
Abstract
Background:
Lower abdominal and pelvic pain frequently has nongynecologic causes, and diagnosis and treatment could be challenging. While gynecologic causes are common, careful consideration must be given to other etiologies as well, particularly gastrointestinal causes. The appendix is a frequent culprit. Even in the absence of gross appendicitis, the appendix can be a cause of chronic lower abdominal pain. The American College of Obstetricians and Gynecologists (ACOG) has issued a committee opinion stating that elective coincidental appendectomy during a gynecologic surgery may be beneficial in some circumstances.
Case:
A was a 43-year-old, gravida 6, para 6 woman underwent uncomplicated total vaginal hysterectomy and bilateral salpingectomy for abnormal uterine bleeding. Five weeks postoperatively, she developed right lower-quadrant (RLQ) pain of unclear etiology. Her symptoms did not respond to conservative management. She was taken back to the operating room for examination under anesthesia and diagnostic laparoscopy, at which time, no gynecologic etiology was found. Elective appendectomy was performed for the RLQ pain.
Results:
This patient's pain resolved. Pathologic examination of her appendix showed it contained an adult pinworm (Enterobius vermicularis). The patient and her close contacts were treated with albendazole.
Conclusions:
Gynecologists should consider atypical appendiceal pathology, including helminthic infections, in the differential diagnosis of chronic and subacute lower abdominal and pelvic pain. (J GYNECOL SURG 36:141)
Introduction
Lower abdominal and pelvic pain have a broad differentials in women, and diagnosis and treatment can be challenging. In particular, when a patient presents with new-onset symptoms after a hysterectomy, postoperative and gynecologic causes should be evaluated thoroughly. While gynecologic causes are common, careful consideration must be given to other etiologies as well, particularly gastrointestinal (GI) causes. The appendix is a frequent culprit. Even in the absence of gross appendicitis, the appendix can be a cause of chronic lower abdominal pain. 1 Occult appendiceal causes of chronic pain include chronic inflammation, appendiceal endometriosis, chronic or subacute bacterial infection (including tuberculosis), and helminthic infection, particularly with Enterobius spp. (pinworm). Elective appendectomy is an appropriate intervention for chronic right lower-abdominopelvic pain, as pain rates have been shown to decrease significantly postoperatively.2,3 Given these findings, the American College of Obstetricians and Gynecologists (ACOG) issued a committee opinion stating that elective coincidental appendectomy during gynecologic surgery may be beneficial in some circumstances, including exclusion of appendicitis in patients with complicated differential diagnoses, such as patients with chronic pelvic pain. 4
Case
This is the case of a multiparous female who underwent total vaginal hysterectomy for benign indications and who developed abdominopelvic pain postoperatively, which ultimately was ascribed to appendiceal helminthic infection. Institutional review board approval was not required for this case report. Informed consent regarding the usage of patient information for research and education purposes was obtained from the patient, and the ACOG patient consent form was also signed by the patient, prior to proceeding with the report.
This patient was a 43-year-old, gravida 6, para 6, Hispanic female, who had abnormal uterine bleeding that was attributed to adenomyosis and uterine leiomyoma. She underwent total vaginal hysterectomy (TVH), bilateral salpingectomy, and cystoscopy in July of 2017. Her surgical history was limited to an interval bilateral tubal ligation via a laparoscopic Filshie-clip application, and her obstetric history comprised of six uncomplicated spontaneous vaginal deliveries. Preoperative imaging included transvaginal ultrasound, which noted a 5-cm class 2 submucosal fibroid, a15-mm endometrial stripe, a 2.4-cm simple right ovarian cyst that was unchanged from prior imaging, and a normal cul de sac. Intraoperatively, no ovarian cysts or other abnormalities were noted. Her TVH with bilateral salpingectomy was uncomplicated, and she was discharged to go home in good condition. Surgical pathology testing showed adenomyosis and a 4.5-cm leiomyoma as well as bilateral fallopian tubes with no significant pathologic abnormality.
Five weeks postoperatively, this patient developed new vaginal spotting, an abnormal vaginal discharge, severe deep dyspareunia, and pain radiating from her pelvis to her right-lower quadrant (RLQ). She had no prior complaints of pelvic pain. She described this pain as crampy, colicky, and intermittent.
