritative symptoms in either group. 12 Thus, no rigorous evidence exists regarding of the superiority of a CHG vaginal preparation for preventing surgical-site infection at gynecologic surgery. Given the results of the current study, it would be prudent to reconsider these recommendations prior to further rigorous study. The current study specifically did not investigate surgical-site infections due to limited power, prior reports on this topic, and infections being rare after hysteroscopy. For instance, one study noted the prevalence of infection after hysteroscopy to be 0.06%. 13
In terms of adverse side-effects, it is important to highlight that irritative symptoms persisted at least 24–48 hours after surgery in a significant number of participants receiving both types of antisepsis and in two-thirds of patients receiving the CHG preparation. This could influence patients' postoperative comfort, relationships, and self-esteem substantially, as may be inferred from vulvovaginal atrophy literature. 14 Importantly, it is plausible that many participants' irritative symptoms persisted beyond the 1–2-day postoperative timeframe studied, influencing the participants' quality of life and relationships further. Additionally, the persistence of an unusual discharge in 20 patients at 24–48 hours after surgery overall might be a surrogate for vaginitis as a result of alteration of vaginal flora caused by either preparation. This has yet to be studied in detail. The irritating culprit of the CHG preparation might be the alcohol solution. 15 Most CHG skin preparations contain 70% alcohol. This study used a 4% alcoholic solution as recommended by the ACOG, but the results provided evidence that perhaps even a 4% alcohol solution is still too potent for the vaginal mucosa. Additional research is needed before this information can be confidently used in clinical settings.
Despite the number of studies comparing the antiseptic properties of CHG and PI, only one other study compared the tolerance to these 2 preparations. Al-Niaimi et al. found that the 2% CHG for preoperative vaginal antisepsis followed by sterile water rinses after surgery was not associated with increased irritation compared to PI. 16 Of note, the study only assessed vaginal irritation or burning at one timepoint the day after surgery. Moreover, there have also been numerous reports on the adverse effects of these antiseptics individually. CHG has been increasingly described to cause hypersensitivity reactions, such as contact dermatitis, contact urticaria, and anaphylaxis, especially when applied on mucosal surfaces.17–19 PI, although less often implicated, is also a source of hypersensitivity reactions and has been noted to cause anaphylaxis rarely after vaginal application. 20 Future steps should involve further studies comparing tolerance to these two preparations. 21
Strengths of this current study include its randomized design, as well as the ability to control for confounding factors, such as age, menopause, urethral catheterization, and baseline symptom scores. The study was limited by its single-blinded design, as physician blinding to vaginal preparation was not feasible. Many participants had mild-to-moderate symptoms at all timepoints, which may indicate a less severe impact on postoperative well-being. Furthermore, the present study included participants undergoing only hysteroscopic procedures. As is evidenced by a high percentage of participants with vaginal and urinary symptoms after both antiseptic preparations, these procedures themselves might certainly influence postoperative irritative symptoms. Additionally, the loss of follow-up, both immediately and 24–48 hours postoperatively, could have caused selection bias. Finally, although the CHG preparation performed less well in terms of patient subjective complaints, it is worth pointing out that these conclusions were not based on objective criteria, such as a confirmed hypersensitivity reaction suggestive of an allergy. Further studies are needed to examine vaginal and urinary symptoms specifically after the use of CHG preparations for hysterectomies of various routes.
Conclusions
Surgeons performing gynecologic procedures that require vaginal antiseptic prophylaxis who choose to use CHG should counsel their patients about the potential for postoperative vaginal and urinary symptoms. Rigorous studies are needed to demonstrate the efficacy of vaginal CHG preparations for preventing gynecologic surgical-site infections.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
This work was supported by the Albert B. Gerbie Professorship Fund.
Appendix 1: Sample of Survey Administered at T0 (Preoperatively)
Date ___/___/_____ Surgeon _____________ Participant ID ________________