On evaluation in September of 2017, her abdominal examination was notable for RLQ tenderness, and a pelvic examination was severely limited by her intolerance to pain, which was a change from her preoperative visits. Her cuff was confirmed to be intact, but had a 1-cm area of tender, polypoid-appearing tissue on the inferior portion of the cuff. An attempted office biopsy was unsuccessful due to this patient's pain. No adnexal masses or other abnormalities were palpated on a bimanual examination. A vaginal wet mount revealed bacterial vaginosis, and she was treated with metronidazole. Laboratory studies including urinalysis yielded otherwise normal results, and the patient remained afebrile with normal vital signs. Her symptoms failed to be ameliorated with conservative management (metronidazole and pain medication). A pelvic ultrasound performed in November of 2017 showed surgical absence of the uterus and cervix, a right ovary with multiple simple cysts (the largest of which measured 2.8 × 2.8 × 2.6 cm), no adnexal masses, and a normal cul-de-sac. The left ovary abutted the vaginal cuff, and the patient had corresponding tenderness with pressure on this area; however, the ovary did not appear to be fixed to the cuff. Differential diagnoses for her symptoms included fallopian-tube prolapse through the vaginal cuff, ovarian adhesions, and/or granulation tissue.
Given the examination and imaging findings, her intolerance to an in-office examination, and persistent vaginal and RLQ pain, this patient was offered examination under anesthesia (EUA), diagnostic laparoscopy, adhesiolysis, cuff biopsy, possible cuff revision, and any other procedures as indicated.
On November 30, 2017, 4 months postoperative from her TVH, she was taken back to the operating room and underwent EUA, vaginal cuff biopsy, and diagnostic laparoscopy, as well as an appendectomy. On vaginal examination, the cuff was noted to be intact and overall normal-appearing, with the exception of a 1 × 1.5–cm fleshy hyperemic nodule at the inferior aspect of the cuff consistent with granulation tissue, which was removed. Diagnostic laparoscopy revealed normal-appearing ovaries not adherent to the cuff; surgical absence of the fallopian tubes with no tubal remnants noted; filmy adhesions of omentum and sigmoid colon to the vaginal cuff with no tethering of these organs to the cuff; and a normal-appearing vermiform appendix. There was no evidence of endometriosis or other abnormal or dense adhesive disease. Given her persistent RLQ pain and absence of evident pelvic or posthysterectomy etiology, the decision was made to perform an appendectomy. The gynecology team used a LigaSuretm device to cauterize and ligate the appendiceal blood vessels and dissect the appendix from its surrounding connective tissue, and an Endoloop® device to secure the appendiceal stump.
Results
The patient did well postoperatively and was discharged to go home on the day of the appendectomy. She returned to the clinic 1 week later, at which time, she reported complete resolution of her RLQ and pelvic pain. However, on review of her systems, she did report vulvar and perianal itching in the previous few weeks. Surgical pathology of the vaginal-cuff nodule revealed fragments of granulation tissue. The appendix revealed a degenerating adult Enterobius vermicularis (pinworm) within the appendiceal lumen, shown in Figures 1 and 2. No image of the gross pathology was available. These findings were reviewed with the patient. Perineal and anal examination, including a tape test, were performed in the clinic to evaluate for further pinworm infection. No ova or worms seen externally nor were they detected with the tape test. However, the test was limited due to performance during daytime clinic hours rather than in the evening. The patient and her close contacts were treated with albendazole based on these pathology results.

Vermiform appendix, stained with hematoxylin and eosin staining, showing cross-section of a degenerated Enterobius vermicularis.
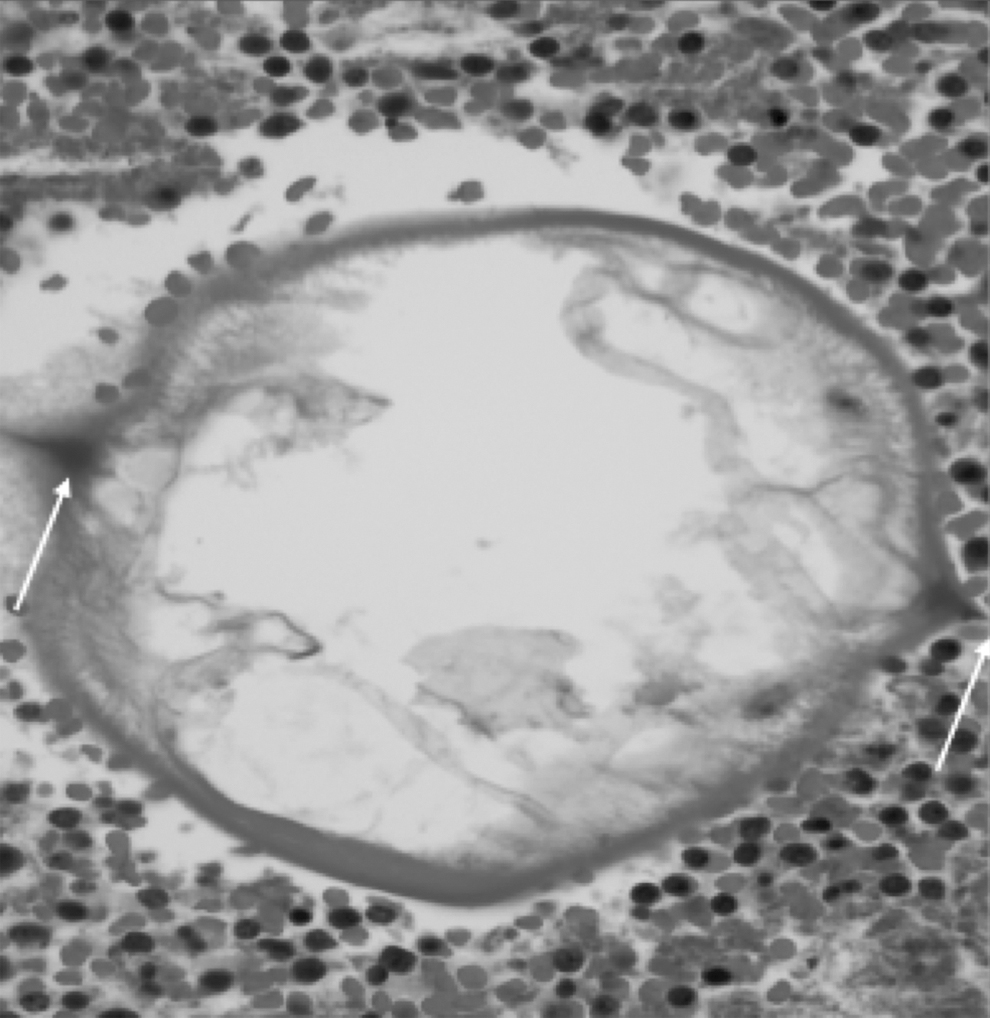
Enlarged, boxed portion of the degenerated Enterobius vermicularis from Figure 1. Note the prominent alae on either side of the helminth and surrounding eosiophilic infiltrate.
Discussion
The appendix is an established cause of RLQ pain, and can visually appear normal even if harboring infection or other pathology. As appendiceal pain can mimic that of gynecologic etiologies, gynecologists may be faced with diagnostic dilemmas, especially if there are no abnormalities visualized. In the current patient, the pinworm infection coincided with her postoperative course, and with no other GI symptoms, appendiceal pathology was low on the list of her differential diagnoses. This case illustrates an unusual cause of an appendiceal infection resulting in chronic lower-abdominal pain. However, a literature review showed that there were limited number of case reports, including 1 case series, of Enterobius infection of the appendix. 5 Although pinworms more commonly infect children, this possibility should not be overlooked in adults. In fact, there was 1 other case of chronic, intermittent, noncatamenial RLQ pain and dyspareunia in a young woman who underwent laparoscopic appendectomy and was found to have Enterobius in her appendix. 6
Conclusions
Based on a review of the literature, appendectomy in the setting of chronic lower-abdominal pain can have therapeutic and diagnostic results, even in the absence of grossly visible appendiceal abnormalities. Gynecologists should include atypical appendiceal pathology (including helminth infection) in differential diagnoses of chronic lower-abdominal and pelvic pain, and may perform elective coincidental appendectomy when appropriate. Regarding operative technique, the Endoloop technique, which gynecologic surgeons might have more experience with, has been shown to induce fewer postoperative complications than an endo-stapling device for securing the appendiceal stump. 7 However, for gynecologists unfamiliar with appendiceal surgery and who believe elective coincidental appendectomy is indicated, the current recommend enlisting the help of general surgery colleagues, whether as a planned combined case or for an intraoperative consultation.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Glorimar Rivera Colon, MD, who made the pathology diagnosis of the appendiceal enterobial infection and contributed slides for this case report. The authors would also like to acknowledge their patient, who has graciously allowed them to tell her story and, in doing so, contribute to the medical literature.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was obtained for this case report.